
The “Magneto View”: A Simple Method for Obtaining Intraoperative Axial Radiographs of the Calcaneus
Erik T. Newman, MD, Brian A. Kelly, MD, and Edward K. Rodriguez, MD, PhD
Disclosure Information©2015 by The Orthopaedic Journal at Harvard Medical School
 PDF
PDFBACKGROUND Displaced, intra-articular fractures of the calcaneus are often treated with open reduction and internal fixation, which relies on appropriate intraoperative imaging. Of particular importance is axial imaging of the calcaneus, namely the Harris view. However, obtaining the Harris view intraoperatively can be a challenge. We describe the “Magneto view,” a simple method for acquiring intraoperative axial views of the calcaneus.
TECHNIQUE Open reduction and internal fixation of the calcaneus is performed via a lateral approach with the patient in the lateral decubitus position. Both the x-ray source and the image intensifier of a standard C-arm are sterilely draped. To obtain the Harris view, the C-arm is rotated such that the beam is oriented parallel to the floor. With the surgeon standing in the center of the “C,” the base of the C-arm is advanced towards the posterior of the patient until the heel is adjacent to the x-ray source. Optimal axial imaging may then be obtained.
CONCLUSION The “Magneto View” is a simple and versatile technique for the acquisition of accurate intraoperative axial imaging of the calcaneus.
Fractures of the calcaneus are the most common fractures of the hindfoot, frequently presenting in young males following a high-energy axial load such as a fall from height.1 Two early observers, Cotton and Henderson, wrote in 1916 that “the man who breaks his heel bone is ‘done’, so far as his industrial future is concerned.”2 Fortunately, surgical and imaging techniques have improved; for patients with significantly displaced intra-articular fractures, operative treatment with open reduction and internal fixation (ORIF) now leads to superior outcomes as compared with conservative management.3,4
Accurate reduction and fixation of the calcaneus relies on appropriate intraoperative imaging. In particular, proper screw placement into the sustentaculum tali, avoidance of iatrogenic injuries to neurovascular structures at the medial hindfoot, and correction of varus deformity can be aided with proper axial imaging, namely the Harris view. However, this radiographic view can be particularly difficult to obtain intraoperatively due to positioning and overlapping structures of the foot. We present the “Magneto view,” a simple alternative method for obtaining high-quality intraoperative axial views of the calcaneus when performing ORIF through a standard lateral approach.
The patient is placed in the lateral decubitus position on a radiolucent table, with the affected extremity up. The well leg is placed in a straight leg position. With the use of multiple blankets or a foam pad placed on top of the contralateral limb, a stable platform is created under the operative extremity on which to perform the procedure. The knee of the operative leg can be bent so that lateral imaging avoids capturing the well leg. All bony prominences are well padded.
A single large C-arm fluoroscopy unit is required to obtain the necessary views. At the beginning of the procedure, the unit may be placed in any position convenient for the surgeon, but must be able to be maneuvered to the posterior side of the patient. We suggest that the base of the C-arm be brought in diagonally from the foot of the table. The monitor can be placed at the foot of the bed or anterior to the patient. Lateral images of the calcaneus can be obtained in the usual fashion, with the beam of the C-arm oriented perpendicular to the floor.
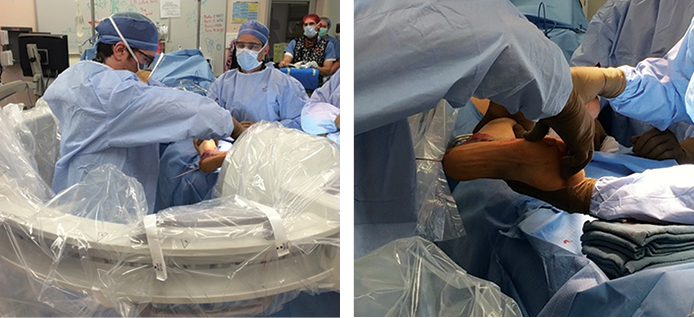
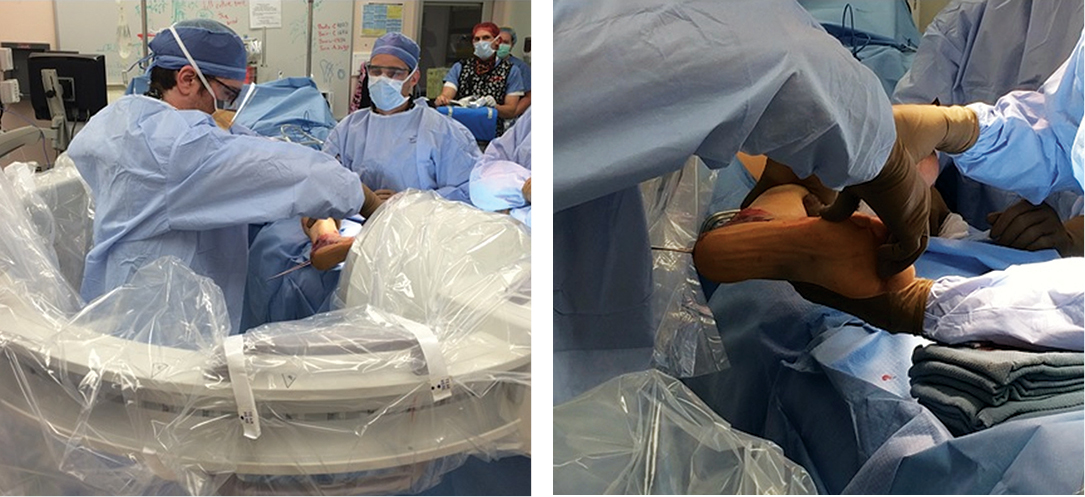
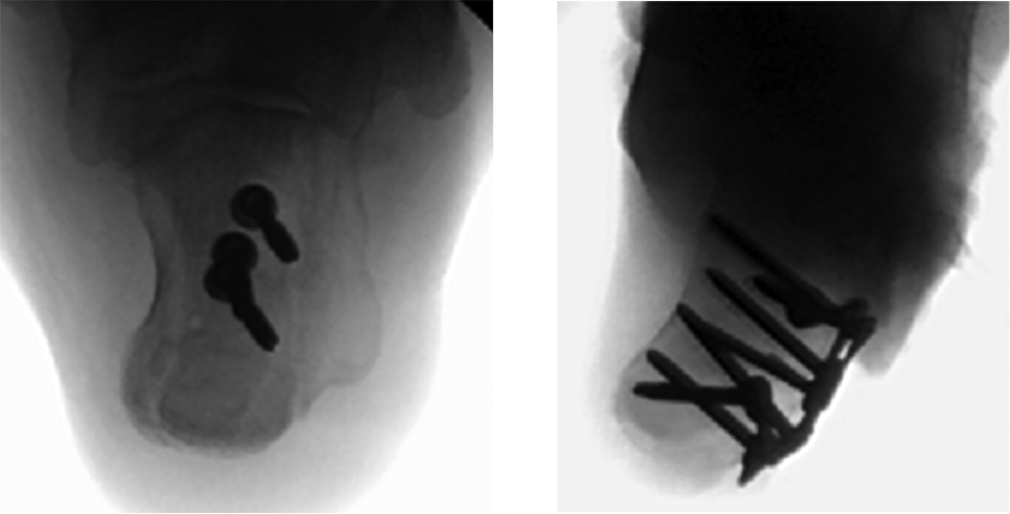
When axial imaging is needed, the C-arm is positioned posterior to the patient. The “C” is rotated 90 degrees such that the beam is oriented parallel to both the floor and the long axis of the patient, with the x-ray source towards the head of the patient and the intensifier towards the foot. Both the x-ray source and image intensifier are draped in a standard sterile fashion (Figure 1). The operating surgeon stands in the center of the “C”, between the x-ray source and intensifier, while the unit is advanced towards the patient (Figure 2); care is taken to maintain sterility at all times. To obtain the Harris view, the surgeon extends the hip and flexes the knee to place the heel adjacent to the x-ray source (Figure 3). The rotation of the “C” can be adjusted to optimize the view and obtain axial images at multiple angles, ensuring proper alignment of the heel and placement of the sustentacular screw (Figure 4).


Beam is parallel to both the floor and the long axis of the patient. C-arm is brought in from the posterior side of the patient; the operating surgeon stands in the center of the “C”.
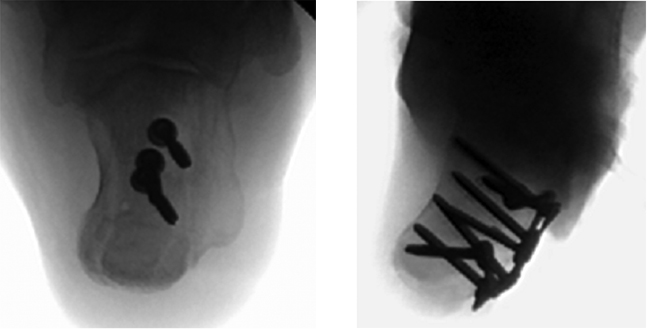
High-quality intraoperative imaging is essential in the fixation of intra-articular calcaneal fractures. Of particular importance is the sustentanculum tali, which is typically maintained in an anatomic position with respect to the medial talus. Fluoroscopic visualization of this so-called anteromedial “constant” fragment with the Harris view allows for accurate placement of screws and avoidance of medial penetration which puts neurovascular structures at risk. Additionally, a quality axial image confirms correct alignment of the heel.
The Harris view was first described in 1948 by Harris and Beath, as a method of assessing for the presence of a talocalcaneal bridge in a rigid flat foot deformity.5 An axial view of the calcaneus is obtained with the x-ray source posterior to the heel and tilted caudally ~45° with respect to the long axis of the foot. As applied to calcaneal fractures, the Harris view allows for assessment of subtalar joint displacement, angulation of the tuberosity fragment, increase in heel width, and residual calcaneal varus after reduction.
However, adjustment of projector angle in acquiring Harris views may be necessary intraoperatively. Essex-Lopresti noted in his initial classification of calcaneal fractures that reliance on a single axial view may not allow for accurate characterization of the subtalar joint: “Unless the rays strike the joint tangentially its outline will not show against the mass of spongy bone. Furthermore, if the joint is simply displaced downwards and forwards – that is, in the line of the X-ray tube – no deformity will be apparent.”2 More recently, a cadaveric study performed by Gitajn et al. found that the standard 35-45 degree Harris view may be inadequate in assessing placement of lateral-to-medial sustentacular screws.6 They noted that inferior screw misplacement, which could endanger the (FHL) and neurovascular bundle, was identifiable only on 10 and 20 degree views.
Several methods of obtaining axial images of the calcaneus in the operating room have been outlined. Typically, a single C-arm is used, with only the image intensifier draped. In a recent paper outlining percutaneous fixation techniques, for instance, Marsh et al. describe positioning the base of the C-arm at the foot of the bed, opposite the surgeon and at a 45 degree angle to the axis of the patient.7 To obtain Harris views in this configuration, the x-ray source is arced below the table until the beam is parallel to the floor. Abousayed et al. described a two C-arm technique for calcaneal fixation: with the patient in a lateral decubitus position, a standard C arm is utilized for lateral views, while a mini C-arm, oriented horizontally and positioned with the x-ray source just posterior to the calf, allows for variable-angle Harris views.8 Other authors have argued for the intraoperative use of three-dimensional imaging modalities.9,10 One report found that the use of a C-arm-based three-dimensional imaging device, following initial reduction and fixation with the aid of standard fluoroscopy, resulted in alteration of screw placement in 41% of cases, albeit at the expense of slightly longer operative times.10
Three drawbacks exist with this technique. First, positioning of the surgeon in between the x-ray source and image intensifier may result in slightly higher radiation exposure per fluoroscopy shot. However, we feel that this may be compensated by the decreased number of shots required given the accuracy afforded by this technique. Second, the extra maneuvering and draping necessary to position the c-arm correctly makes switching between views more time consuming, and slightly more expensive if multiple drapes are required. This can be minimized if an experienced X-ray technician is available. Additionally, we attempt to perform a majority of the procedure utilizing the lateral view, switching to the axial view to verify the heel alignment after provisional reduction has been obtained, and again after implants have been placed to ensure proper screw position. Finally, there are increased sterility concerns with the positioning of the surgeon. The surgeon and operating room staff need to be vigilant for any breaks in sterility when this method is used. We believe, however, the quality and ease of obtaining these images justifies these added risks and inconveniences.
The “Magneto view” described here represents a novel technique for positioning and use of the C-arm intraoperatively. By draping both the x-ray source and the image intensifier and standing in the center of the “C,” the surgeon has improved ability to adjust the angle of projection for axial views of the calcaneus, while maintaining unfettered access to the surgical field. In our experience, this is a simple way to obtain high quality images with the standard – as opposed to mini – C-arm, without the added time and expense of advanced imaging modalities.





{kind=link}
{kind=link}
{kind=link}
{kind=link}