
Atraumatic Lumbosacral Fusion Mass Fracture: Bisphosphonates to Blame?
Heeren Makanji, MD, Ahmer Ghori ,MD, Gregory W. Brick, MBChB
The authors report no conflict of interest related to this work.
©2015 by The Orthopaedic Journal at Harvard Medical School
 PDF
PDFBACKGROUND To report a case of an atraumatic fracture through a posterolateral lumbosacral fusion mass following removal of instrumentation in a patient on prolonged bisphosphonate therapy.
METHODS Case report and review of the literature.
RESULTS A 55-year-old woman with spondylolisthesis who underwent uncomplicated L4- S1 laminectomy and posterolateral fusion with pedicle screw constructs presented six years later with back pain. Imaging revealed a robust fusion mass with no implant failure or pseudarthrosis. She underwent removal of hardware, and one week later, the patient returned with a non-displaced fracture through the fusion mass. The patient was managed non-operatively with a lumbar orthosis and referred for endocrine consultation. She had received bisphosphonate therapy for 8 years and was subsequently transitioned to teriparatide. CT scan one year after removal of instrumentation showed a healed fracture through the fusion mass.
CONCLUSION Despite evidence of a robust fusion mass after spinal fusion, prolonged bisphosphonate therapy may contribute to atraumatic fracture.
Degenerative spondylolisthesis is common in patients over 50 years of age and often presents with symptoms of spinal stenosis.1 Surgical management includes decompression and instrumented fusion to address pain, neurologic symptoms, and instability.2
Clinical outcome is good to excellent in up to 80% of patients, but back pain may persist in a small percentage of these patients.3 Although the etiology of this residual back pain is unclear, hardware-related pain is a recognized entity. Removal of hardware can alleviate this pain, but this strategy remains controversial because painful hardware is a diagnosis of exclusion.4 There remains a paucity of literature on complications after removal of hardware after posterior-lateral spinal fusion.5,6
We report a case of an atraumatic fracture of a posterolateral fusion mass following removal of pedicle screw/rod construct in a patient concurrently being treated with bisphosphonates.
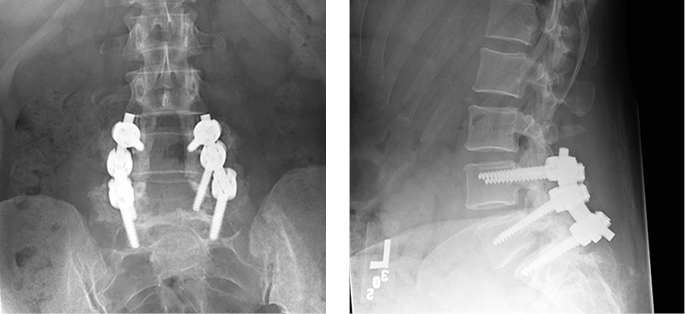
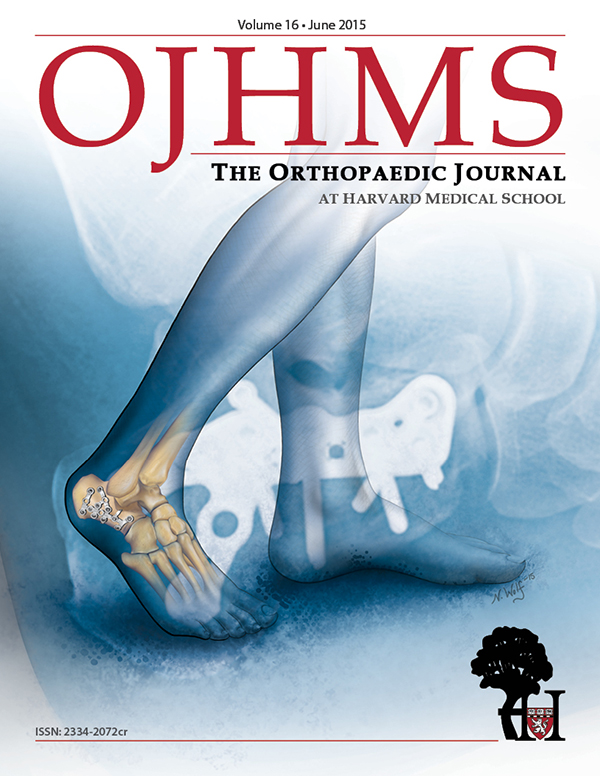
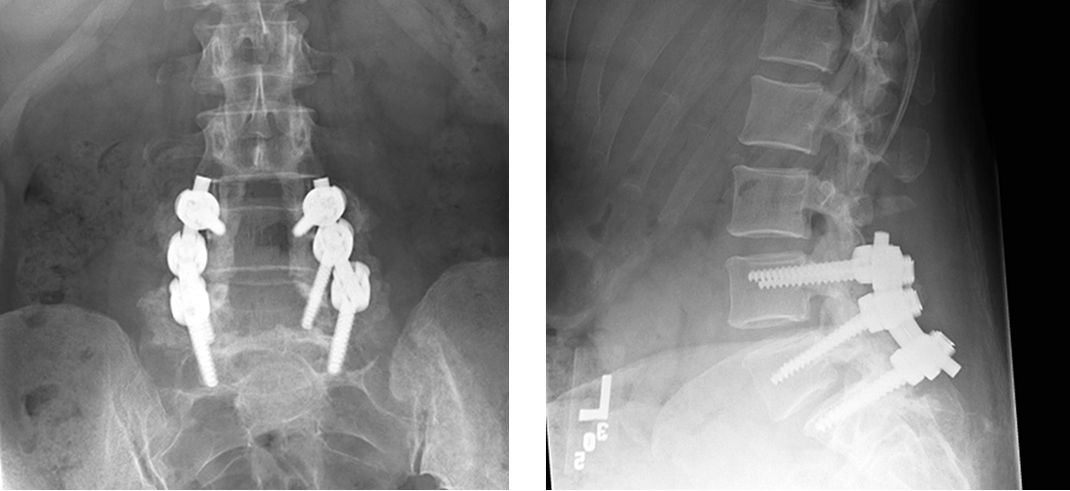
A 55-year-old female with spinal stenosis at L4-S1 and grade 1 degenerative spondylolisthesis at L4-L5 underwent uncomplicated laminectomy and posterior-lateral fusion using a pedicle screw/rod construct and iliac crest bone graft (Figure 1)). Surgical outcome was excellent with significant pain relief and no complications. Six years postoperatively, the patient developed recurrent back pain localized to the right L5-S1 paraspinal region unresponsive to conservative measures. A CT scan at this time demonstrated a robust fusion mass bilaterally without any evidence of implant failure, pseudarthrosis, or junctional instability (Figure 2). C-reactive protein was 5.7 mg/L and erythrocyte sedimentation rate was 17 mm/hr.
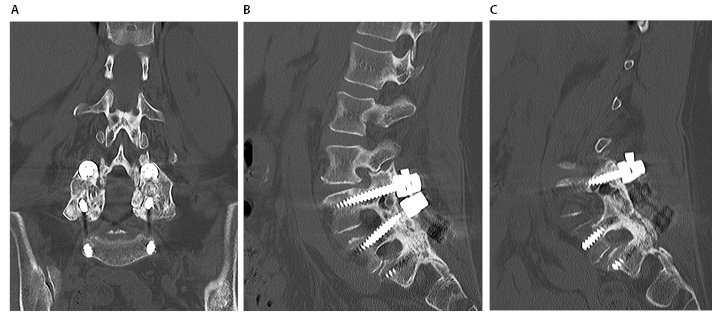
Robust fusion mass in (A) Coronal, (B) Left posterolateral, and (C) Right posterolateral views. Implants were well-fixed, and no evidence of instability was noted intraoperatively.
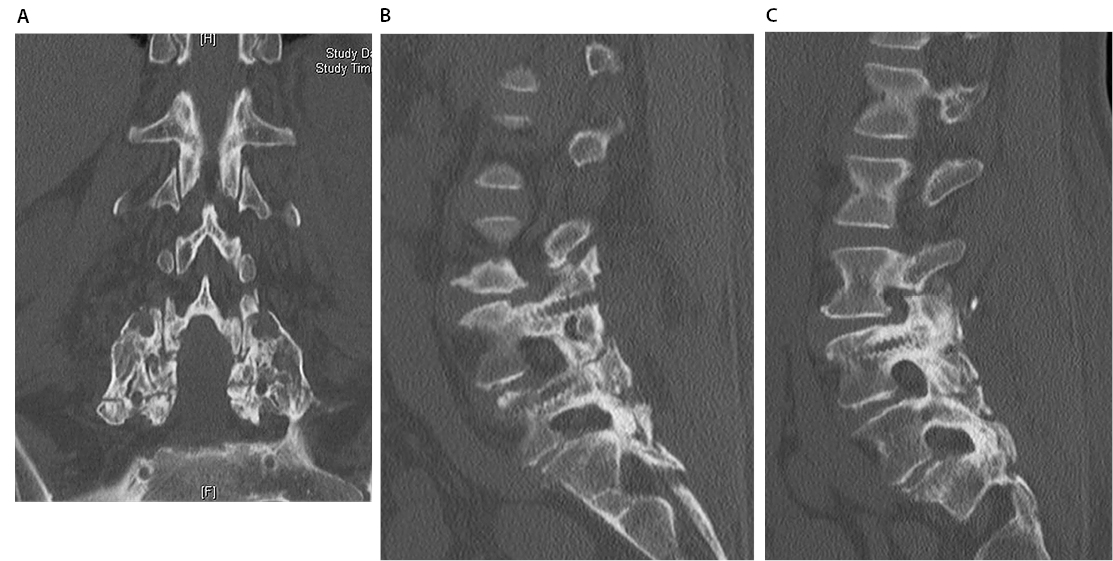
Due to continuing pain and failure of conservative measures, including physical therapy, the patient ultimately elected to have instrumentation removed. Intra-operatively, the bridging fusion at all levels was deemed solidly healed without instability. The patient was weight bearing as tolerated and was discharged home after physical therapy evaluation on post-operative day three. The patient returned one week later with inability to ambulate secondary to severe back pain. She denied any traumatic events, and a subsequent CT scan revealed a non-displaced fracture through the L4-L5 facets bilaterally and mild compression fracture of the L5 vertebral body (Figure 3). She was treated non-operatively with a back brace and referred for endocrine consultation.
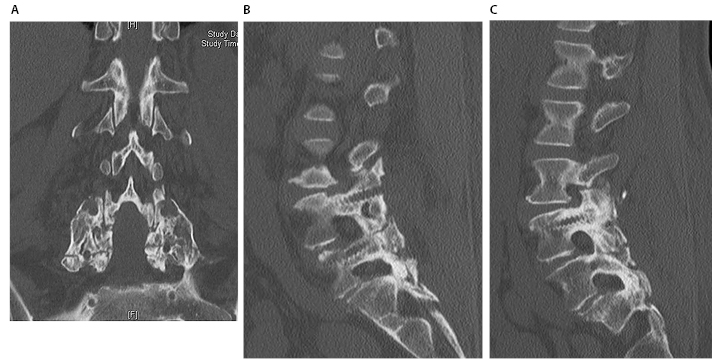
Fracture extends bilaterally from the fused facets joints of L4-L5 and through the L5 pedicle screw holes. A Mild compression fracture was also noted at the anterior vertebral body of L5. Multiple views are shown: (A) Coronal, (B) Left posterolateral and (C) Right posterolateral
The patient had been on uninterrupted alendronate therapy (70 mg weekly) for eight years prior instrument removal for osteopenia (T score -1.4). Her most recent DEXA scan had shown osteopenia (T score -1.5). Laboratory tests during endocrine consultation revealed normal bone specific alkaline phosphatase (12.2 mcg/L), osteocalcin (33 ng/mL), procollagen type I propeptide (65 mcg/L) and serum c-telopeptides (397 pg/mL). There was no evidence of metabolic bone disease.
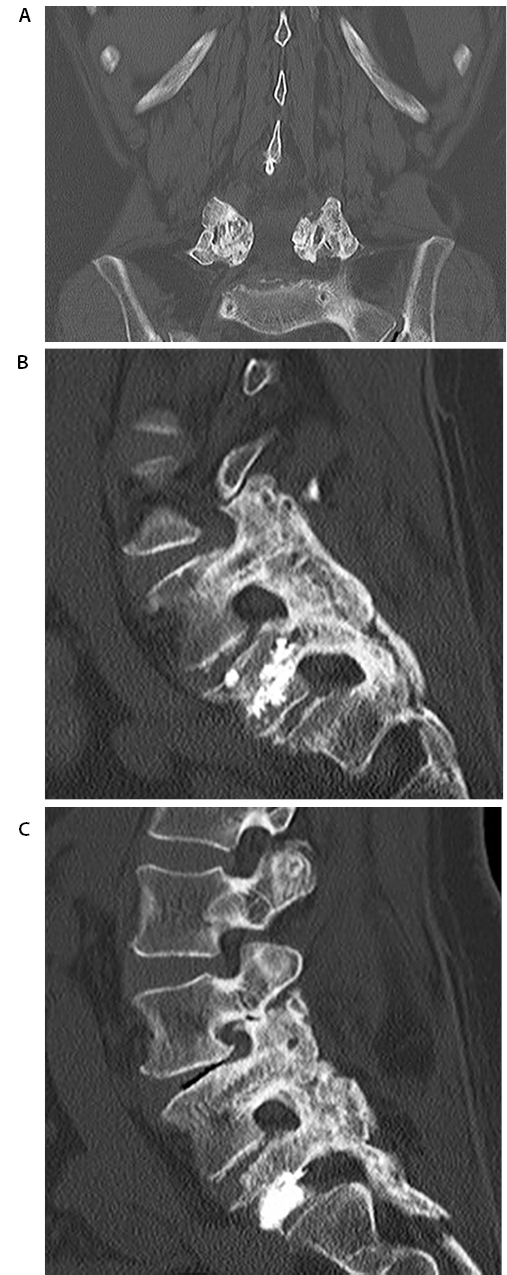
Alendronate was discontinued, and anabolic therapy using teriparatide was initiated. Vertebroplasty was performed four months later for the L5 compression fracture with moderate pain improvement. The final CT scan one year after removal of instrumentation showed a healed fracture through the fusion mass (Figure 4). At final follow-up, the patient had returned to her baseline, full ambulation with occasional use of cane, and with no residual back pain.
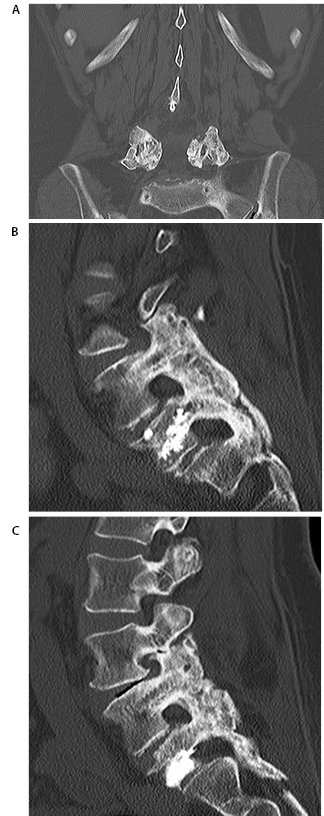
(A) Coronal, (B) Left posterolateral, (C) Right posterolateral
Studies report excellent clinical outcomes after decompression and instrumented fusion for spondylolisthesis.1-3 Screw breakage and loosening are the most common complications of instrumentation.7 Removal of hardware is occasionally performed after fusion when the cause of recurrent back pain cannot be determined. However, this strategy remains controversial, as implant removal has been reported to have a 3% to 20% complication rate overall.8,9 Infection, significant vessel injury, and vertebral compression fractures have been reported in the literature, but large studies are lacking.
Atypical fractures of the subtrochanteric femur with prolonged bisphosphonate therapy are well documented.10 However, a causal relationship has yet to be established.11
While several studies have evaluated the effect of bisphosphonate therapy on bony healing after spinal fusion surgery, controversy remains. Bisphosphonates function by inhibiting the enzyme farnesyl-pyrophosphate synthase in osteoclasts, leading to cytoskeletal abnormalities and inability to create the ruffled border.10 Experiments in animal models have suggested that alendronate inhibits bony fusion despite fusion masses that may appear radiographically larger and more dense.12,13 A recent systematic review has supported claims that bisphosphonate therapy may impede bony fusion, but implications for mechanical strength of the construct are unknown.14 A more recent animal study, showed no significant difference in fusion rate, but did show a significant decrease in tensile strength of the fusion mass in the group treated with low and high dose alendronate.15 Alternatively, several studies have also shown no difference or increase in fusion rates with bisphosphonate therapy.16,17 There is a paucity of literature evaluating the effect of bisphosphonates on the integrity and mechanical strength of the fusion mass over the long term, after there is initial evidence of fusion.
Although the evidence surrounding bisphosphonate therapy is debated, the argument for PTH treatment (teriparatide) is more convincing. Teriparatide is a synthetic analog of PTH, which when given, intermittently stimulates increased bone formation (but leads to bone resorption if chronically elevated.18 Unlike bisphosphonates, these agents promote creation of new bone rather than preventing breakdown of existing bone. Several studies and a systematic review have suggested that PTH treatment increases fusion rates and improves microarchitecture.13, 18-19 When compared to bisphosphonate therapy, PTH treatment improves rate and duration of bone union and reduces rate of pedicle screw loosening in osteoporotic patients.20, 21
While the cause of the fracture in this case is unknown, it is possible that bisphosphonate therapy contributed to subclinical fracture in the fusion mass, which may have been the source of back pain. With removal of hardware and the creation of a new stress riser at the site of the previous pedicle screw, this subclinical fracture may have propagated through the fusion mass. Alternatively, the stress riser itself may have led to de novo fracture. Although the pre-operative CT scan and intraoperative findings were not suggestive of pseudarthrosis, surgical exploration may not necessarily appreciate this entity and it can also contribute to potential fracture. While result after the index procedure was excellent, the effect of bisphosphonate therapy over the long term in these patients is uncertain.
This is a case of an atraumatic fracture through a spinal fusion mass after implant removal in a patient on prolonged bisphosphonate therapy. The etiology of the fracture is unknown, but extended bisphosphonate therapy likely contributed to a subclinical fracture that propagated after implant removal.





{kind=link}
{kind=link}
{kind=link}