
Effective Use of Magnetic Resonance Imaging in the Evaluation of Knee Pain
Eric D. Fornari, MD, Jay Saillant, MD, Isi Obadan, MD, MPH, Caroline H. Hu, BA, Elizabeth G. Matzkin, MD
The authors report no conflict of interest related to this work.
©2015 by The Orthopaedic Journal at Harvard Medical School
 PDF
PDFBACKGROUND Knee pain is one of the most common complaints of patients presenting to clinical practitioners. Despite its prevalence, many clinicians continue to have difficulty evaluating knee pain. The purpose of this study was to ascertain which clinical aspects of a patient’s history and physical exam findings were most predictive of an MRI being of utility in the evaluation of knee pain.
METHODS A retrospective review was performed of all patients (476) who had a knee MRI at a single academic medical center during a consecutive two-year period.
RESULTS Subjects in whom an MRI was of clinical utility (297) differed significantly from those for whom it was not (179) with respect to five independent multivariate predictors: duration of knee disease, presence of knee joint laxity, joint line tenderness, knee joint effusion, and extent of degenerative findings on plain radiographs. The predicted probability of an MRI being of clinical utility is summarized as 25% for one predictor, 43% for two, 56% for three, 72% for four, and 95% if all five are present. There was a strong relationship between the number of predictors and the proportion of subjects in whom an MRI was of clinical utility, as well as good diagnostic performance of this group of five multivariate predictors.
CONCLUSION This study has derived five multivariate predictors (duration of symptoms, presence of knee joint laxity, joint line tenderness, knee joint effusion, and extent of radiographic degenerative findings) that are meant to aid clinicians in evaluating patients who present with knee pain. These results should serve as an initial guide to determine the utility of an MRI in a patient presenting with knee pain.
Knee pain is one of the most common complaints of patients presenting to both primary care and orthopedic physicians. It has been found to be present in up to 20% of the adult general population and represents the primary physical symptom of up to 6% of patients presenting to an adult primary care clinic.1,2 Determining the underlying etiology can sometimes be difficult, in part because of the extensive differential diagnosis. Thus, despite its prevalence, many clinicians continue to have difficulty evaluating knee pain and the indications for specific imaging modalities are often unclear.3 Furthermore, if they do order some form of imaging, our experience demonstrates that the indications for specific imaging modalities are not clear.
In the hands of a trained practitioner, the knee examination is reasonably sensitive in detecting meniscal and ligamentous injury.3 The widespread availability of magnetic resonance imaging (MRI) has changed the diagnostic approach to many orthopedic conditions, including the knee. It has become an important diagnostic tool with both a high sensitivity and specificity with regard to detecting intra-articular pathology.4,5 Shifts in referral have led to an increase in the use of MRI by non-orthopedic physicians.6,7 Numerous studies have demonstrated, that when used appropriately, such modalities are cost-effective, have been able to avoid unnecessary referrals to orthopedists, or changed referral to a more appropriate secondary care provider.8-11
In today’s health care climate, proper allocation of resources is of paramount importance. In addition to excessive health care costs, inappropriately ordered MRIs often identify negative findings that cause delayed referrals or demonstrate pathologies unrelated to the patient’s symptoms that cause unnecessary referrals. Appropriate medical practice dictates that a study should only be obtained if it is believed that the outcome will influence the treatment plan. The American College of Radiology (ACR) Appropriateness Criteria was developed over a decade ago to improve imaging decision making, however, has shown a very low utilization rate thus far.15 The ACR Appropriateness Criteria recommends plain radiography as the proper initial step in the evaluation of knee pain and that no further imaging is indicated if the initial radiographs demonstrate inflammatory, crystalline, or severe degenerative joint disease.12-14 Our clinical experience has demonstrated that these principles are either not universally known or they are not adhered to, resulting in unnecessary MRIs being obtained.
The purpose of this retrospective review was to ascertain which clinical aspects of a patient’s history and physical exam findings were most predictive of an MRI being of utility in the evaluation of knee pain. We hypothesized 1) that unnecessary knee MRIs are ordered and this could be decreased using simple radiographic and clinical exam findings and 2) more unnecessary MRIs are ordered by non-orthopedic physicians.
The institutional review board approved this study. A retrospective review of all knee MRIs ordered at a single academic medical center over a two year period was performed. Inclusion criteria included patients >18 years old and evaluation by a member of the adult orthopedic department. A pre-study power analysis using a 90% probability of detecting a 15% difference in the probability of meniscal tear among patients with and without joint line tenderness determined 462 patients would be required. A chart review was performed on patients who met these criteria to collect demographics and physical exam data. All radiographs and MRIs were also reviewed. Radiographs were evaluated by a resident and an attending for severity of osteoarthritis using the Kellgren-Lawrence Grading System.16 We considered Grades 0-2 to be mild, Grade 3 to be moderate, and Grade 4 to be severe osteoarthritis.
Patients were considered appropriate candidates for an MRI if their clinical diagnosis and treatment required possible surgical intervention. This included ligament tears with clinical instability, meniscal tears and chondral flap tears or lesions with mechanical symptoms in which potential surgery would be beneficial to alleviating symptoms. Since there are no formal guidelines available, there was no standard to compare to or use as a control. Patients were then placed into a group of “MRI indicated” or “MRI not indicated” for further analysis. In order to validate the placement of patients in MRI appropriate groups, a workgroup of experts in Orthopedics, Rheumatology, Primary Care, and Musculoskeletal Radiology was convened to evaluate several patient scenarios. The experts were asked if they would order an MRI based on patient scenarios created using the studied predictors – age, chronicity, effusion, joint line tenderness, ligamentous stability and Kellegren Lawrence grading of osteoarthritis. Group census demonstrated that there was agreement in all patient scenarios amongst these experts.
Data are summarized with descriptive statistics: continuous data are presented as Mean ± SD or Median (range) while categorical variables are presented as frequencies and percentages. Comparisons of continuous data were performed using T-tests and differences in proportions, analyzed using chi-squared tests. Where appropriate, non-parametric alternatives (e.g. Mann-U-Whitney test) were applied. Multiple logistics regression with stepwise selection was performed to identify independent clinical predictors of “the clinical utility of MRI in evaluating knee abnormalities”. Regression model fit was estimated with Hosmer and Lemeshow goodness-of-fit test, and results were reported using regression estimates, adjusted odds ratios, p-values and 95% confidence intervals.
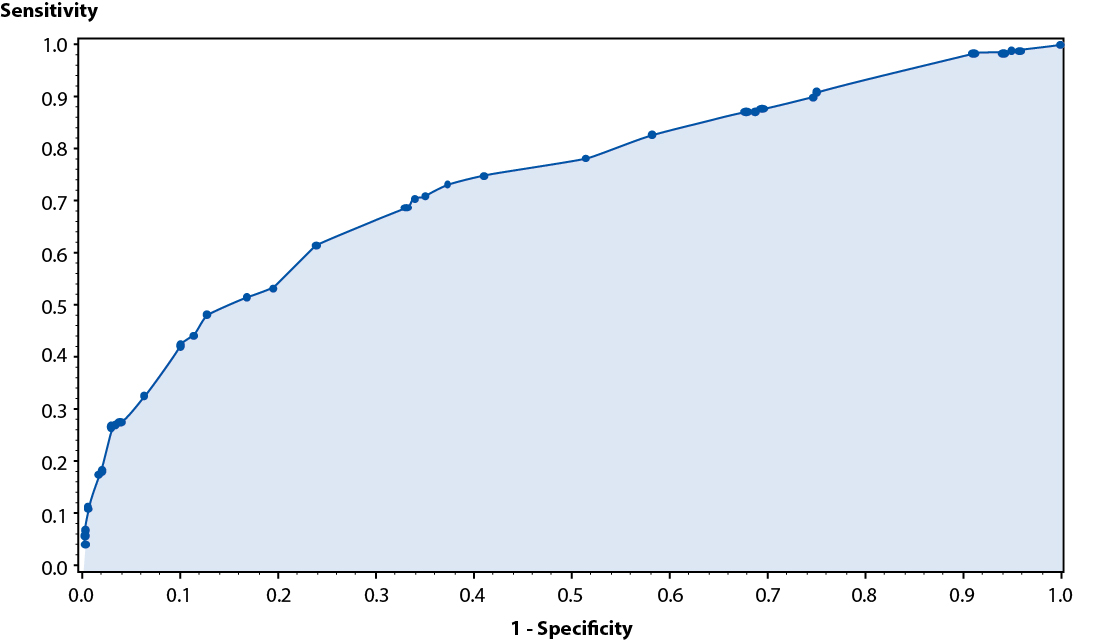
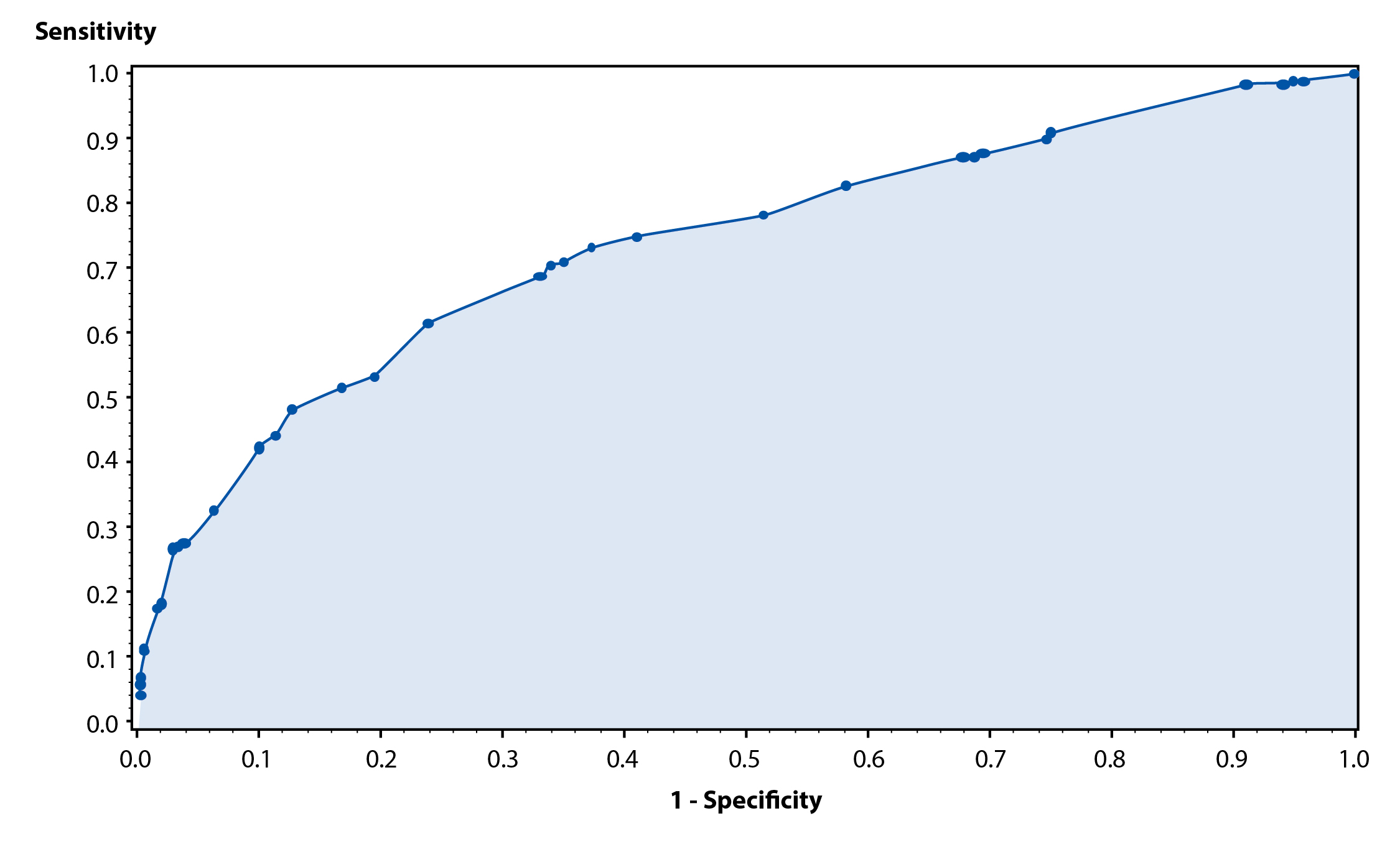
The probability of having a knee abnormality requiring MRI evaluation was estimated for each combination of predictors, and a Mantel-Haenszel chi-square test for trend was used to evaluate the relationship between increasing number of predictors and the proportion of subjects with knee abnormalities requiring MRI evaluation. Also, a receiver operating characteristics (ROC) curve was constructed to assess the diagnostic performance of this group of multivariable predictors in identifying “the clinical utility of an MRI” given the presence of knee abnormalities.
Use of MRIs was compared between orthopedic and non-orthopedic physicians using chi-squared analyses. Data on subjects referred to orthopedic physicians were also analyzed. Formal hypotheses testing were two sided with statistical significance defined as p < .05. All statistical analyses were done using Statistical Analysis Software version 9.1.3 (SAS Institute, Inc., NC).
Our chart review identified 476 subjects who had an MRI of their knee at an academic medical center over a continuous 2 year period and met the aforementioned inclusion criteria. 201 (42.2%) were above 50 years of age, and 254 (53.4%) were females. More than half of the subjects (58.4%) presented with chronic knee disease (defined as > 6 weeks in duration). Over two-thirds of cases reviewed (68.3%) had joint line tenderness of their affected knee, while 53.6% had a knee effusion on physical examination and 53.8% had left-sided knee pain.
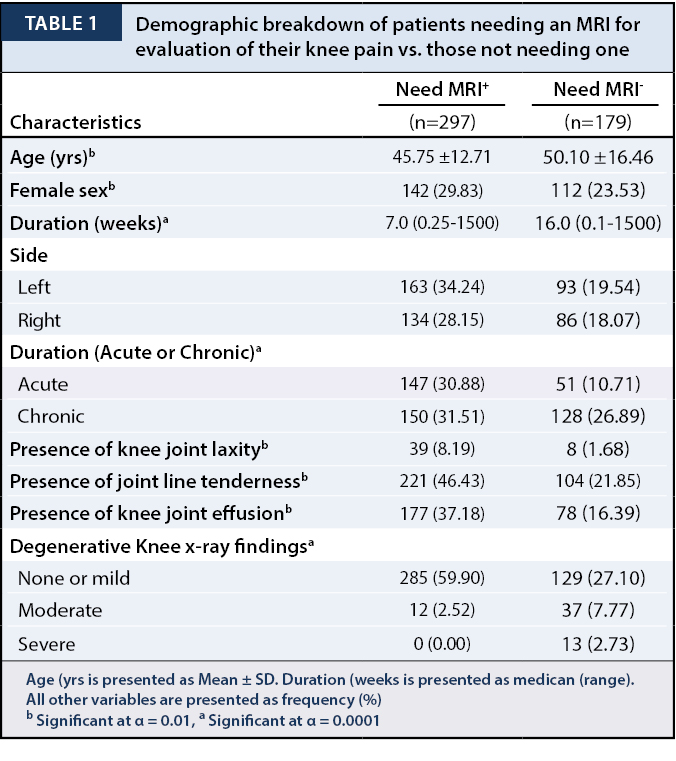
Subjects in whom an MRI was of clinical utility (297) differed significantly (p < 0.01) and (p < 0.0001) from those for whom an MRI was not useful (179) for evaluation of their knee abnormalities with respect to age (45.71 ± 12.73 vs. 50.1 ± 16.46 years), proportion of females (29.8% vs. 23.53%), duration of knee disease (30.88% vs. 10.71%) as well as evidence of knee laxity (8.19% vs. 1.68%), joint line tenderness (46.43% vs. 21.85%) and joint effusion (37.18% vs. 16.39%) on physical examination (Table 1).
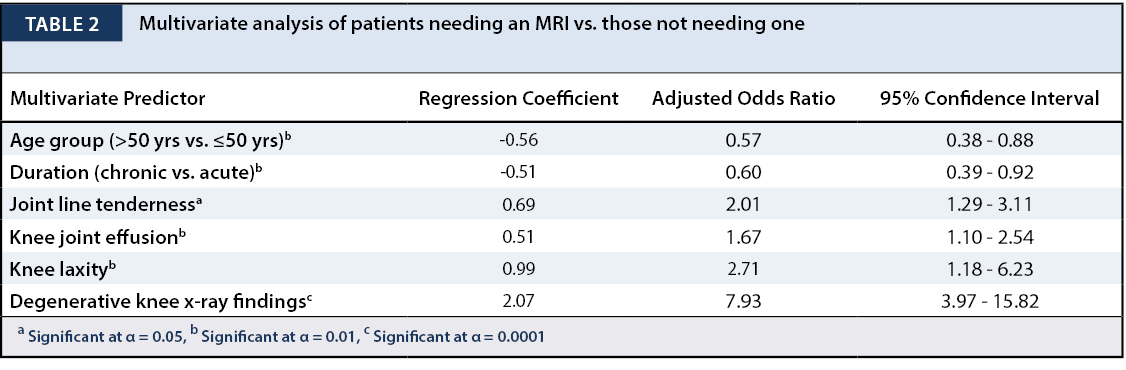
Multivariate regression yielded 6 independent predictors for clinical necessity of an MRI for further evaluation of knee pain: age, duration of knee disease, presence of knee joint laxity, joint line tenderness, knee joint effusion on clinical examination and degenerative findings on knee X-ray (Table 2). Results showed that subjects who were over 50 years of age were 43% less likely to need an MRI for the management of their knee condition compared to those aged 50 and below (p < 0.01), and those with chronic knee pain (> 6 weeks) were found to be 40% less likely, compared with subjects with knee pain of acute duration (p < 0.01). Those with none to mild degenerative knee X-ray findings were significantly more likely to require a knee MRI when compared with their counterparts having moderate to severe degenerative changes (p < 0.0001), indicating that lack of radiographic evidence of degenerative changes is a strong predictor of the clinical necessity for an MRI.
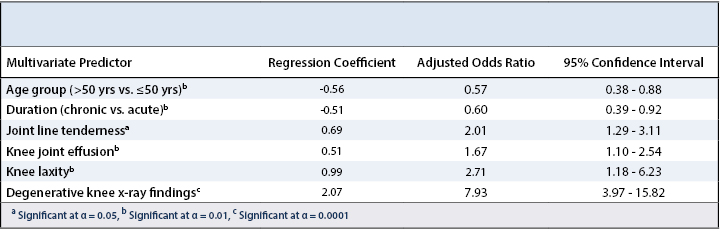
However, age and degenerative findings on X-ray were found to be strongly associated (p < 0.0001): 414 of the 476 subjects (86.97%) analyzed for this study showed no to mild changes on X-ray, with significantly more subjects (64.7% vs. 35.3%) aged 50 years or below. It was determined that both variables likely evaluated the same underlying concept, thus age was excluded as one of the variables further analyzed. We therefore utilized 5 multivariate predictors in the algorithm described below.
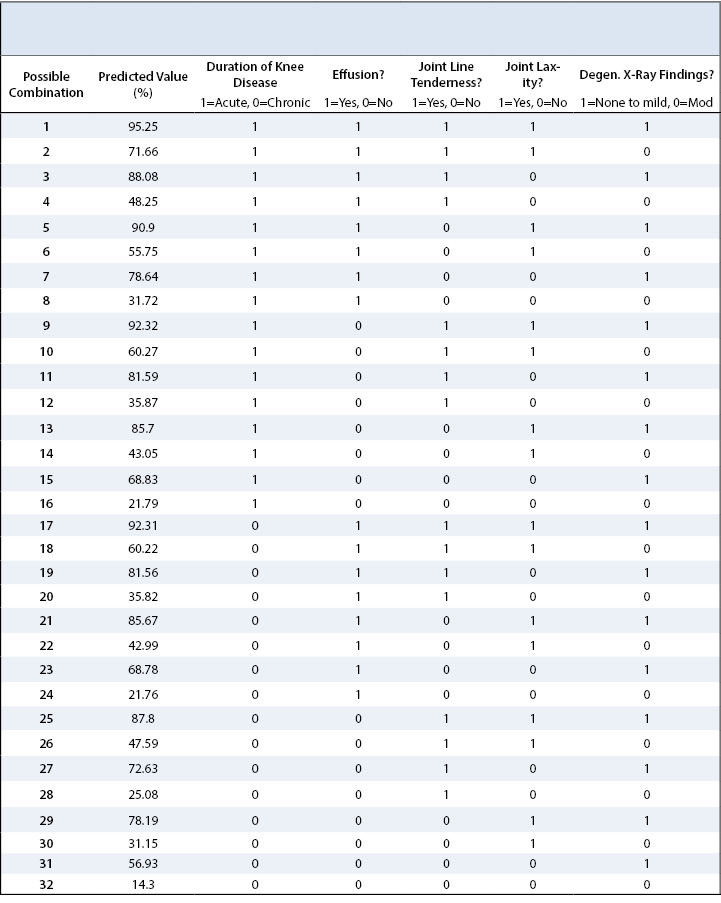
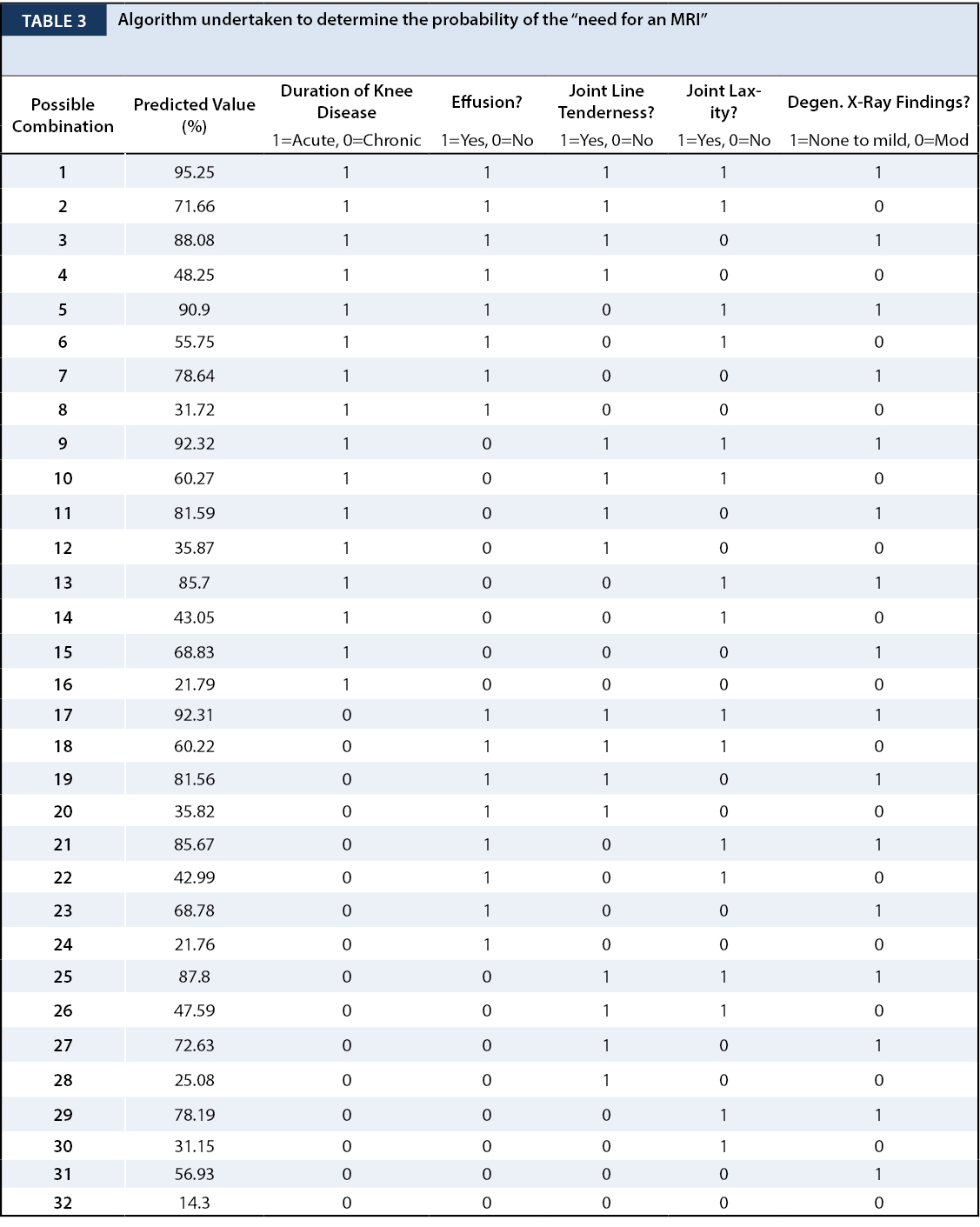
We developed an algorithm to ascertain the predicted probability of “the clinical utility of an MRI for further knee evaluation” on the basis of all possible combinations (2 x 2 x 2 x 2 x 2) of all five binary multivariate predictors (Table 3). For example, a patient who presents with a knee effusion, joint line tenderness and is found to have at best, mild degenerative changes on knee X-ray, will have an 81.56% probability of needing an MRI for further management. Conversely, a patient with a chronic knee condition that presents with a knee effusion, no joint line tenderness or laxity, and moderate degenerative changes on knee X-ray will have a predicted probability of requiring a MRI of only 21.76%.
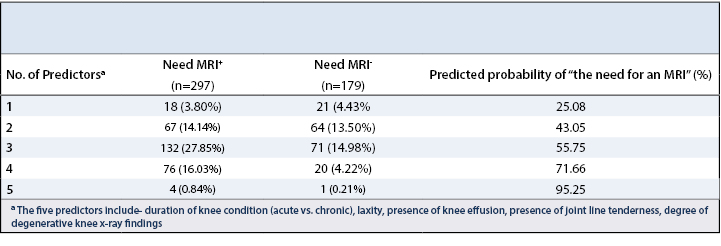
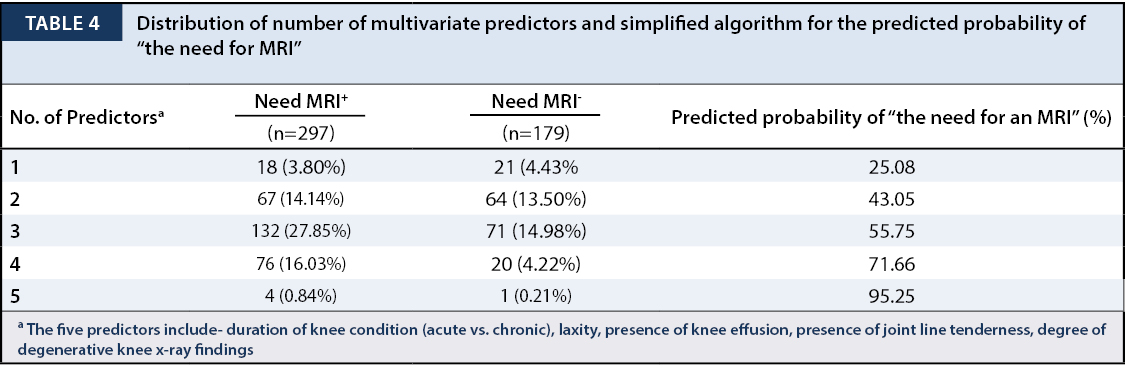
We also developed a simplified algorithm based on the number of multivariate predictors (one through five) (Table 4). For example, an adult with a suspected knee abnormality but only one of the above listed predictors has an 25.08% predicted probability of needing an MRI for further management, whereas an adult presenting with all 5 multivariate predictors has a predicted probability of 95.25% of needing an MRI.
The Mantel-Haenszel chi-square test for linear association indicated a very strong relationship between an increasing number of predictors and the proportion of subjects in whom an MRI was of clinical utility (p < 0.0001). The relationship was also evaluated with a receiver operating characteristics analysis (Figure 1), with the area under the ROC curve (73.7%), indicating good diagnostic performance of this group of 5 multivariate predictors in identifying clinical situations where an MRI is needed for management of the patients knee pain.
Of the 476 MRI tests ordered, our data revealed that orthopedic surgeons ordered a majority of the MRIs (68.34% vs. 31.66%). However, only 35% of the non-orthopedic ordered-MRIs were eventually ascertained to be useful in the management of these patients, compared with a 75% usefulness rate of all MRIs ordered by orthopedic physicians. Thus, orthopedic physicians had significantly more appropriately ordered MRIs than their primary care counterparts (p < 0.0001). In at least 52.62% (251 of 476) cases, patients were referred to an orthopedic physician without an initial X-ray. Furthermore, 13% (61 of 476) of patients in our study population had an MRI done before X-rays were obtained. Based on our algorithm, 57.37% (35 of 61) of those patients did not need an MRI in the work-up of their knee pain.
This study has derived five multivariate predictors to help determine if a patient is in need of an MRI for further evaluation of their knee pain (duration of symptoms, knee effusion, joint laxity, joint line tenderness, and extent of radiographic degenerative changes). Attention to these aspects of a patient’s presentation and exam may serve as an initial guide for clinicians when deciding whom to refer for an MRI and in doing so, can reduce the number of unnecessary tests ordered.
When presented with any clinical symptom, the fundamentals of a thorough history and clinical examination cannot be overemphasized. Jackson et al. performed a systematic review of the literature regarding the evaluation of acute knee pain in the primary care setting and found that the physical exam was reliably sensitive in detecting meniscal, ACL, and PCL tears (74%-81%) but less sensitive for detecting other cartilaginous damage (51%).3 For all lesions, except medial meniscus tears, specificity was high (92% to 96%), suggesting that physical exam is normal in patients without damage to these structures.3
It is clear that MRI is the technique of choice to image internal derangement of the knee. Subhas et al. collected pre-MRI history, diagnosis, and planned management and reviewed post-MRI results in 93 patients, and demonstrated that MRI results changed diagnosis in 29.3% and management in 25.3% of cases.17 When used appropriately, MRI is a cost-effective means of avoiding unnecessary diagnostic arthroscopy.8,9 Munk et al. found MRI to have twice the positive predicative value for meniscus tear compared to clinical examination.18 Additionally, they found that MRI would reduce a resultant negative diagnostic arthroscopy to 5%.18 The diagnostic value of MRI for ligamentous injuries has also been shown to be high.19,20 There are varying reports in the literature on the utility of MRIs ordered by specialists compared to non-specialists. Uppal et al. and Lee et al. found no difference in the prevalence of abnormalities found on knee MRI in patients referred by orthopedic and non-orthopedic surgeons.21,22 Conversely, Sherman et al. found that the rate of normal results for non-orthopedic practitioners was 33.9% compared with 15.3% for orthopedic surgeons (P<0.001).23 Similarly, Wylie et al. found that MRIs ordered by orthopedic surgeons had twice as many positive findings than MRIs ordered by primary care physicians.24 Other studies have also demonstrated that primary care providers order a high percentage of MRIs that either show normal findings or would not alter the treatment plan.25,26 Our data revealed that orthopedic physicians ordered more MRIs compared to primary care physicians (68.4% vs 31.6%). However, only 35% of the PCP-ordered MRIs were eventually useful in patient management, whereas the MRIs ordered by the orthopedic physicians had a 75% usefulness rate. This low diagnostic utility of MRIs ordered further emphasizes the need for a tool to assist physicians with imaging decisions.
Bhattacharyya et al. demonstrated that meniscal tears are clearly associated with osteoarthritis and that the chance of MRI detecting a medial or lateral meniscus tear in the presence of radiographic findings of moderate osteoarthritis (slight joint space narrowing) is 89%.12 They concluded that MRI contributes little to the decision-making process regarding treatment of patients with symptomatic knee osteoarthritis,12 considering that concomitant meniscal tears are frequently asymptomatic and arthroscopy has not been shown to be more beneficial than conservative treatment for knee osteoarthritis.12,27,28 This follows the recommendations of the American College of Radiology who contend that a MRI is not indicated for the evaluation of non-traumatic knee pain before plain radiographs or when radiographs reveal significant degenerative changes because additional imaging will not alter the treatment plan.13 Pill et al. made a similar argument, demonstrating that weight-bearing radiographs are ideal for evaluating knee pain and that MRIs are only indicated when the cause of knee pain is not readily apparent after careful physical and radiographic evaluation.14 Likewise, our study confirmed that the presence of even moderate degenerative changes on X-rays was a negative predictor of the clinical utility of further imaging with MRI.
In our study population, 13% of the patients had an MRI performed prior to having plain radiographs of their knee. Based on the application of our group of multivariate predictors, 57% of these patients ultimately did not require their MRI scan for management of their knee pain. This is similar to findings by Lee et al.22 In their study, 37% of the MRI scans were not preceded by radiographs.22 Furthermore, George et al. showed that 28% of knee MRIs in a large Medicare database were performed without prior radiographs.29 Combined with shoulder MRIs without preceding radiographs, George et al. found the extrapolated expense of these unwarranted MRIs to be between $20 and $35 million.29 Both Gelb et al. and Boden et al. also demonstrated that the practice of using MRI as an initial screening tool is not cost-effective.30,31
One of the strengths of our study is the large number of subjects that it included as well as a pre-study power analysis, which was done to ensure that we obtained an appropriate sample size. Furthermore, all patients were evaluated by physicians specializing in the evaluation of the musculoskeletal system, which provides standardization to their exam. This study also has its limitations. It was retrospective in nature and thus subject to all the usual biases that accompany such literature. In addition, we acknowledge the inherent controversy and subjectivity in making the determination which patients we deemed as needing an MRI. Since there are no formal guidelines to utilize as a standard control, the decision on when to order an MRI is left to the discretion of the evaluating practitioner. In order to substantiate the need for an MRI, a multidisciplinary group of experts was convened and demonstrated agreement in evaluating patient scenarios. We also contend that our methodology parallels actual clinical practice.
Our study derived five clinical predictors (duration of symptoms, effusion, laxity, joint line tenderness, and degree of radiographic degenerative change) that can serve as a guide for clinicians when determining the need for an MRI in the evaluation of knee pain. Furthermore, standard radiographs, ideally including weight-bearing views, should routinely be obtained prior to considering more invasive and costly imaging modalities. As in all clinical situations, decisions regarding the proper course for an individual patient’s care are ultimately best left at the discretion of the involved health care professional. We intend for these results to serve as a guide to aid clinicians when deciding how to best evaluate knee pain and hope it will allow them to do so in a more efficient and cost-effective manner.
We thank Rafael Cavalcanti, MD for his assistance with data collection and Emily Curry, BA for her assistance with manuscript preparation.







{kind=link}
{kind=link}
{kind=link}
{kind=link}