
Residual Joint Laxity and Increased Cartilage Contact Deformation in ACL Reconstructed Knees
Ali Hosseini, PhD, Willem A. Kernkamp, MD, Nathan H. Varady, BSc, Guoan Li, PhD
This study was financially supported by the National Institutes of Health (R01 AR055612).
The authors report no conflict of interest related to this work.
©2017 by The Orthopaedic Journal at Harvard Medical School
 PDF
PDFOBJECTIVE The precise mechanisms contributing to postoperative degenerative cartilage changes in anterior cruciate ligament (ACL) reconstructed knees are not completely understood. This study further investigates the potential biomechanical aspects contributing to early degenerative changes.
METHODS Eight patients with a unilateral ACL reconstruction and intact contralateral knee were imaged using magnetic resonance and dual fluoroscopy imaging techniques during a quasi-static lunge. Knee kinematics and cartilage contact deformation were measured in both knees. The correlation between postoperative knee kinematics and cartilage contact deformation was studied.
RESULTS In the medial compartment at full extension, a moderate negative correlation was observed between cartilage deformation and anterior-posterior translation (R2 = 0.29, p=0.20), and a strong negative correlation was observed between deformation and internal-external rotation (R2 = 0.82, p=0.005). For the lateral compartment at full extension, a weak correlation for anterior-posterior translation was observed (R2 = 0.12, p=0.43). No correlation was seen in the medial or lateral compartment at 30° of flexion.
CONCLUSION Our results indicate that reductions in anterior translation and internal rotation after ACL reconstruction are correlated with increased cartilage deformations. Hence, improved knee joint kinematics may result in increased cartilage contact deformation, highlighting an important potential mechanism for the high incidence of degenerative changes in ACL-reconstructed knees.
KEYWORDS Anterior cruciate ligament, cartilage deformation, graft forces, osteoarthritis
The goal of anterior cruciate ligament (ACL) reconstruction is to restore knee stability, reduce the risk of secondary injuries, facilitate pre-injury activity level, and potentially prevent posttraumatic osteoarthritis (OA).1 Yet, the incidence of postoperative joint degenerative changes is 50-80%.1,2 Persistent postoperative knee laxity,3 inflammatory cytokines in the synovial fluid,4 occult cartilage abnormalities,5 and increased T1ρ/T2 signals of cartilage6-8 have been implicated in postoperative cartilage degeneration. However, the precise mechanisms contributing to these postoperative degenerative changes are not completely understood.
We have previously shown that ACL reconstruction was unable to fully restore normal knee kinematics in both cadaveric and in vivo experiments.3,10 We have also demonstrated that in vivo tibiofemoral cartilage contact deformations after clinically successful ACL reconstruction were higher than those measured in the intact contralateral knees at lower flexion angles.11 Multiple studies have indicated altered loading conditions within the knee are an important risk factor for OA development.12,13 Degenerative changes in response to altered joint loading after ACL transection have been well-demonstrated in longitudinal animal experiments.14 However, the relationship between postoperative knee kinematics and cartilage contact deformations after ACL reconstruction is not well defined.
We hypothesized that in ACL-reconstructed knees, decreased postoperative knee joint laxity is correlated with increased articular cartilage contact deformation. Therefore, we assessed the correlation between the changes in knee kinematics and corresponding changes in cartilage contact deformation in eight ACL-reconstructed knees.
This study is a re-analysis of our previous published studies of the tibiofemoral kinematics3 and tibiofemoral cartilage contact deformation in knees with a torn ACL and after ACL reconstruction.11 Our institutional review board approved both studies, and written consent was obtained from all participants prior to study participation. Eight patients with unilateral ACL rupture and intact contralateral knees participated in the studies (19-38 years old; 5 men, 3 women). The ACL rupture was confirmed on both clinical examination and MRI findings. All patients underwent arthroscopic surgical reconstruction of the ACL performed by the same orthopaedic surgeon as was described previously.3,11
The combined magnetic resonance (MR) and dual fluoroscopic imaging system (DFIS) technique has been described in detail previously.3,15 Briefly, both the ACL-injured and the intact contralateral knee were MR scanned with the patient supine, with the knee in a relaxed, extended position while sagittal and coronal plane images were acquired with a 3-Tesla MRI scanner. The MR images were then imported into solid modeling software to construct 3-dimensional (3D) surface mesh models of the tibia, femur, and articular cartilage.3
Next, both knees of the patients were imaged using the DFIS technique pre-operatively and six months postoperatively. Each patient performed a single-leg quasi-static lunge.11 The joint kinematics were regenerated using captured DFIS images and 3D MRI joint model. This technique has an accuracy of 0.1 mm and 0.3° in determining tibiofemoral joint translations and rotations, respectively.15
To measure the tibiofemoral joint kinematics, a coordinate system was created on both knees of each patient. The axes of both the tibia and femur and kinematic measurements have been described in detail previously.3
Cartilage thickness was calculated by finding the smallest Euclidian distance connecting a vertex of the articular mesh model to the cartilage-bone interface of the 3D models. The accuracy and repeatability of cartilage thickness measurement using MRI-based models of the knee joint has been validated to be 0.04 ± 0.01 mm.16 Cartilage contact deformation was then defined for each vertex of the articular surface mesh as the amount of cartilage surface intersection divided by the sum of the tibial and femoral cartilage thicknesses.16 The peak cartilage contact point was determined at each tested flexion angle in both medial and lateral condyles. Previous validation studies showed an accuracy of 4% when this technique was used to measure the cartilage contact deformation.17
Tibial anterior-posterior (AP) translation and internal-external (IE) rotation of six month postoperative knees were compared to those of intact contralateral knees. The changes (i.e., Δ = reconstructed – intact contralateral) were defined as ΔAP and ΔIE. Also changes in peak articular cartilage contact deformation were defined as ΔD. A paired Student’s t-test was used to detect significant differences between intact and reconstructed knees, with significance level set at p<0.05. The correlation between the changes in knee kinematics (ΔAP and ΔIE) with the changes in cartilage contact deformation of medial and lateral condyles (ΔD) were studied at full extension and 30° of knee flexion as the ACL primarily functions at lower flexion angles.
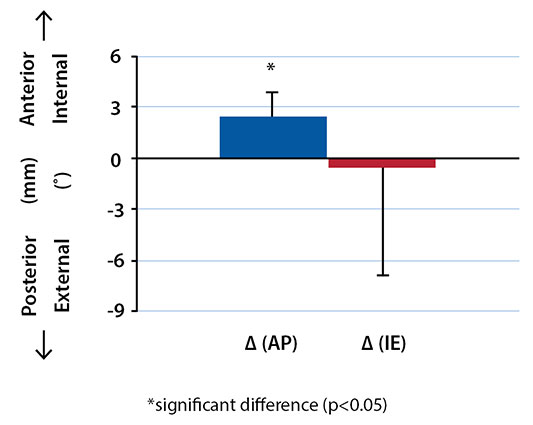
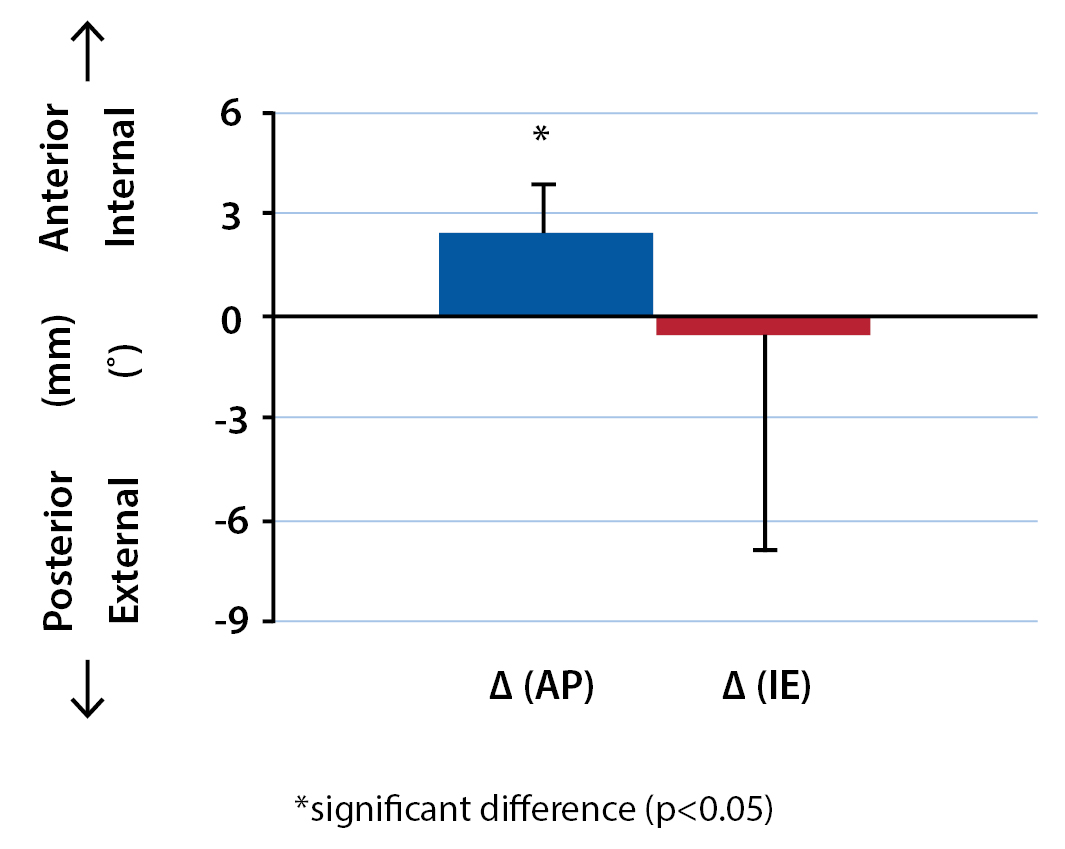
Changes in Kinematics
The change in tibiofemoral joint kinematics (i.e. reconstructed minus intact contralateral) is shown in Figure 1. At full extension, in the AP direction, a mean extra 2.5 mm anterior tibial translation was observed relative to the intact contralateral knees. No change was notable at 30° of knee flexion. Regarding IE rotation, the reconstructed knees had an extra external tibial rotation of 0.5° and 1.3° relative to intact knees at full extension and 30° of flexion, respectively.
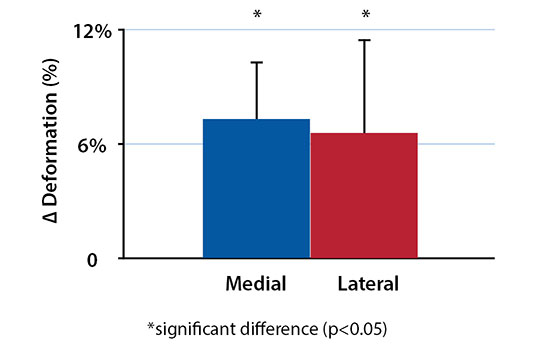
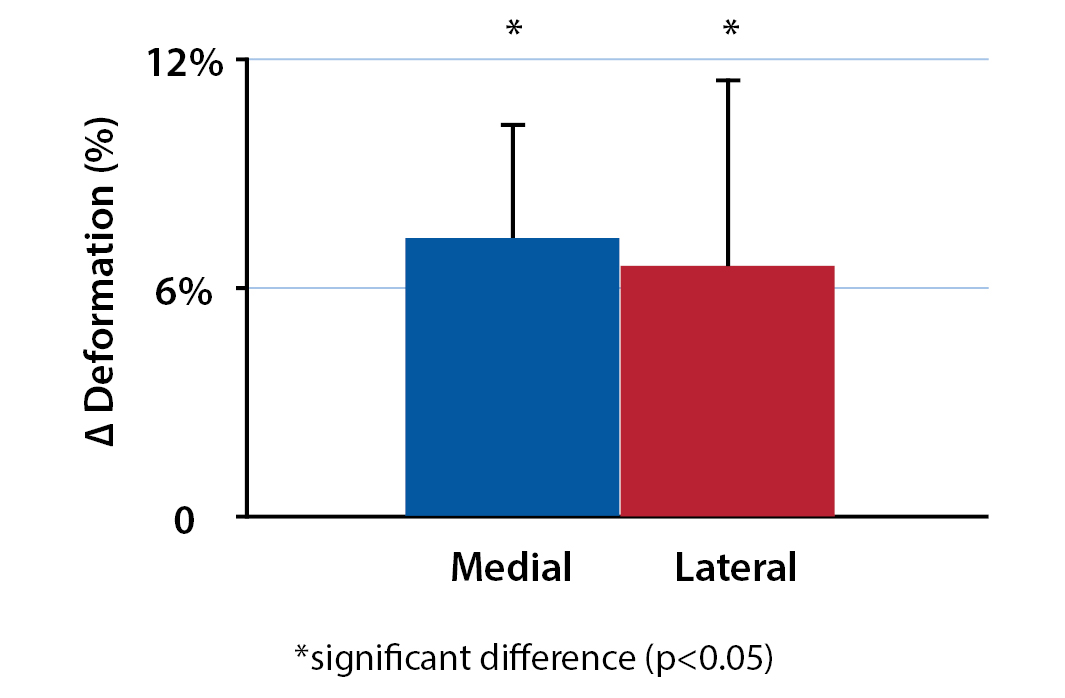
Changes in Contact Deformation
The changes in tibiofemoral cartilage contact deformation are shown in Figure 2. In the medial compartment, an increased cartilage deformation of 7.3% (p<0.001) and 1.6% (p>0.05) was measured in reconstructed knees at full extension and 30° of flexion, respectively. In the lateral compartment of reconstructed knees at full extension, an increased cartilage contact deformation of 6.6% (p=0.006) was observed. However, no significant changes in the cartilage deformation were found in the lateral compartment at 30° of flexion.
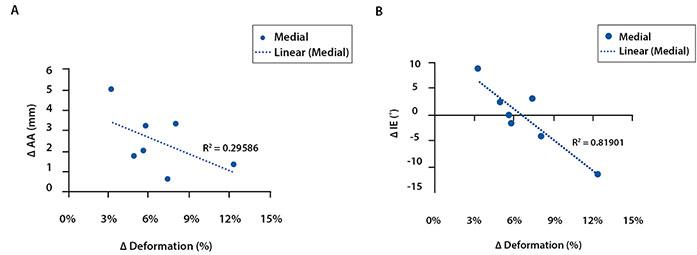
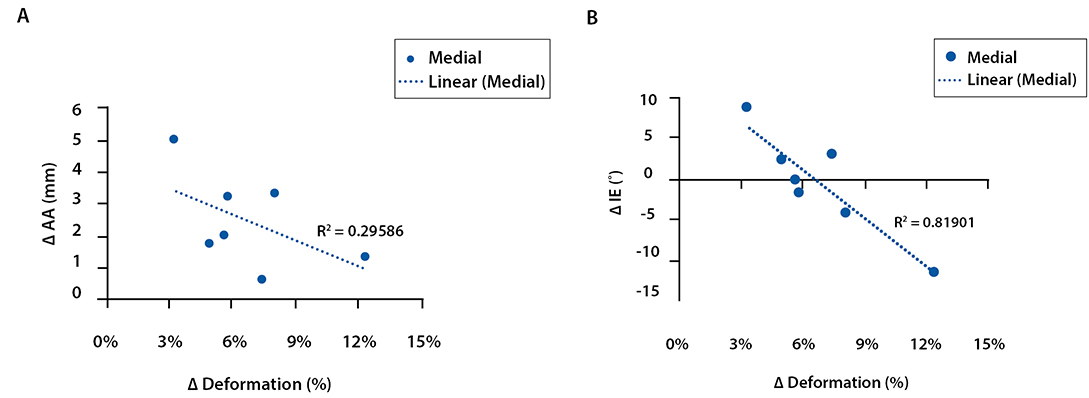
Correlation of Changes in Tibiofemoral Cartilage Contact Deformation with Changes in Tibiofemoral Kinematics
A moderate negative correlation was observed between ΔD and ΔAP in the medial compartment at knee full extension (R2 = 0.29, p=0.20 Fig. 3), and a weak correlation in the lateral compartment (R2 = 0.12, p=0.43). With regard to internal tibial rotations, a strong negative correlation was observed between ΔD and ΔIE in the medial compartment at knee full extension (R2 = 0.82, p=0.005 Figure 3). No correlation was observed in the lateral compartment at full extension, and no correlations were observed in either the medial or lateral compartment at 30° of flexion.
The most important finding of this pilot study was the existence of a moderate negative correlation between cartilage contact deformation and AP translation, and a strong negative correlation between cartilage contact deformation and IE rotation in the medial compartment at full extension of the knee. This data indicates that restoring knee kinematics (i.e., reducing laxity in AP translation and IE rotation) by means of ACL reconstruction may lead to increased cartilage deformation when compared to those of the intact knees.
Aberrant ACL graft forces may play a role in this correlation, as previous research has demonstrated an inability of ACL reconstruction to restore native ACL forces.9,18-23 For example, Li et al.18 found that in vitro ACL graft forces were greater at all flexion angles when compared to the intact ACL knee, and that higher ACL graft forces were required to reproduce native anterior tibial translation. Similarly, anatomic double bundle reconstruction is widely reported to better restore (or overcorrect) native knee kinematics24-26 but this techniques leads to significantly elevated graft forces.26,27 In the cadaveric study by Araujo et al.,19 three different ACL reconstruction techniques were tested; the anatomic single bundle ACL reconstruction had greater graft forces at full extension and an overconstrained knee in anterior tibial translation at this angle. The non-anatomic ACL reconstructions on the other hand showed lesser graft forces and greater knee laxity. Sim et al.9 showed that three different ACL reconstruction techniques achieved lesser graft forces when compared to the intact knee. In this study, the reconstructive techniques were unable to restore AP translations or IE rotations at lower flexion angles. A closer look at above described data suggests that reconstructions with greater graft forces may be able to better restore knee kinematics than reconstructions with lesser graft forces. Importantly, our study reveals that the elevated graft forces required to achieve better kinematics may be leading to increased cartilage contact deformation in ACL reconstructed knees when compared to the intact contralateral knee.
Previous studies have been unable to show substantial OA prevention related to ACL reconstruction when compared to non-surgically treated patients,28-30 with up to 50-80% of patients developing OA within 10 years after ACL reconstruction.1,2 The exact pathophysiology of cartilage degeneration remains unclear, but may be due to the altered postoperative mechanical and biochemical factors. It has been suggested that even minor, persistent abnormal kinematics after ACL reconstruction alter the cartilage contact locations to smaller areas of thinner cartilage with increased magnitudes of cartilage contact deformation.12,31,32 It is thought that this shift in loading of previously unloaded cartilage areas could lead to early degenerative changes.16,31-33 For example, Li et al.18 This may play an especially important role in the development of OA in unreconstructed knees. It has also been shown that an above-threshold dynamic compression of cartilage in the presence of inflammatory cytokines can induce and accelerate cartilage degradation.34 Hence, the increased cartilage contact deformation associated with better kinematics may play an important role in the high incidence of OA even in ACL-reconstructed knees. Specifically, the increased cartilage contact deformation in the ACL-reconstructed knee further supports the idea of mechanical overload playing an important role in the progressive development of OA.
Increased cartilage deformation may also lead to biochemical changes within the tissue. Analyzing the biochemical composition of cartilage using specific MR imaging biomarkers such as T1ρ and T2 has become increasingly popular for assessing early degenerative changes to cartilage indirectly.6-8 Zaid et al.35 recently correlated postoperative knee kinematics and cartilage T1ρ values one year after ACL reconstruction and found patients overloading previously unloaded areas were at higher risk of developing degenerative cartilage changes in the medial compartment of the knee. These findings demonstrate that mechanical deviations can result in observable biochemical changes in vivo. In future studies, the combined investigation of kinematics and cartilage deformation measurements with observable biochemical changes (e.g., T1ρ) represents a novel opportunity to help elucidate certain aspects of the complex interplay between mechanical and biochemical factors in the etiology of OA after ACL reconstruction.
There are a number of limitations to this study. In vivo ACL graft forces were not measured due to technical challenge. Only one functional activity, a single-legged, quasi-static lunge was studied. A trans-tibial ACL reconstruction technique was used. As the ACL is most active at low flexion angles, only full extension and 30° of knee flexion were studied. Future studies should assess the correlation between kinematics and cartilage deformation at additional flexion angles, with different reconstruction techniques, and under different motions and loading conditions. Additionally, a longitudinal, prospective study is warranted to investigate the time dependent knee joint kinematics, cartilage contact deformation and early cartilage biochemical composition changes of the knee after ACL reconstruction to investigate the biomechanical factors that could affect the postoperative cartilage degeneration.
In conclusion, this pilot study indicates that reduced anterior translation and internal rotation after ACL reconstruction is correlated with increased cartilage deformation. Therefore, the consequences of improved knee kinematics after ACL reconstruction might be related to the early degeneration of cartilage.






{kind=link}
{kind=link}
{kind=link}