
Development of a Smartphone Web-Based Pain Diary to Collect Data on Pain Level and Medications Taken in Children Following Injury or Surgery
John D. Cahoy, MD, PhD, Anneliese Lierhaus, BS, Matthew D. Riedel, MD, Marie Harris, MPH, Rachel L. Difazio, PNP, PhD, Susan T. Mahan, MD, MPH
Disclosure Information©2015 by The Orthopaedic Journal at Harvard Medical School
 PDF
PDFThis paper describes the development of the Orthopaedic Pain Application Log (OPAL), a smartphone web-based pain diary to monitor pain levels, use of analgesic medications, and their effectiveness in children. With the concepts of pain control and narcotic abuse now at the forefront of medical research and community discussion, this web-based application stands to provide a new and effective way of monitoring narcotic need and use in pediatric patients. We discuss the design and development of the Orthopaedic Pain Application Log. Furthermore, we propose a study to test its use for monitoring pain and medication use in patients who undergo emergency department or operative treatment for distal radius fractures. This new smartphone web-based pain diary has the potential to change the way we prescribe and monitor narcotic use in children. The data gathered in this study can be used to establish algorithms and implement protocols for treating pain in both children and adults after orthopaedic injuries and procedures, and may potentially reduce the amount of narcotics prescribed and available in our communities by making our prescribing practices more efficient.
The American Academy of Pediatrics has identified pain management as an integral part of the “comprehensive assessment and management of trauma” and the Joint Commission’s (JCAHO) standards recognize the importance of assessing and treating pain.1,2 These recommendations increase focus on post-discharge pain control; however, this can also lead to the over prescribing of narcotic pain medication. A study by Fortuna et al. 2010 showed that prescribing of controlled substances for adolescents and young adults has nearly doubled since 1994.3 There is concern that these controlled substances may be used for nonmedical purposes, including for psychotherapeutic reasons. The results of the 2006 National Survey on Drug Use and Health showed that 7.0 million or 2.8% of all persons aged 12 or older had used prescription type psychotherapeutic drugs nonmedically in the past month, 16.4 million, or 6.6% of the population, had used in the past year, and 49.8 million or 20.3%, had used prescription psychotherapeutic drugs nonmedically during their lifetime.4 It is also possible that some providers may be hesitant to provide adequate post-discharge narcotics as part of their discharge planning. Likewise parents may be hesitant to appropriately treat their children’s pain while at home. Both situations result in patients having undertreated pain post-discharge.5,6
The nature of narcotic prescribing patterns is of interest beyond the medical community as elected representatives are actively questioning the proper prescribing of narcotics and their availability in communities. The governor of Massachusetts, Governor Charlie Baker, has prioritized an initiative early in his term to take steps to combat opioid abuse. Governor Baker proposed addressing opioid abuse in multiple ways including addressing opioid availability due to over-prescribing.7 Our goal is to appropriately prescribe narcotics based on need and decrease the amount of unused narcotics available for abuse in our communities. We hope to achieve this goal by finding a better way to monitor pain and narcotic use after discharge, and to use this information to adjust our narcotic prescribing practices.
A recent study conducted in the emergency department (ED) at Boston Children’s Hospital (BCH) identified that both children with nonreduced (only required casting), and reduced (required procedural sedation for reduction and casting) fractures had clinically meaningful levels of pain 48-72 hours after ED discharge.8 The Parents’ Postoperative Pain Measure (PPPM), a validated pain score for children 4-12 years as measured by their parents,9,10 was used to measure the child’s pain after ED fracture treatment and discharge. Multivariate logistic regression analysis determined that increased odds of clinically important levels of pain at home were associated with those children who received narcotics for pain control in the ED (odds ratio (OR) 2.58, 95% confidence interval (CI) 1.24-5.39); overnight discharge (OR 1.94, 95% CI 1.01-3.75), and higher pain score at ED arrival (OR 1.15, 95% CI 1.02-1.29).8 A home diary after discharge was also included in this study, however, due to a low 51% return rate, the authors decided that the home diary data was inadequate for analysis.
In order to monitor a patient’s at home pain level, medication use and effectiveness, we have developed a smartphone web-based pain diary to collect data in children following injury or surgery. The Orthopaedic Pain Application Log (OPAL) collects user input on a patient’s smartphone, tablet, or home computer via a secure website that is directly transferred and securely stored on a BCH server. The Orthopaedic Pain Application Log uses a software design similar to a web-based voiding diary developed by the Department of Urology at BCH. This voiding diary was studied in a cohort of 38 patients with mobile Internet access who were asked to use a web-based diary (no choice was given to use a paper diary in this cohort). The authors compared this web-only based cohort to an earlier cohort of 45 patients who used a paper based diary and found that although the web-based diary offered data quality advantages for select groups, the overall data quality was not clearly better for the web-based diary. In addition, the completion rates were somewhat lower for the web-based group. In their analysis and discussion the authors felt that including the option for either the web-based smartphone diary or a paper-based diary might lead to a better overall participation rate and increased quality of the data set.11 Given these results, we will offer a choice of either the Orthopaedic Pain Application Log web-based diary or a paper-based diary to maximize response rates and data quality.
Given the high proportion of adults and children who now have instant access to mobile technology and the increasing popularity of software for regularly monitoring various aspects of our daily lives, we hypothesize that the Orthopaedic Pain Application Log has the potential to both increase both overall participation rate and increase the completeness and prospective nature of the data when combined with the option of a paper based diary. Below we describe development of the Orthopaedic Pain Application Log and a study proposed to test its use.
The Orthopaedic Pain Application Log was developed in order to monitor patient pain and medication use after discharge from the ED or operating room. The Orthopaedic Pain Application Log utilizes a flexible software platform for use across all devices with an Internet Browser, including desktop computers, laptops, as well as tablets and smartphones. The operating system is a secure, HIPAA-compliant network server internal to BCH. The application development team was composed of BCH Information Technology developers, BCH pain specialists from the Department of Anesthesia, as well as physicians, nurses, and researchers from the Department of Orthopaedics. The team initially provided the programming team concept drawings to aid in the application development (Figure 1).
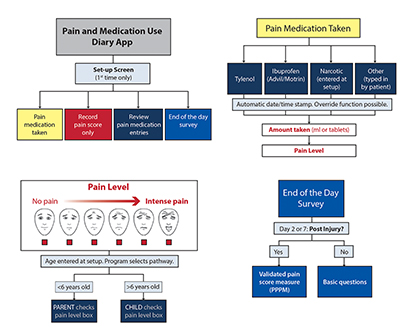
(A) Options from main menu (B) Recording pain medication taken (C) Recording pain level using FACES scale (D) End of the day questions. Faces Pain Scale - Revised (FPS-R). www.iasp-pain.org/fpsr. Copyright ©2001, International Association for the Study of Pain®. Reproduced with permission.
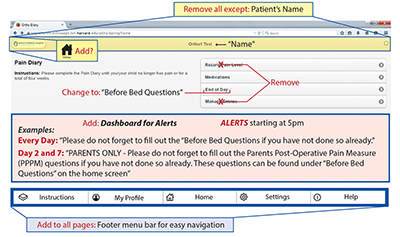
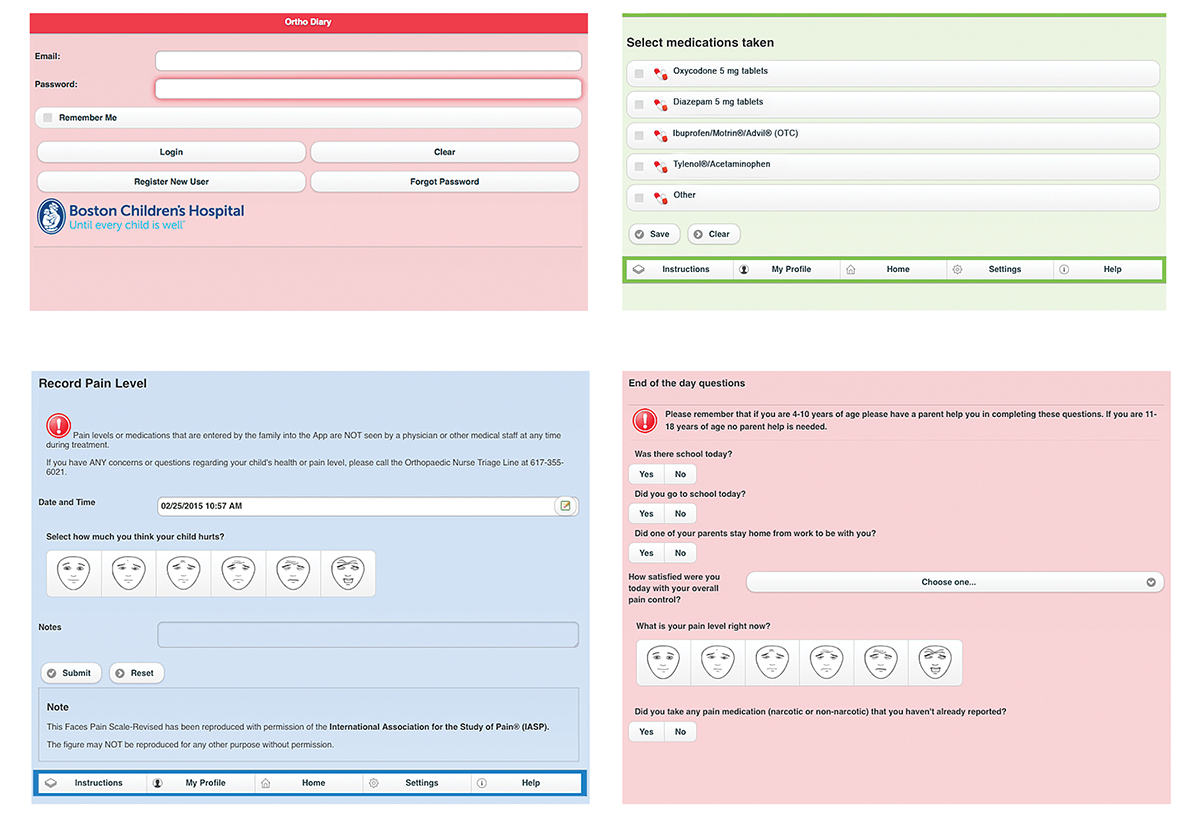
Several versions of the Orthopaedic Pain Application Log were refined to include the following specifications: 1) a user interface that was clean and simple, 2) logical chains of actions with all pages reached in no more than three navigational clicks and 3) “clickable” elements that are clearly presented (Figure 2). The interface design and use of colors and fonts were chosen for ease of reading and legibility. The application structure was designed so that when users entered their input in real time, these inputs would automatically upload and be stored on a secure research server to be accessed and downloaded into a PDF. Screen shots of our version 1.0 are shown in Figure 3 and were used in our first phase of testing.
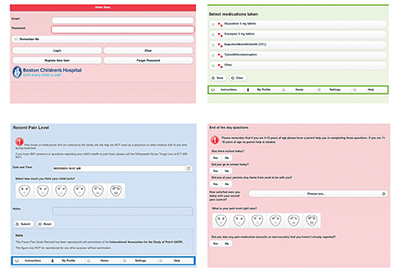
(A) Login screen (B) Record medication (C) Record pain level (D) End of the day question. Faces Pain Scale - Revised (FPS-R). www.iasp-pain.org/fpsr. Copyright ©2001, International Association for the Study of Pain®. Reproduced with permission.13
Technology integration of version 1.0 was piloted in a small orthopedic patient population who were discharged after no more than 2 nights of inpatient stay. The primary objective was to test the general usability, function, and satisfaction of the application. A questionnaire was given to users at the end of the 7-day trial for additional feedback. Preliminary results suggested that OPAL is easy to use and recommendations collected from the pilot pointed to the need for improvement of navigation and enhancement of application design and function. These suggestions have been programmed into the application and we proposed the following study using OPAL.
We will further test OPAL through a prospective observational study involving patients treated for distal radius fractures (DRF) in the ED or operating room at BCH. All patients who are seen and treated for DRF at BCH are currently identified and treated according to the DRF Standardized Clinical Assessment and Management Plans (SCAMPs) treatment algorithm.12 Clinical data is collected on DRF SCAMPs patients including age, gender, injury, and treatment. However, no data is currently collected to capture (a) pain level at presentation, discharge, and during recovery post-discharge, (b) the type and amount of narcotic and over the counter (OTC) pain medication prescribed, and (c) home use, effectiveness, and length of treatment with narcotic and OTC pain medication. Since there is already an extensive dataset on the DRF injury type along with a standardized treatment, we have selected to study pain level and medication use in this group of patients with the Orthopaedic Pain Application Log.
Patients with DRF will be approached in the ED or post operatively for participation in the study. After consenting and before the patient is discharged, a research coordinator will offer to assist in installing the web application on a patient’s or family’s smartphone or tablet that can be used to track the patient’s pain and medication. The day after discharge, families will receive a phone call from the research coordinator to ensure that the web application is working on their device. A paper-based alternative, which the patient can fill out on a daily basis, will be offered to those patient families who prefer to use a paper diary instead of the electronic application. At their first follow-up visit in the orthopaedic clinic, participants will be approached by the research coordinator to fill out a one-time paper-based questionnaire to obtain more details about post-discharge events. This questionnaire will include post-discharge pain, medication use, barriers to medication use, and parent practices regarding their distribution of pain medication in response to patient’s reports of pain.
The goals of this study using the Orthopedic Pain Application Log are to: (1) test a real-time electronic pain monitoring system to monitor how much pain a patient is experiencing after discharge from the ED or the operating room (OR), (2) determine the amount of pain medication used, (3) aid in the development of a standardized algorithm for prescribing pain medications based on the patient’s age, injury pattern, and treatment setting, (4) to more quickly identify patients who may either have unrecognized complications causing increased narcotic requirements or those at risk for abusing narcotic medications, and (5) potentially change the way we prescribe and monitor narcotic use for all both children and adults with other orthopaedic injuries.
This paper describes the development of a smartphone web-based pain diary (the Orthopaedic Pain Application Log, OPAL) to collect data on pain level and medication use in children following injury or surgery. We will use the Orthopaedic Pain Application Log to monitor pain and medication use in children who are treated for a DRF. We will then use this data to identify clinical and demographic risk factors for insufficient pain control and ultimately develop a standardized algorithm for prescribing narcotic pain medication.




{kind=link}
{kind=link}
{kind=link}