
Atraumatic Late Screw Loosening of the Tibial Polyethylene Insert Locking Mechanism in a Constrained Knee Arthroplasty: A Case Report
Arvind von Keudell, MD, Kshitijkumar Agrawal, MD, Harry E. Rubash, MD
The authors report no conflict of interest related to this work.
©2016 by The Orthopaedic Journal at Harvard Medical School
 PDF
PDFCASE We describe a case of middle-aged woman who had undergone a total knee arthroplasty with a Zimmer NexGen Legacy Constrained Condylar Knee (LCCK) (Warsaw, IN). Nine years later, an atraumatic failure of the locking mechanism of the polyethylene insert and the tibial base plate occurred. There was no evidence of loosening of either tibial or femoral components. The patient underwent revision surgery with reinsertion of another tibial base plate and locking mechanism.
CONCLUSION There may be a role to monitor patients with a LCCK prosthesis for the occurrence of asymptomatic screw loosening on a yearly basis, especially if there is clinical suspicion.
The condylar constrained knee arthroplasty is used to provide a stable knee in patients with extensive bone loss demonstrating a flexion or extension gap imbalance or in patients with severe deformities with soft tissue contractures and ligamentous laxity.1-7 Other indications include neuropathic arthropathy and rheumatoid arthritis that present with severe varus or valgus deformities. Once the decision is made that a posterior stabilized total knee may not provide sufficient stability, a non-linked constrained knee design may be used. It allows limited rotation, medial lateral translation and limited varus-valgus angulation. Constrained knee implants use a pin or screw to stiffen the post to withstand the increased forces across the implant. Kim et al.5 has reported on 14 patients undergoing total knee arthroplasty with a constrained knee design. At an average of 6.3 years there were no failures. Other authors have reported complications including aseptic loosening, patellar maltracking resulting in patella fracture and polyethylene wear.8
To our knowledge, there are only four other studies reporting on patients with screw disengagement from the locking mechanism most commonly due to a traumatic event9-12 or loosening from the femoral component with migration into the joint in older prosthesis versions, such as the Insall- Burstein-II constrained condylar knee prosthesis.13 Screw loosening is an uncommon complication and can lead to metallosis with backside wear and failure of the locking mechanism that may require revision total knee arthroplasty.
We present a unique case of atraumatic loosening of the locking mechanism 9 years after initial surgery with a constrained total knee design.
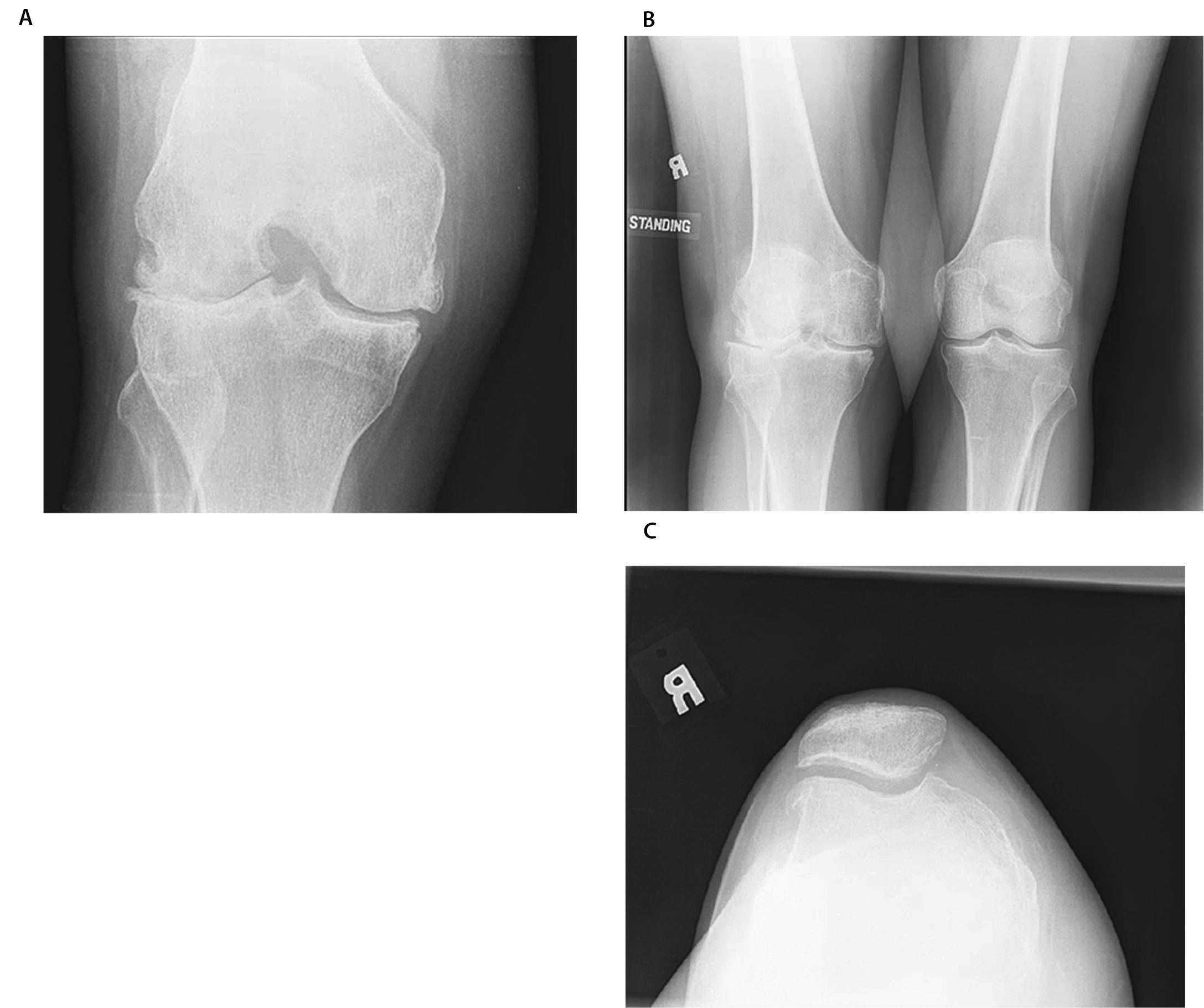
The patient is a fifty-four-year-old woman with a fifteen-year history of rheumatoid arthritis and end stage tricompartmental joint disease with osteophytosis in her right knee and significant soft tissue contracture with valgus deformity. She previously underwent partial medial meniscectomy. She also had a distant history of open synovectomy for rheumatoid arthritis that was complicated by postoperative infection. The patient’s knee examination before surgery was significant for a 15 degree valgus deformity and range of motion from 15- 90 degrees that was uncorrectable. On radiographs, the right knee showed tricompartmental disease affecting primarily the lateral compartment (Figure 1). She was treated with a Legacy Constrained Condylar Knee (LCCK, NexGen, Zimmer, Warsaw, In) in September 2003.
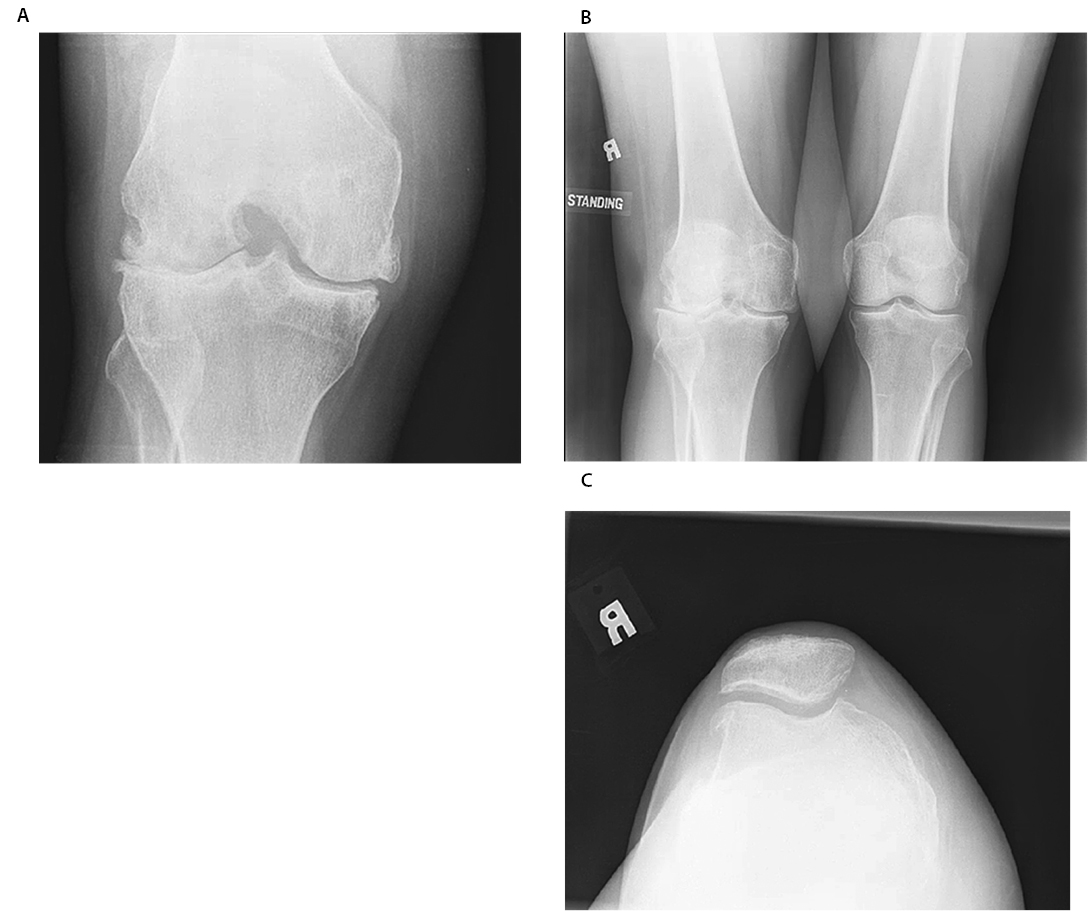
(A, B, C) Three views of the right knee demonstrating loss of joint space, particularly laterally, and osteophyte formation
Extensive lateral release was performed including the lateral collateral ligament and the iliotibial band. The LCCK prosthesis with tibial and femoral intramedullary stems was implanted. The components were fixed with tobramycin-impregnated cement. The polyethylene was inserted and fixed with a locking screw to reinforce the junctions as described by the technique guidelines by the manufacturer. This entails tightening of the screw to a fixed tension with a torque-measuring screwdriver.
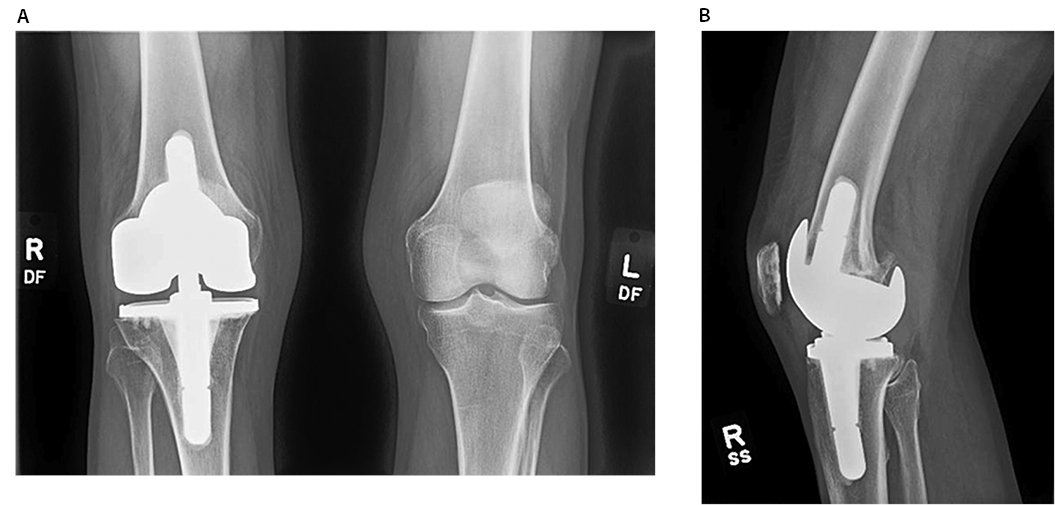
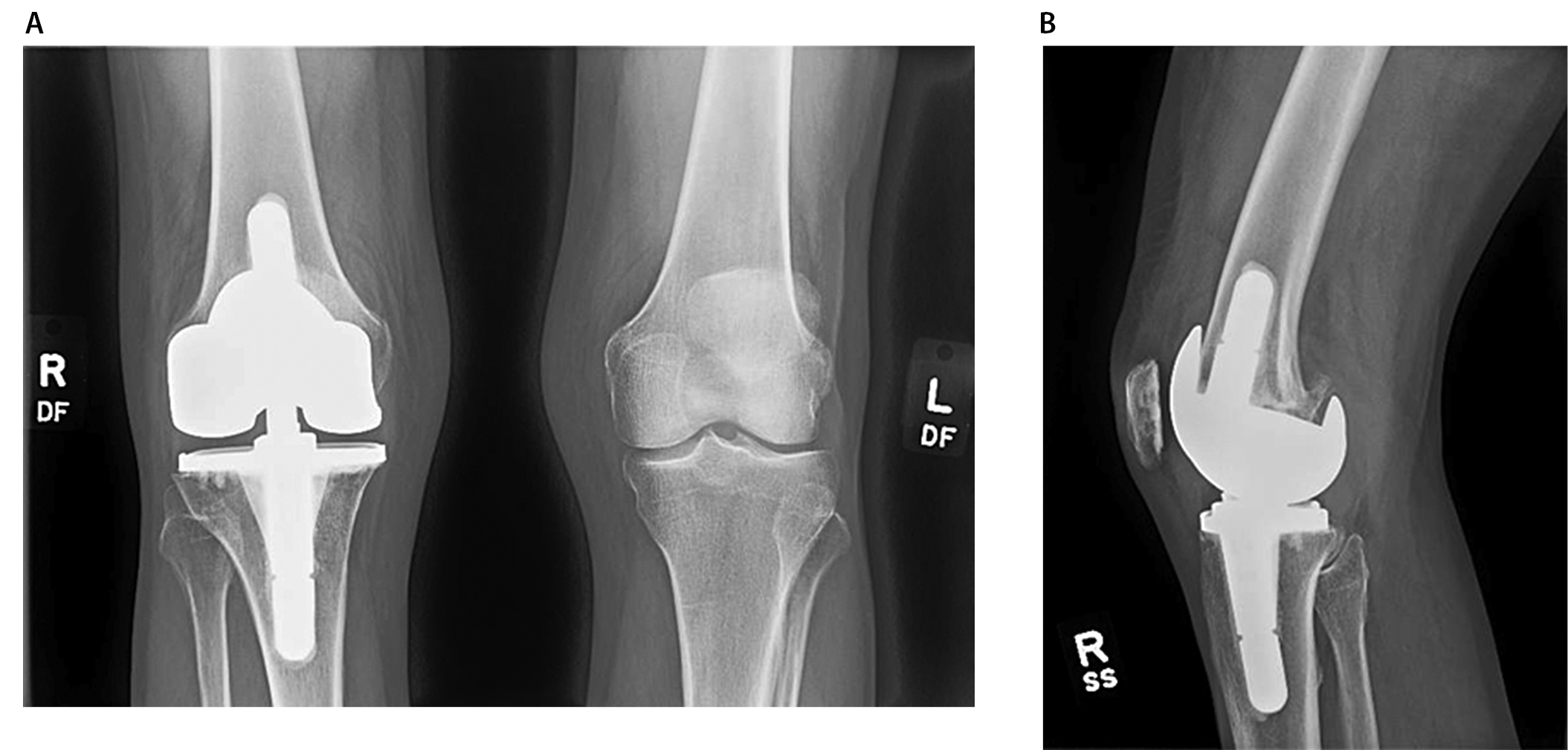
The patient did not experience any postoperative complications and physical examination demonstrated active range of motion of 0 to 115 degrees with neutral alignment until 9 years postoperatively. She had no signs of wear on serial follow-up radiographs and returned to basic recreational activities without pain (Figure 2).
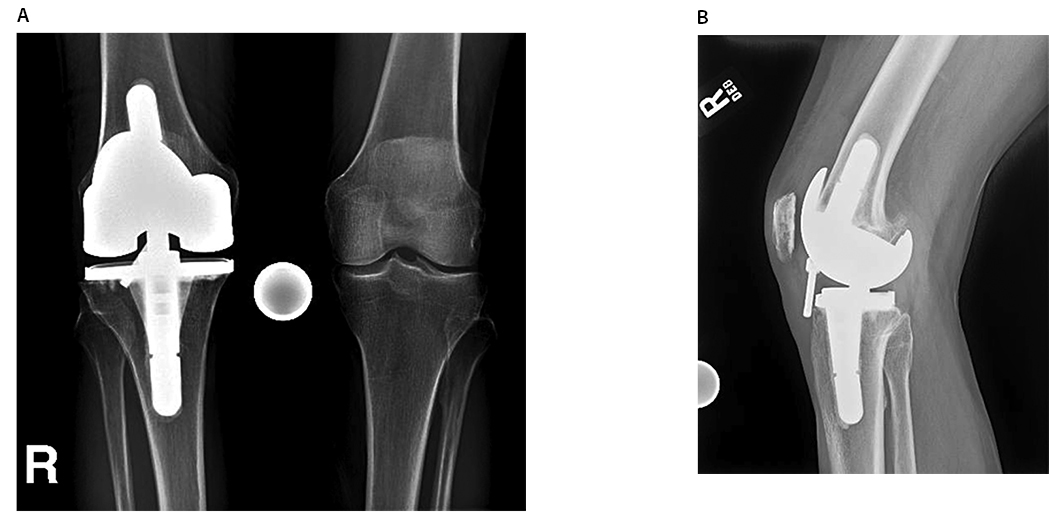
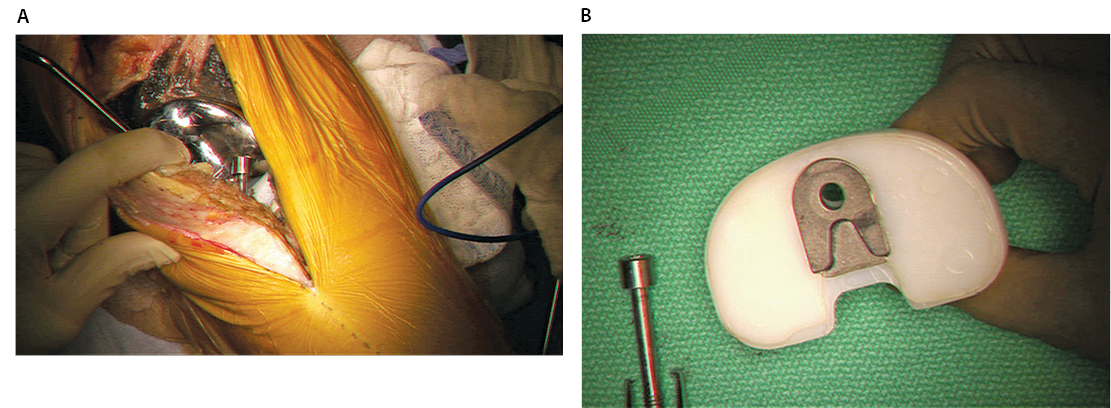
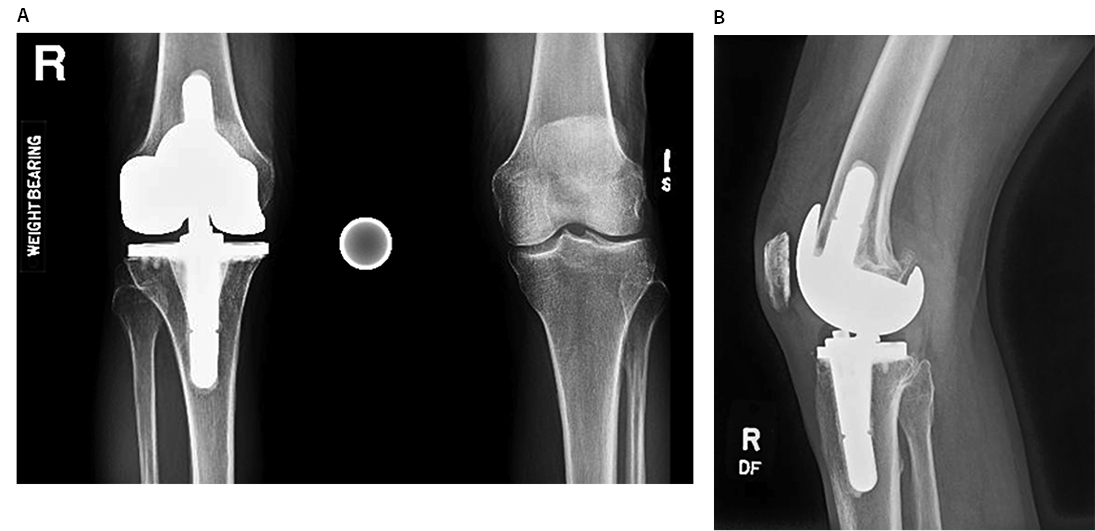
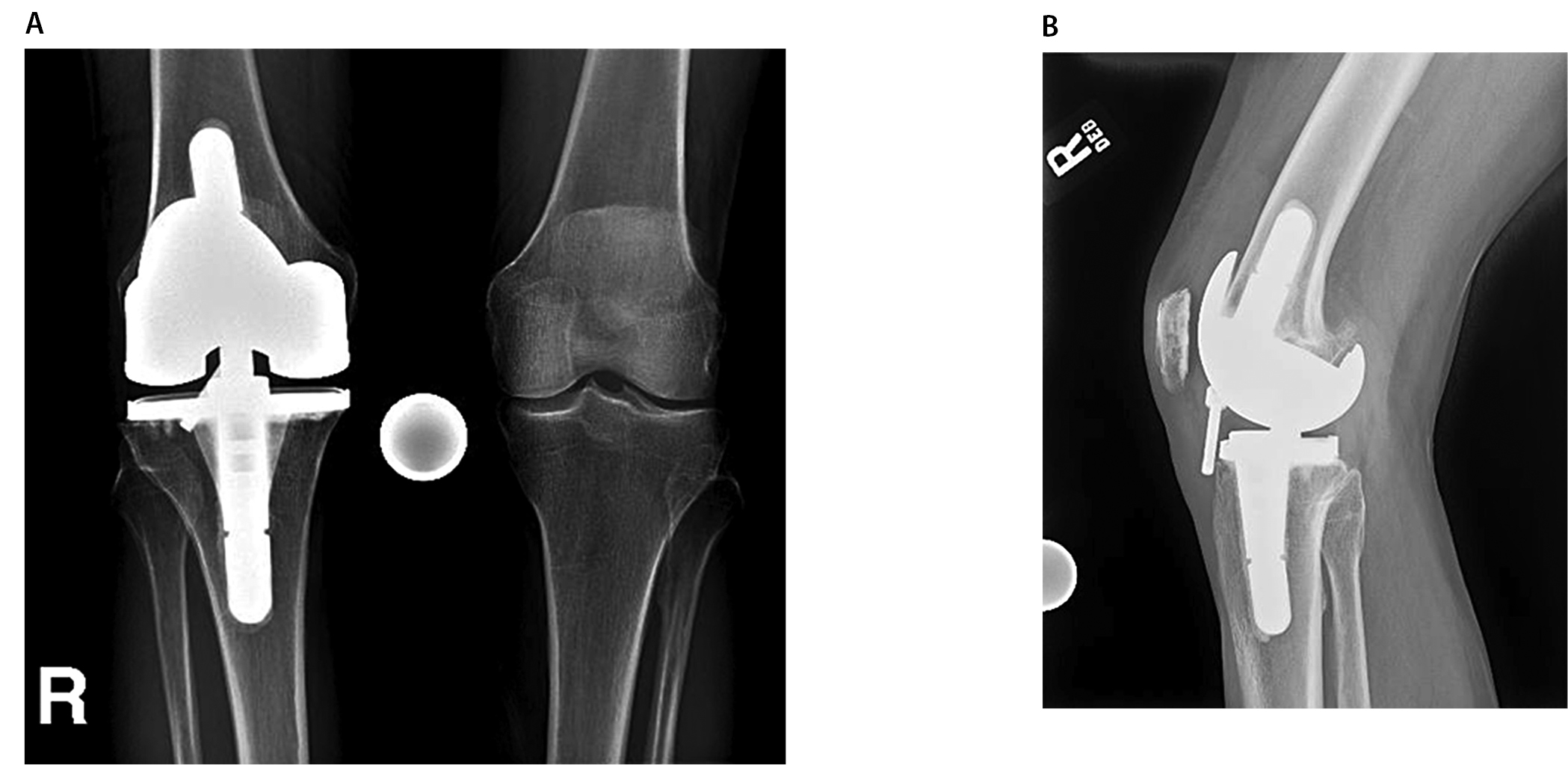
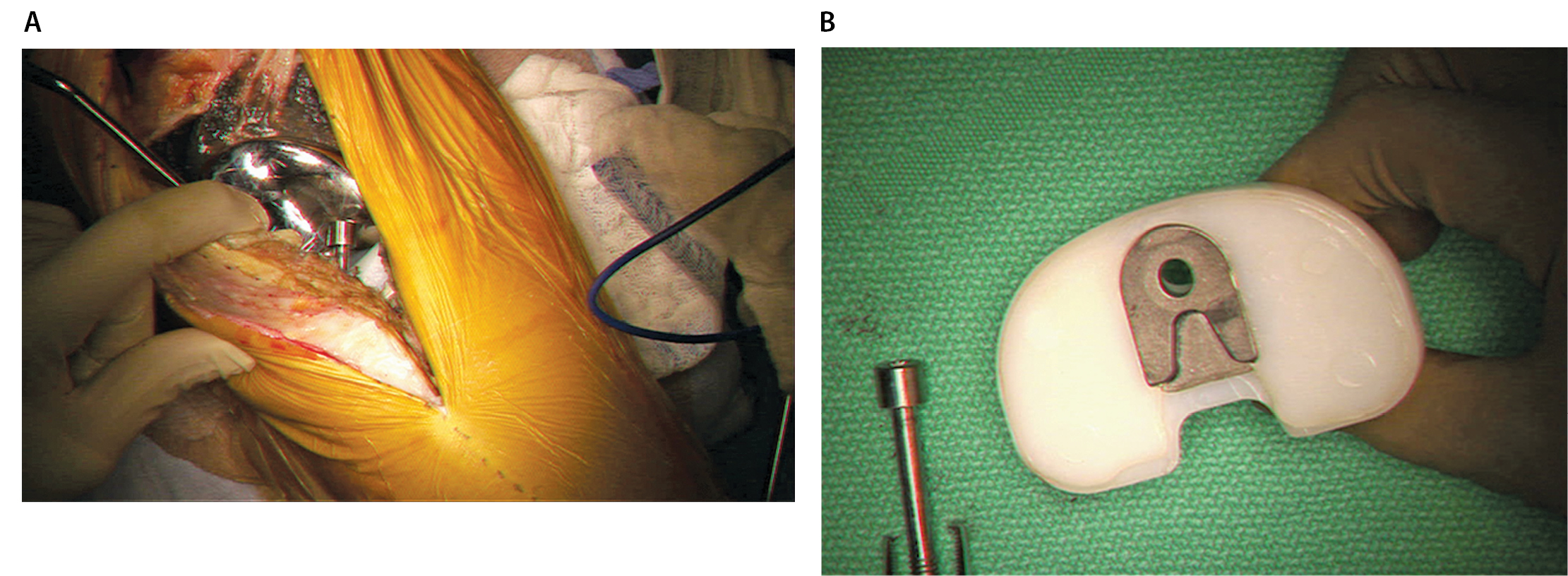
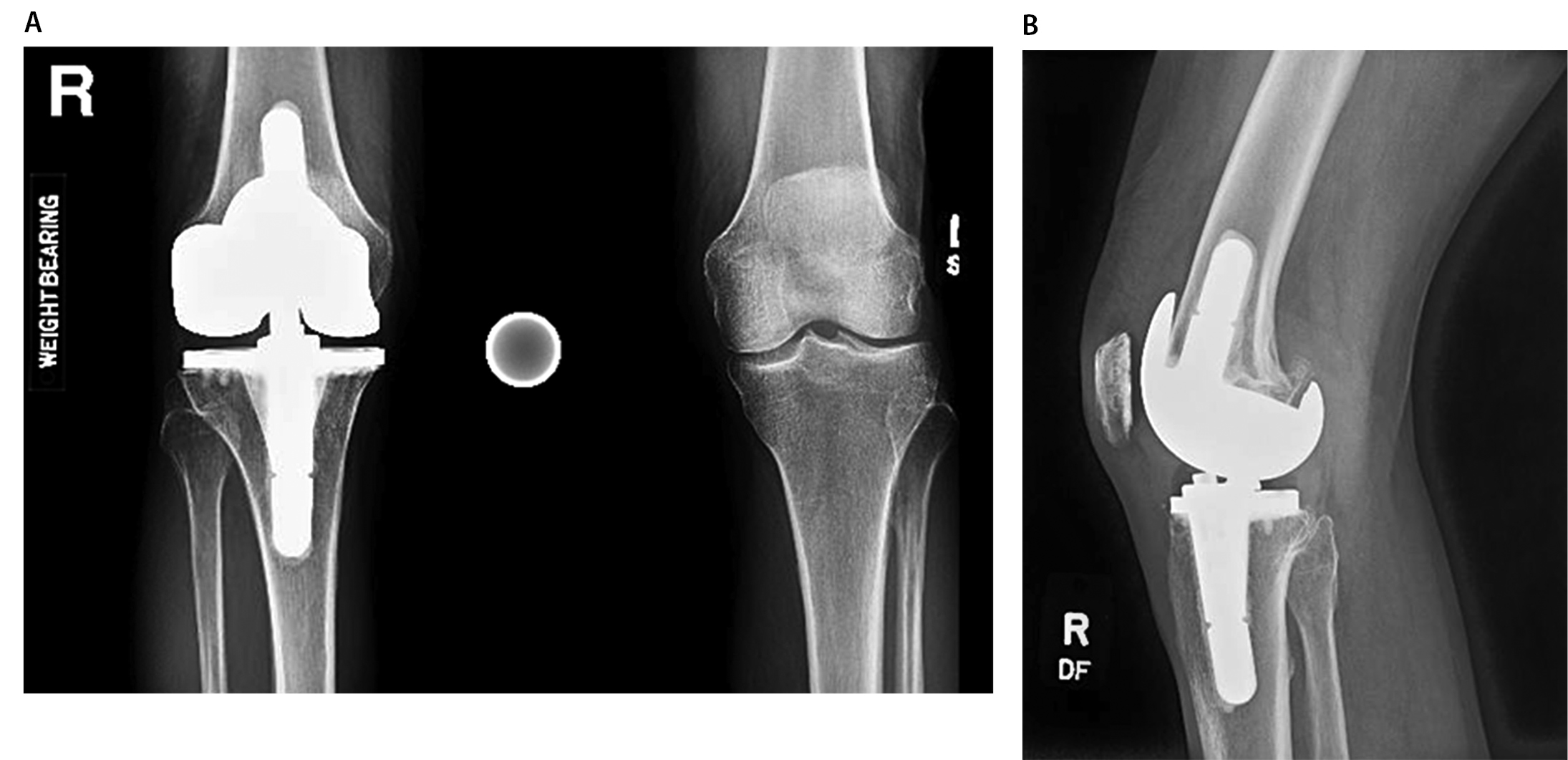
She re-presented in February 2013 with sudden onset of acute right knee pain and clicking without a history of trauma. On physical examination the knee had active range of motion from 0 to 115 degrees and no instability but demonstrated clicking in mid-flexion. Radiographic imaging demonstrated a loosened screw with no evidence of breakage or any loosening of the tibial and femoral components (Figure 3).The patient underwent a medial parapatellar arthrotomy with removal of the loosened screw, implantation of a new polyethylene liner as well as a new locking screw. Intraoperatively, the screw was apparent behind the patellar tendon and the joint demonstrated extensive metallosis in the suprapatellar pouch as well as in the lateral and medial gutters (Figure 4). The screw was intact with minimal evidence of wear, similar to the initial polyethylene liner, which was not disengaged. There was, however, evidence of backside wear over the tibial polyethylene metal insert. We performed extensive synovectomy to remove all visible metal debris and implanted a new liner with a new locking screw. The patient’s postoperative course was uncomplicated. At two-year follow-up, she remained pain free with active range of motion from 0 to 130 degrees with no ligamentous instability and symmetric foot progression (Figure 5).
The use of unlinked constrained knee prosthesis has demonstrated excellent long-term outcome studies with survivorship up to 96% at 10 years.6 Reported complications with the use of a constrained knee prosthesis are similar to unconstrained knee implants and include component loosening, deep infection, tibiofemoral instability, limited range of motion, extensor mechanism problems, fractures and wound problems.8,14,15 Constrained knee implants use a pin or screw to stiffen the post to withhold the increased forces across the implant. We report on late atraumatic screw disengagement in the Zimmer (Warsaw, IN) NexGen Legacy Constrained Condylar Knee (LCCK) prosthesis.
The additional constraint has shown to lead to increased stresses on the cement-implant interfaces as well as increase in micromotion between the insert and the tibial base plate that may cause backside wear and subsequent osteolysis.16 Some constrained designs use supplemental screw fixation to decrease micromotion. Only a few cases have reported on the disengagement of the locking screw from the tibial insert causing mechanical symptoms.9 The exact mechanism of this unusual complication has not been fully elucidated. Rapuri et al.9 hypothesized that counterclockwise torque which is created between the insert and the tibial tray due to the rotation of the femur on the tibia can cause disengagement. The authors postulated that micromotion at the backside of the insert on the baseplate likely allows this force to be transferred to the screw, and, over many cycles, may lead to screw loosening.
Another experimental hypothesis is that different material properties of polyethylene may be subject to creep under loading and, thus, the locking screw preload decreases with time, reducing the torque needed to loosen the locking screw.17 The major concern of disengagement of a modular object in knee arthroplasty is the development of metallic wear, fretting and corrosion that ultimately could lead to a severe inflammatory response causing arthrofibrosis or osteolysis with the potential need for early intervention.
This appears to be a concern with other implant designs as well. Shah et al.10 reported on a patient with loosening of the locking screw from the tibial insert in a Performance Knee (Biomet, Warsaw, IN) after four asymptomatic years. The loosened and dislodged screw and the polyethylene insert were exchanged. There was no extensive wear pattern or tibial or femoral component loosening. Sathappan et al.18 reported on a case in the Anatomic Modular Knee (AMK; Depuy, Warsaw, IN) with screw loosening of the screw locking mechanism in the tibial insert causing massive osteolysis requiring revision procedure. Both cases attributed micromotion between the two components to the disengagement of the locking mechanism.
In our patient, the LCCK was implanted for severe deformity as a primary total knee arthroplasty. It remained asymptomatic for nine years without signs of radiographic osteolysis. It suddenly became symptomatic once the locking screw migrated into the knee joint. The disengagement process was probably the cause for the severe metallosis in the knee synovial tissue over an extended period. In contrast to the case reports by Rapuri et al.,9 our patient did not experience a traumatic event that may have incited the disengagement. The evidence of backside wear of the tibial polyethylene supports the theory of micromotion at the backside of the insert translating into slow loosening of the screw-thread interface. Therefore, it is important to monitor for any signs of screw loosening to prevent premature wear of the tibial insert or osteolysis around the components on an annual basis.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}