
The Validity of Using ICD-9 Codes for Identifying Venous Thromboembolism Following Below Knee Surgery
Reinout R.O. Heijboer, BSc, Bart Lubberts, MD, Pim A. D. van Dijk, BSc, Bryan G. Vopat, MD, Anne H. Johnson, MD, Daniel Guss, MD, MBA, Christopher W. DiGiovanni, MD
The authors report no conflict of interest related to this work.
©2016 by The Orthopaedic Journal at Harvard Medical School
 PDF
PDFBACKGROUND To determine the incidence of venous thromboembolism (VTE) after surgeries performed below the knee, previous studies have used the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) procedure codes to identify a DVT (deep vein thrombosis) or PE (pulmonary embolism) event. The purpose of this study was (1) to determine the incidence of VTE in a large cohort of patients who had undergone surgery below the knee, and (2) to assess the validity of the ICD-9-CM procedure codes used.
METHODS Current Procedural Terminology codes and ICD-9-CM codes were used to identify patients who had undergone below knee surgery and developed a reported VTE. The medical records of 21,904 patients were evaluated to assess the validity of the VTE ICD-9-CM code against the documentation of DVT or PE in radiology reports. Positive predictive value (PPV) and sensitivity of ICD-9-CM codes were calculated.
RESULTS The incidence of VTE was 2.5% (552/21,904). Of those patients identified as having VTE, 344 (62.3%) had a DVT, 130 (23.6%) had a PE, and 78 (14.1%) were recorded as having both a DVT and PE. The PPV of ICD-9-CM coding were 55.7% (327/587) for DVT, 84.4% (108/128) for PE, 60.2% (59/98) for DVT/PE combined, and 60.8% (494/813) for VTE in total. The resulting sensitivity scores were 95.1% (327/344) for DVT, 83.1% (108/130) for PE, 75.6% (59/78) for DVT/PE combined, and 89.5% (494/552) for VTE in total.
CONCLUSION The overall rate of VTE after below knee surgery was 2.5%. This study found that ICD-9-CM code use had an 89.5% sensitivity rate for VTE. Using ICD-9-CM codes to search for a VTE demonstrated a low PPV, however, because only 60.8% could be verified by a radiological study. By comprehensively assessing the incidence of VTE after below knee surgery, we illustrated a potential source of inaccuracy in the use of retrospective ICD-9-CM based data capture methodologies.
Venous Thromboembolic Disease (VTE)—encompassing Deep Vein Thrombosis (DVT) and Pulmonary Embolism (PE)—occurs in 1 to 2 per 1000 persons per year in Western countries, and is the third most common cardiovascular disease after myocardial infarction and stroke.1-3 VTE is often caused by the immobilization or tissue injury that result from trauma or surgery, and can be a significant cause of morbidity and mortality following orthopaedic surgery.4,5
Within the below knee surgical population, wide variation in the use of VTE chemoprophylaxis remains—due, in part, to a lack of consensus regarding risks and treatment benefits. While chemoprophylaxis may impact VTE rates, exposure to these prophylactic medications can itself have serious side effects, including adverse bleeding events or even death.6 A more precise understanding of the risks and incidence of VTE following below knee surgery would enable surgeons to select anticoagulant treatment strategies based on evidence. Moreover, reliable prediction of VTE incidence would enable a more shared decision making process between patients and surgeons as to managing one of the potential major risks of undergoing below knee surgery. Few studies have examined the incidence of VTE in the below knee surgery population with appropriately controlled and powered scientific methodology. The common method utilized in these studies to identify a VTE event is through International Classification of Diseases (ICD) procedure codes.7-12 Several studies, however, have suggested that this method can be inaccurate.13-17 As ICD-10-CM codes were only recently introduced in the United States, and this was a retrospective study, we reviewed ICD-9-CM codes. Our primary study aim was to determine the incidence of VTE in a large cohort of patients having undergone below knee surgery, and secondarily to assess the validity of using ICD-9-CM codes to identify a VTE event in this population.
Study design and participants
This retrospective study was approved by the Institutional Review Board, and a waiver of informed consent was granted. Two hundred sixty-one Current Procedural Terminology (CPT) codes and 87 ICD-9-CM codes were used to identify patients who underwent below knee surgery between August 1, 2005 and July 31, 2015 in a single hospital network (Appendix 1). Medical record data of patients with one of these CPT codes and ICD-9-CM codes were retrieved through our Research Patient Data Registry (RPDR). The RPDR is a centralized clinical data registry that comprises diagnostic (ICD-9-CM) codes and billing (CPT) codes, demographic information (e.g. sex, date of birth, and race), clinical encounters, transfusion data, laboratory values, and operative and radiology reports. Exclusion criteria were (1) patients younger than 18 years of age; (2) postoperative follow-up less than 90 days; (3) presentation of VTE on admission. Only the first below knee procedure was included when a patient had multiple below knee procedures.
Outcome Measures
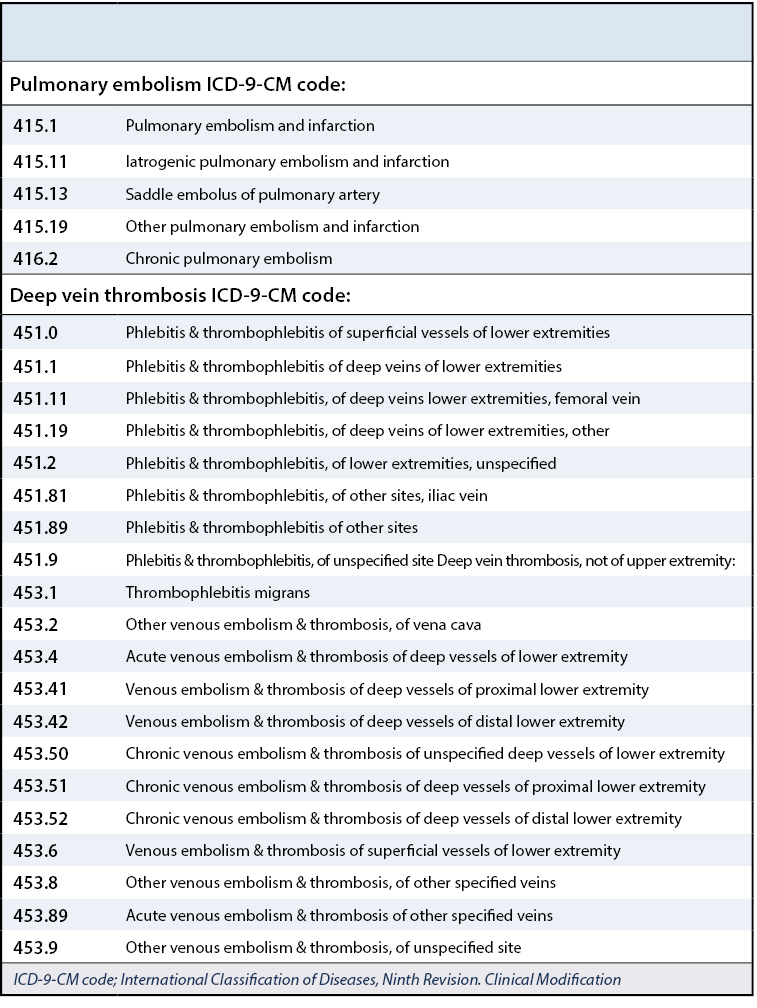
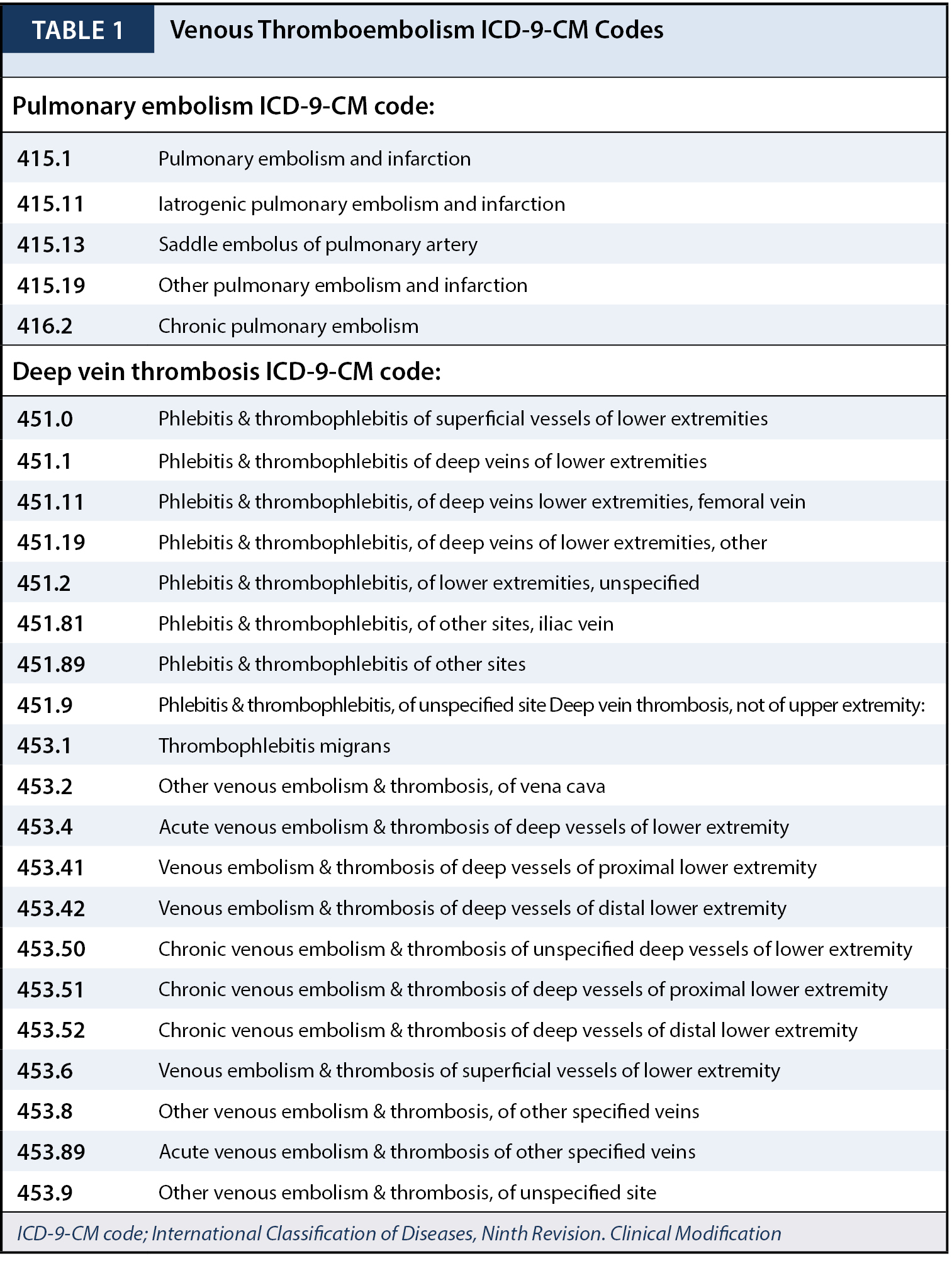
The outcome variables of interest were symptomatic PE and DVT of the lower extremity, iliac vein, or inferior vena cava, within 90 days of below knee surgery. These complications were identified (“flagged”) through specific and unspecific VTE ICD-9-CM codes (Table 1). Radiology reports of all patients were manually evaluated by two abstractors (RH, BL) to assess validation of ICD-9-CM codes against the documentation of DVT or PE in radiology reports. ICD-9-CM codes were defined as correct for a PE if its occurrence was proven by angiogram, magnetic resonance imaging (MRI) or computed tomography (CT) scan, and correct for a DVT if its occurrence was proven by magnetic resonance venography (MRV) or ultrasound. Patients with a DVT in the upper extremity, identified through unspecific DVT ICD-9-CM codes and confirmed by radiology reports, were excluded from analysis. Although we expect that the majority of patients received one or several forms of VTE prophylaxis, we were unable to stratify this specifically.
Data Analysis
We calculated the positive predictive value (PPV) of the ICD-9-CM codes by comparing the number of VTE patients identified with both ICD-9-CM codes and radiology reports abstraction (true positive) divided by the number of true positive patients plus the number of patients who were flagged with ICD-9-CM codes but had negative VTE radiology reports (false positive). We calculated the sensitivity of the ICD-9-CM codes by comparing the number of true positive patients divided by the number of true positive patients plus the number of VTE patients, identified with abstraction of radiology reports, who were not flagged with an ICD-9-CM code (false negative). All medical records of false positive patients underwent further detailed review to better understand why they were incorrectly flagged. Stata (Stata version 13, Statacorp LP, College Station, Texas, United States) was used for all data analyses.
There were 23,206 patients identified who had undergone below knee surgery between August 1, 2005 and July 31, 2015. One thousand two hundred sixty-two patients met one of our exclusion criteria. Additionally, 40 patients with upper extremity DVT who were identified through unspecific DVT ICD-9-CM codes and radiology reports were then also excluded from analysis, leaving 21,904 patients. There were 11,163 female (51.0%) and 10,767 male (49.0%) patients, with a median age of 50 years (interquartile range 37 to 62 years).
Venous thromboembolism flagged with ICD-9-CM codes
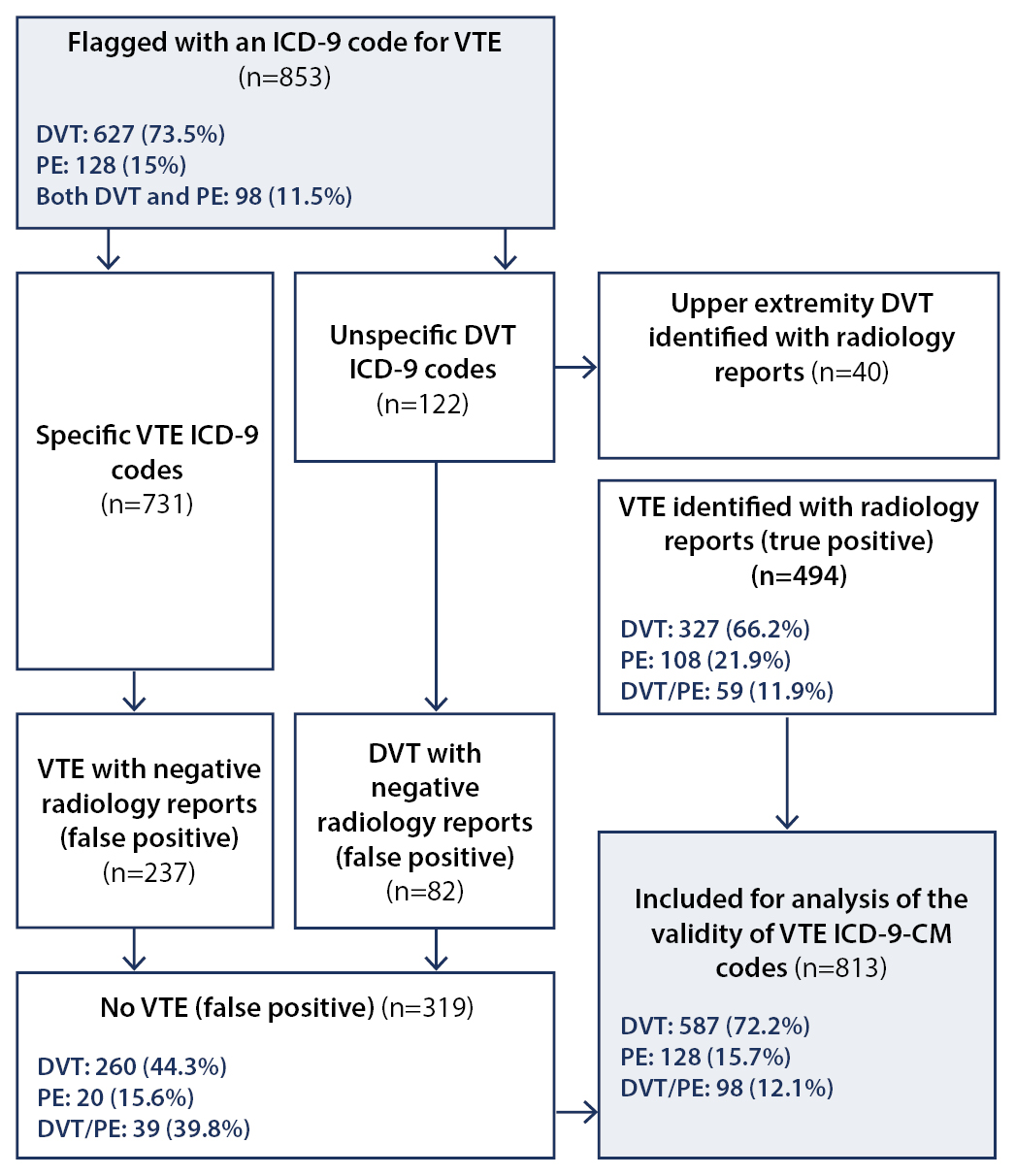
Eight hundred fifty-three patients had specific and unspecific ICD-9-CM codes for VTE after below knee surgery. Six hundred twenty-seven (73.5%) patients had a DVT of the lower extremity, iliac vein, or inferior vena cava, 128 (15.0%) patients were documented to have a PE in isolation, and 98 (11.5%) were found to have combined DVT/PE—even though theoretically it is recognized that any patient identified with a PE has by definition already sustained some form of systemic DVT, be it recordable or not. The 40 patients (4.7%) with an isolated upper extremity DVT, identified through ICD-9-CM codes and confirmed by radiology reports, were excluded from this further analysis. Four hundred ninety-four patients were identified as true positive, and 319 patients were identified as false positive (Figure 1). Reasons for false positive ICD-9-CM codes included: (1) DVT in the upper extremity while having specific ICD-9-CM code for DVT in the lower extremity, iliac vein, or inferior vena cava (n=28; 7.8%); (2) administration of VTE prophylaxis in the absence of VTE (n=65; 18.2%); (3) diagnosis or procedure for arterial stenosis (n=58; 16.2%); (4) thrombosis of an arterial bypass (n=12; 3.4%); (5) Prior history of DVT or PE (up to 15 years prior) (n=66; 18.4%); (6) Suspicion of DVT or PE (n=129; 36.0%).
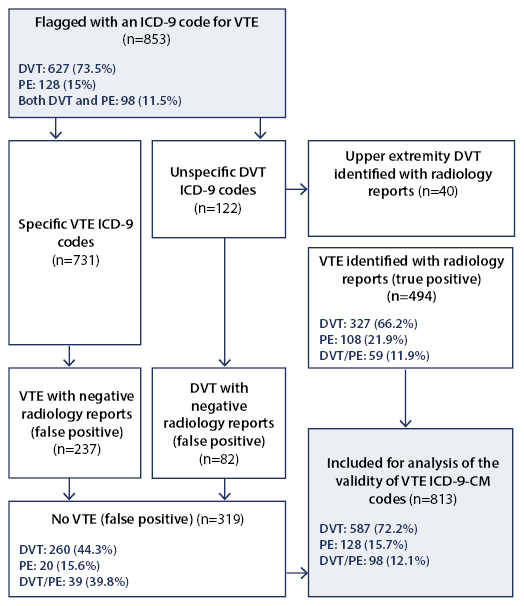
Flowchart showing used method for selecting patients for analysis of the validity of International Classification of Diseases, Ninth Revision, Clinical Modification codes.
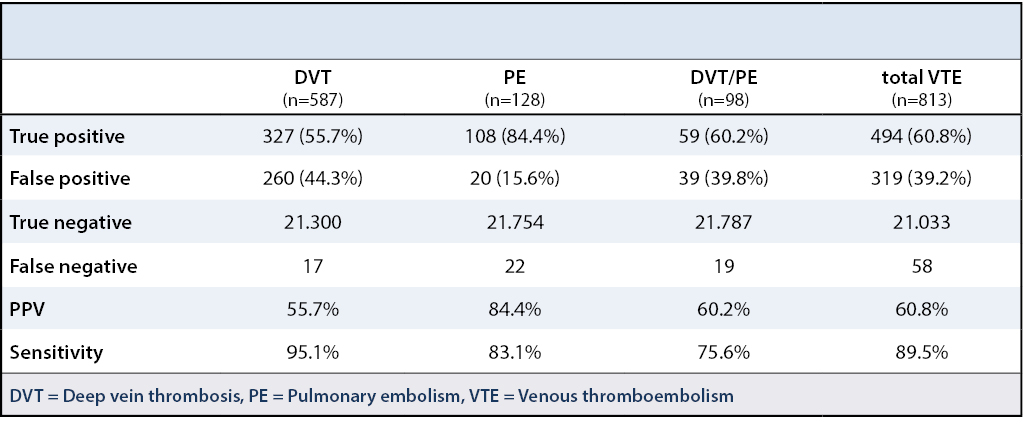
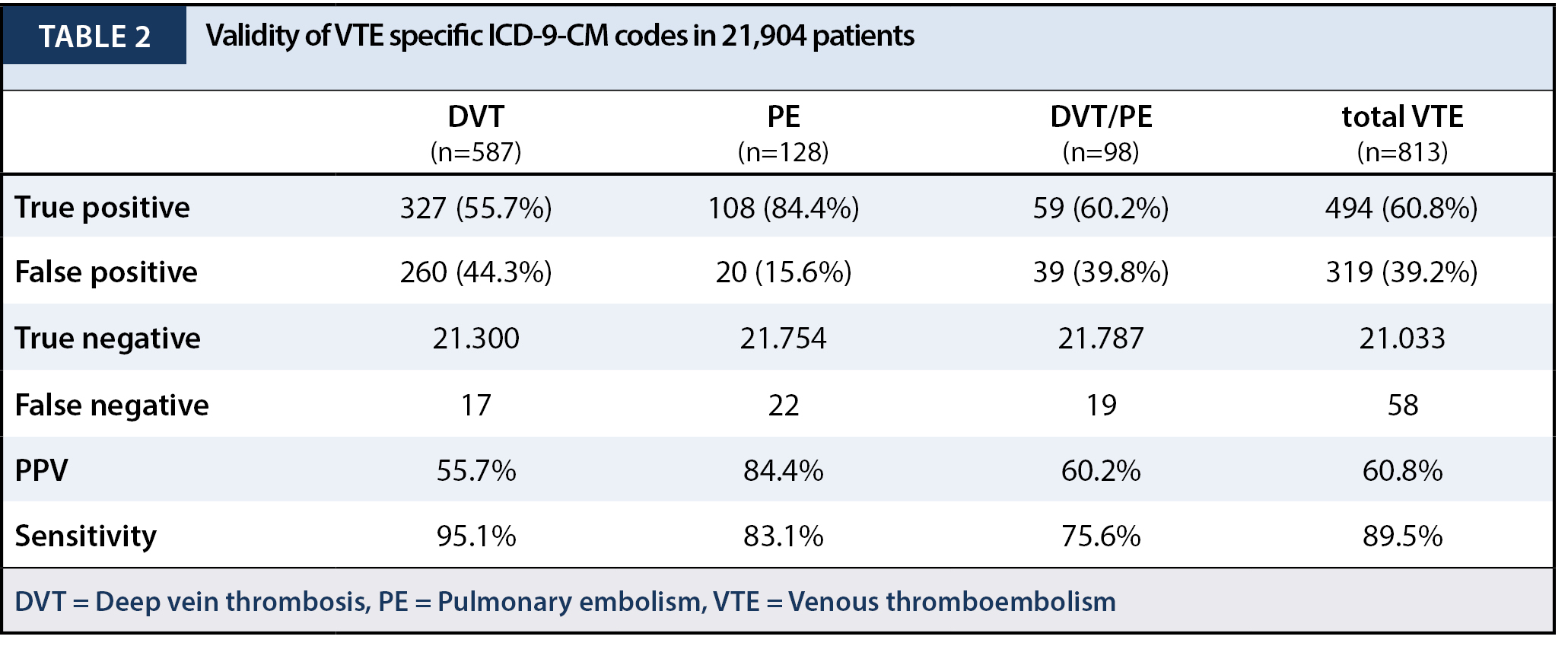
The resulting PPVs of ICD-9-CM coding were 55.7% (327/587) for DVT, 84.4% (108/128) for PE, 60.2% (59/98) for combined DVT/PE, and 60.8% (494/813) for VTE in total. The resulting sensitivity scores were 95.1% (327/344) for DVT, 83.1% (108/130) for PE, 75.6% (59/78) for combined DVT/PE, and 89.5% (494/552) for VTE in total (Table 2).
To determine the incidence of VTE after below knee surgery, previous studies have used specific ICD-9-CM codes for identifying VTE.7,8,10 We assessed the accuracy of these ICD-9-CM codes in a large cohort of patients who underwent surgery below the knee, and found that the overall PPV was 60.8% and the sensitivity was 89.5%.
The overall incidence of VTE following surgery below the knee was 2.5%. It should also be pointed out in noting this figure, however, that many of these patients had received one or several forms of VTE prophylaxis. These data do not, therefore, represent the true incidence or natural history of VTE following below knee surgery in the absence of VTE prophylaxis—which was not the intent of this investigation.
Other studies have also revealed inaccuracies in VTE ICD-9-CM codes based on reporting that is similar to the results shown in our study. White et al. found the PPV for post-operative lower extremity VTE to be 44% in the University HealthSystem Consortium cohort and 48% in an Agency for Healthcare Research and Quality sample.17 Zahn et al. took random samples of medical records abstracted for a patient safety program at the Centers for Medicare & Medicaid Services.15 In their sample, the PPV of ICD-9-CM coding were 31% for DVT, 24% for PE, and 29% for DVT/PE combined. The resulting sensitivity scores were 67% for DVT, 74% for PE, and 68% for combined DVT/PE. Two other studies showed a comparable low PPV.14,18 These findings illustrate the use of retrospective ICD-9-CM based data capture methodologies as a potential source of inaccuracy, therefore, and suggest that this weakness be considered in interpretation of any past or future assessment of VTE incidence when such scientific methods are employed.
Although ICD-10-CM codes are now increasingly being used in the United States, we expect our findings to be relevant for both ICD-9-CM and ICD-10-CM codes. The difference between ICD-9-CM and ICD-10-CM codes is the expanded number of characters of the ICD-10-CM diagnosis codes, which provides greater specificity to identify disease etiology, anatomic site, and severity.19,20 However, the current method used for flagging VTE remains unchanged.
The VTE incidence rate in this sample was 2.5%. This is within the wide range of symptomatic VTE incidence rate (0.3% - 23%) found in previous studies.8,12,21-25 Shibuya et al. analysed the National Trauma Database and found that in 74,469 patients the VTE incidence rate was 0.49%.8 In a prospective study performed by Solis et al., 7 out of 201 patients (3.5%) who had undergone surgery below the knee developed VTE.24 Wahlsten et al. retrospectively studied 57,619 patients who were operatively treated for a fracture distal to the knee. One percent of them had a postoperative DVT or PE.12 Prior studies found lower VTE incidence rate compared to the incidence rate in our patient cohort.7,8,10-12,26 These studies, however, provided no detailed information on the peri- or postoperative anticoagulant strategies that were used. Therefore these studies might not accurately represent the true VTE incidence rate. Moreover, some of these studies looked at the VTE rate after foot and ankle surgery, while we also included patients who had below knee surgery.7,10,11,26 Our data suggest that patients who undergo below knee surgery are of highest risk of developing VTE. Future research on the incidence of VTE following below knee surgery should provide information on post-operative anticoagulant strategies that are used, so that study outcomes can be put in better perspective.
This study has several limitations, including the fact that it is retrospective in nature. First, our study sample consisted of patients who were seen in a single hospital network—and coding practices may vary from other hospitals. Coding practice may also vary among individual coders, and this source of variation was not determined. Second, we abstracted radiology reports to identify patients who developed VTE within the hospital network, which does not capture those people diagnosed with VTE outside this network. Therefore this analysis may have missed patients who developed VTE in an outside hospital. This study also relied on diagnosed patients as a result of having a symptomatic VTE. Thus, since this population was not routinely screened for asymptomatic VTE, these data may potentially underestimate the true incidence of VTE in this population that often received perioperative prophylaxis. Finally—and in relation to the aforementioned comment—while assessing the incidence of symptomatic VTE following below knee surgery, we did not determine the anticoagulant strategies that were used and therefore cannot comment on either the true natural history of VTE in this population nor the postoperative effectiveness of various treatment strategies.
The overall rate of VTE following below knee surgery in this large cohort of patients was 2.5%. Using ICD-9-CM codes to identify VTE rates in this population appears to have a sensitivity of 89.5%. Only roughly half (60.8%) of the ICD-9-CM codes used for identifying VTE could be verified by a radiological study, however, which demonstrates this methodology as having a fairly low PPV. Through comprehensive assessment of the incidence of VTE following below knee surgery, we illustrated a potential source of inaccuracy in the use of retrospective ICD-9-CM based data capture methodology for this disease entity.






{kind=link}
{kind=link}
{kind=link}