
Outcome of Surgical Fixation of Complex Clavicular Nonunion with Segmental Defect
Arvind von Keudell, MD and Jesse B. Jupiter, MD
The authors report no conflict of interest related to this work.
©2016 by The Orthopaedic Journal at Harvard Medical School
 PDF
PDFOBJECTIVE The purpose of this study is to report on the operative treatment of a unique cohort of clavicular nonunions with a major segmental bony defect.
DESIGN Restrospective Review
Setting Level 1 Trauma Center
METHODSBetween 1996 and 2014, 20 patients with a complex clavicular nonunion and a segmental defect treated with open reduction, intercalary corticocancellous bone graft and internal fixation were retrospectively reviewed.
The main outcome measurements included union rates, complications, functional outcome and the range of shoulder motion. Disabilities of the arm, shoulder and hand (Quick DASH) score, and pain scale were evaluated at the last follow-up.
RESULTS The mean age of patients was 38 years with range of 24- 69 years at the time of surgery. Union was achieved in all cases with one patient requiring a second procedure to gain union. The average final range range of motion was near normal when compared the contralateral extremity. At final follow-up at an average of 36 months (range 12- 60 months), the Quick DASH averaged at 22± 10 points, and 1/10 pain on the VAS pain scale.
CONCLUSION Outcome of open reduction and internal fixation of ununited clavicles with segmental defects can result in high union rates with acceptable outcome scores, high patient satisfaction and a low reoperation rate.
The clavicle has been postulated in the early 20th century as one of man’s greatest skeletal inheritances.1 It is the connection between the axial and appendicular skeleton and fucntions as the key (clavicula - little key in Latin) between those two systems, facilitating and optimizing the function of the upper extremity. The anatomic relationships of the sternoclavicular joint and acromioclavicular joint with their respective ligamentous structures, represent a confluence of two rotational joints. This complicates attempts to restore physiologic length and rotation to recreate normal shoulder girdle biomechanics in the setting of an injury.
Fractures of the clavicle have been estimated to have an incidence of approximately 10% of all fractures. Fortunately, most clavicle fractures heal without surgical intervention. In the past decade, several randomized controlled studies have tried to elucidate whether surgical intervention has a role in the treatment of clavicle fractures, and this remains debatable.2-5 Many would argue for surgical fixation with the rationale that anticipated healing is impaired if various risk factors, such fracture displacement, comminution and shortening are present.
Failure to heal after surgical intervention can present a substantial functional deficit including pain, restricted motion, and ptosis of the shoulder girdle with associated symptoms of a brachial plexus compression.2,6,7
Ununited fractures with a segmental defect caused either by synovial pseudoarthrosis, unstable internal fixation or chronic infection can be challenging to the treating orthopaedic surgeon. A dysfunctional limb may be even more prevalent in these patients, as a shortened clavicle by 1.5cm or greater has been observed to significantly cause functional difficulties.8,9 We therefore make the argument that an attempt should be made to restore clavicular anatomic length to potentially maximize the function and rotation of the shoulder girdle.
We report on the outcome of 20 patients with clavicular fracture nonunion with an average segmental defect of 3cm, who underwent surgical fixation with an autogenous corticocancellous bone graft.
Patients
In this institutional review board approved study, we reviewed the experience of the senior surgeon from 1994 to 2014.
There were 20 patients with an average age of 38 years (range: 24-69 years) at the time of surgery. All presented over a period of 18 years with clavicle fractures that went on to nonunion, with a segmental defect measuring 3cm. The average duration of the nonunion was 40 months (8-100 months), with the exception of one patient who had a documented nonunion for 42 years. Proprionibacterium acnes (P. acnes) infection was present in 5 out of the 20 patients. The indications for surgical intervention included physical disability in all patients that was recalcitrant to nonsurgical treatment for more than 6 months, and neurologic comprise which was present in 6 patients.
Surgical Technique
Patients were positioned on a semi-sitting radiolucent table, and the opposite iliac crest was generally used for obtainment of autograft unless anatomic variants precluded. A straight incision was centered along the inferior aspect of the long axis of the clavicle.
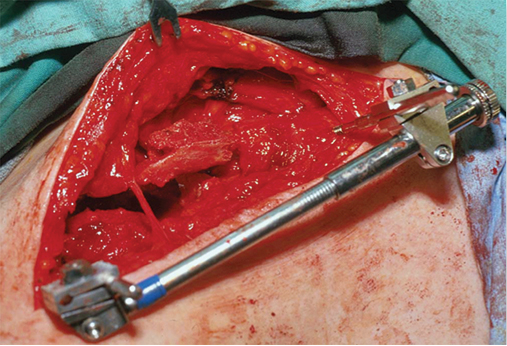
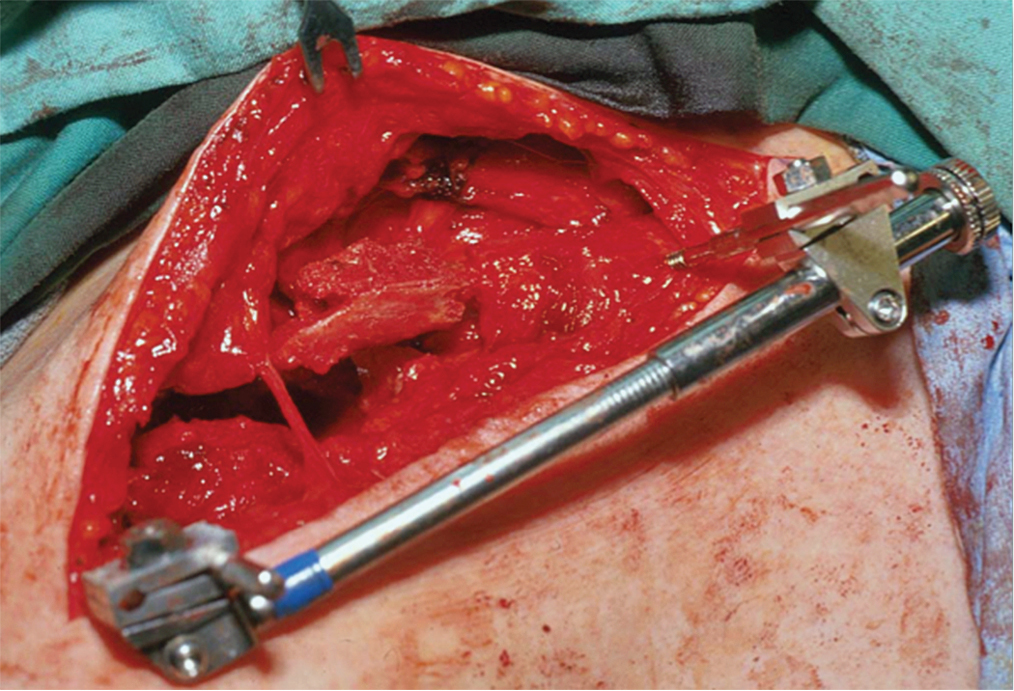
Once identification of both ends of the ununited clavicle was completed, the use of a small distractor was used to restore length, alignment and rotation. It facilitated the assessment of length and dimensions of the bony defect.
The bony ends of the each segment were opened into the medullary canal with a 3.2mm drill bit to stimulate the bone-healing unit, and to create a cavity that would accept the corticocancellous autograft from the iliac crest.
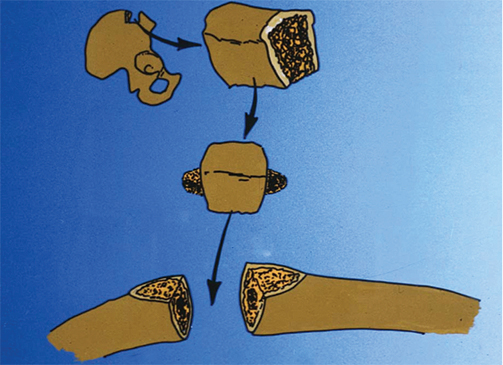
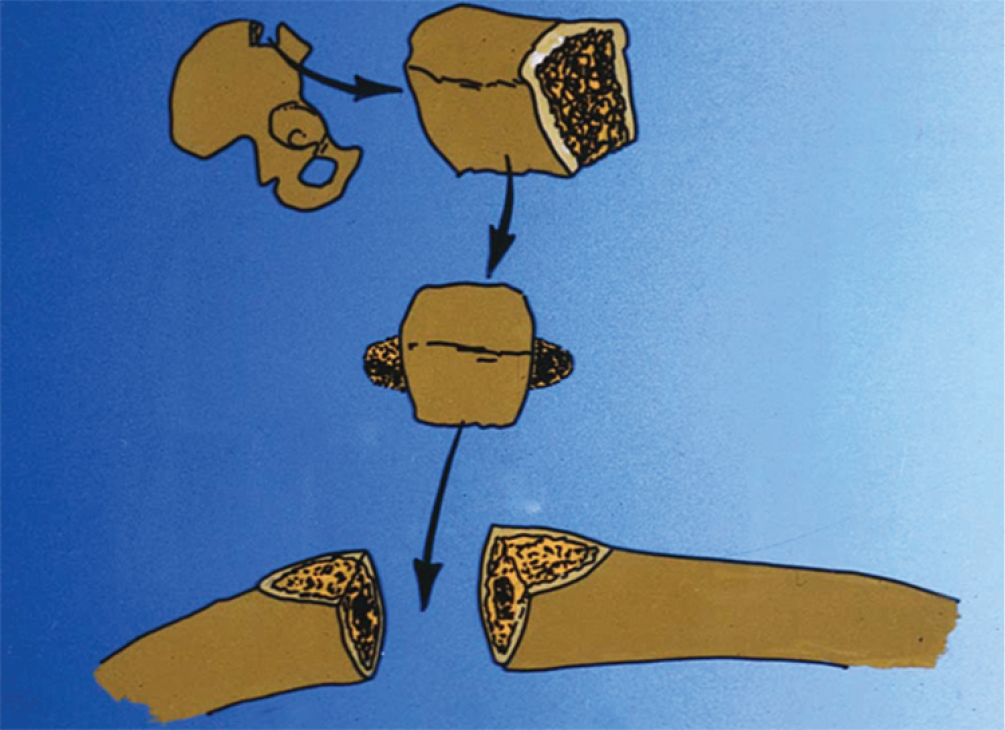
The iliac graft was obtained form the iliac crest. A tricortical section of the iliac crest was harvested at 1.5 times the size of the measured bony defect using osteotomes and an oscillating saw. The graft was shaped to fit the defect with bilateral large pegs that facilitated interdigitation. It was subsequently positioned in the defect with the dorsal cortical margin of the iliac crest on the inferior surface of the clavicle to improve screw purchase and increase resistance against bending forces.10,11
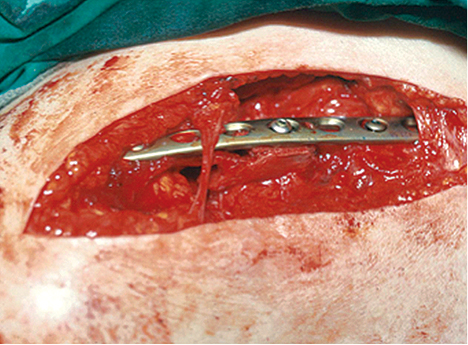
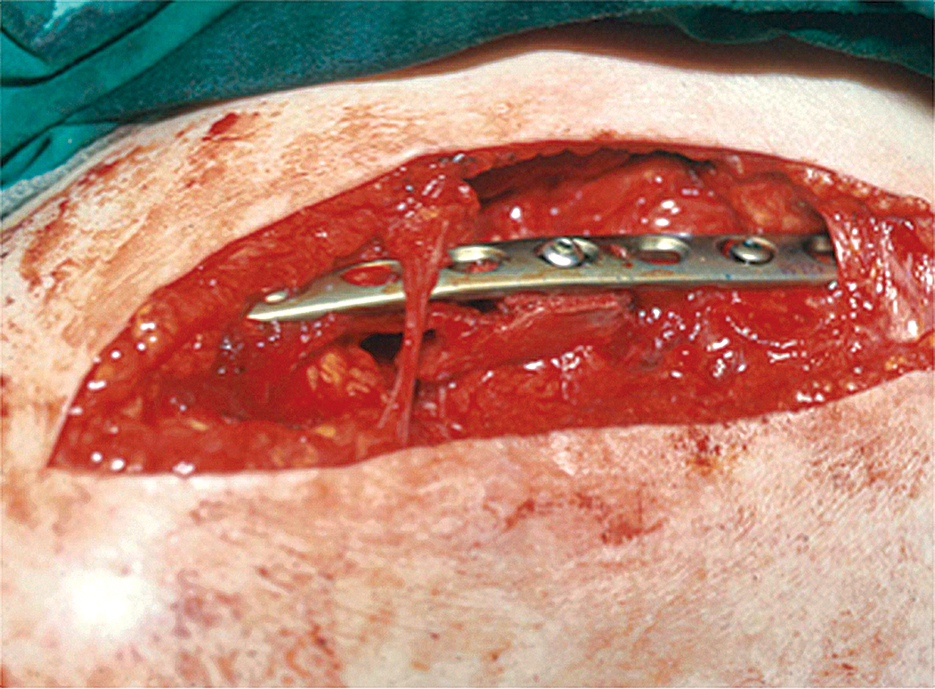
Fixation was achieved with the use of a 3.5mm limited contact dynamic compression plate (Depuy, Synthes, PA, USA) and in 3 cases was augmented with a second smaller plate on the anterior surface. A minimum of 3 screws in compression mode were applied on either side with an additional screw placed into the harvested graft (Figures 1-3).
Additional plating techniques included precontoured plates for additional compression, and wave plate technique to allow for improved bony healing.
A sling was then prescribed for seven to ten days provided the fixation was deemed to withstand early range of motion of the shoulder girdle. Once early bony healing was apparent on radiographs, progressive strengthening exercises were implemented. At 3 months postoperatively, patients were encouraged to return to their occupational or recreational activities.
Follow-up
At a mean follow-up time of 38 months (range: 12 to 60 months) after the index procedure, the Quick Disabilities of the Arm, Shoulder and Hand (Quick DASH) Score and pain score were recorded. We also reviewed the final range of motion in the patients’ records at the time of the final follow-up visit.
20 patients with a complex ununited clavicle with a large segmental defect were treated with surgical intervention. The mean Quick DASH score at the final follow-up after mean time of 36 month (12- 60) was 22±10 points. The VAS pain score was 1/10.
The mean range of shoulder motion at the time of last follow-up visit was near normal in all cases. All patients returned to their occupational and recreational activities with improved physical function. Clavicular length was restored to within 1.0cm± 0.5cm when compared to the contralateral side.
No implant removal was performed within the study population. One patient with an infected nonunion required an additional procedure and he healed subsequently without further intervention. All patients demonstrated union of the clavicle at final follow-up.
Clavicle fracture nonunion with segmental defects are among the most complex fractures to treat, and it remains a challenge to obtain high functional outcomes for patients postoperatively. Most reports on simple clavicle nonunion are amendable to revision fixation with iliac crest bone graft and demonstrate a healing rate of 89-100%.12-14 However, there is scarce literature on the treatment on the subset of patients with clavicle nonunion with an additional large bony segmental defect.
Ballmer et al.15 reported on 37 patients with nonunion of the clavicle of which only 9 patients underwent tricortical iliac crest bone grafting for a segmental defect measuring > 1.5cm. All patients demonstrated union at their final follow-up.
Others have advocated for a free vascularized fibular graft. This has been successfully performed in 3 patients with persistent nounion of the clavicle.16
We report on 20 patients with this unique problem treated over a period of 18 years using screw and plate fixation in combination with a tricortical autograft from the iliac crest, and sculpturing pegs on each side to fit into each end of the nonunion site. It appears this technique may provide sufficient stability and an optimal biologic environment for reliable healing. Attention to the principles of surgical treatment of nonunions may result in consistent and reliable outcome. Key elements in the surgical technique include adequate bone debridement with observation of bleeding bone, the attempt to restore normal length, rotation and alignment in association with the various screw plate configurations, i.e. waveplate, precontoured compression plating or double plating.
Previous observations have reported on the usage of intercalary corticocancellous bone graft in ununited diaphyseal forearm fractures in 35 patients with radiographic evidence of healing within 6 months.17 Similarly, in a previous report10 this technique has been used in the treatment of ununited clavicle fractures. In three patients out of cohort of 23 patients with an unnited clavicle fracture, the use of a sculptured bone graft was necessary. It appears beneficial to place the subsequent plate superiorly to mimic tension band technique, as the ends of a clavicular nonunion most commonly are directed superiorly creating a tension and compression side.18
Special attention should be given to the possibility of P. acnes infection. Underlying P. acnes infection may represent a larger percentage of clavicular fracture nonunion than anticipated.19 In this series, there were five patients suffering from P. acnes infection and had been treated with intravenous antibiotics. It largely remains unknown how many ununited clavicle fracture treated initially with open reduction and internal fixation are due to an underlying infection.
There are a few notable limitations to this study. Although we report a considerable number of patients, the sample size is not sufficient for subgroup analysis. This is a retrospective study, which makes it inherently more susceptible to misleading data and bias. Additionally, we did not have a control group for comparison.
In conclusion, for patients with symptomatic complex ununited clavicle fractures with large segmental defects, open reduction and internal fixation with corticocancellous intercalary bone graft remains a viable surgical option to maintain a long-term high functional outcome and reliable fusion.





{kind=link}
{kind=link}
{kind=link}