
Extra-Articular Calcaneo-Tibial Schanz Pin Stabilization for Acute Ankle Trauma
Catherine Logan, MD, Lauren Ehrlichman, MD, Mohammad Ghorbanhoseini, MD, John Y. Kwon, MD
The authors report no conflict of interest related to this work.
©2017 by The Orthopaedic Journal at Harvard Medical School
 PDF
PDFOBJECTIVE Temporary stabilization of the ankle can be required for many reasons in the trauma setting. External fixation is typically required for injuries that require more rigid temporary stabilization. Several authors have previously reported on the use of trans-articular ankle pin stabilization for provisional immobilization of the ankle joint. While affording stability to the hindfoot, iatrogenic injury to the articular surfaces is a consequence of this technique. The purpose of this paper is to report on a cohort of patients who underwent temporary extra-articular calcaneo-tibial Schanz pin stabilization, a modified technique which does not violate the ankle or subtalar joints, for either temporary stabilization or as an adjunct to internal fixation following acute ankle trauma. Furthermore, we provide a commentary on the potential cost of this technique versus traditional external fixation.
METHODS A retrospective review was undertaken for all patients treated using extra-articular calcaneo-tibial Schanz pin stabilization by the senior author. Patients who sustained ankle trauma and required external fixation, whether for temporary stabilization, as definitive treatment, or as an adjunct to internal fixation, were identified. Patient demographics, diagnosis, treatment, duration of extra-articular ankle pin stabilization and any complications sustained from pin placement were documented.
RESULTS Nine patients underwent temporary extra-articular calcaneo-tibial Schanz stabilization for ankle trauma. Mean age was 64 years. Five patients underwent pin fixation for temporary stabilization prior to definitive fixation or for soft-tissue management. Three patients had this performed in combination with definitive fixation, and one patient had the pin alone used as definitive treatment. The average duration for which the pin was retained was 5.3 weeks. There were no pin-tract complications, no breakage of the pin and no neurovascular injuries, although one patient lost reduction.
CONCLUSION Extra-articular calcaneo-tibial Schanz pin fixation is in our opinion an easy and safe technique for temporary stabilization of the traumatized ankle. It should be considered in length-stable injuries when the ankle joint may be too unstable for splint or cast immobilization alone, yet traditional external fixation techniques may not be required or are not cost-effective.
LEVEL OF EVIDENCE Therapeutic Level IV, Case Series
KEYWORDS Extra-articular ankle pin fixation, ankle fracture, external fixator, ankle soft tissue injury, cost effective
Temporary stabilization of the ankle can be required for many reasons in the trauma setting. External fixation is typically required for injuries that require more rigid temporary stabilization than what can be achieved using a splint or other orthosis, especially if monitoring of the soft-tissue envelope is required.1-4 External fixation of the lower extremity is most commonly performed to stabilize ankle fracture/dislocations, pilon fractures, tibio-talar dislocations and/or to simply immobilize ankle motion in cases of severe soft-tissue trauma.5-7
Various external fixation methods have been used effectively and have been previously well-described in the literature, ranging from simple pin and bar constructs (i.e. “Delta” frame) to thin-wire circular ring fixators.5-7 While effective, multiple pins, bars, and wires are typically required which may in theory increase the likelihood of pin-tract infections.5-7 Furthermore, construct costs may be high. Logan, et al., recently demonstrated significant variability in cost of lower extremity external fixator constructs as placed by orthopaedic staff and trainees for damage control purposes.8 They concluded that once adequate construct stability is achieved then the use of additional components simply increases cost with no additional benefit to the patient.
Several authors have previously reported on the use of trans-articular ankle pin stabilization for provisional immobilization of the ankle joint.9-11 While these studies reported effectiveness of this technique, difficulties such as joint arthrosis, pin migration and inadequate fixation were also noted. League et al. demonstrated the effectiveness of extra-articular ankle pin stabilization as compared to trans-articular ankle pin stabilization in a cadaveric biomechanical model.12 To our knowledge, Thomas Roukis published the only report of clinical use in the orthopaedic literature of the extra-articular ankle stabilization technique when describing 9 cases used for ankle stabilization after posterior calf lengthening.13
The purpose of this paper is to report on a cohort of patients who underwent temporary extra-articular calcaneo-tibial Schanz pin stabilization, a modified technique which does not violate the ankle or subtalar joints, for either temporary stabilization or as an adjunct to internal fixation following acute ankle trauma. Furthermore, we provide a commentary on the potential cost of this technique versus traditional external fixation.
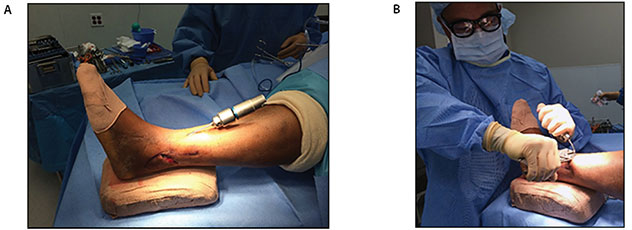
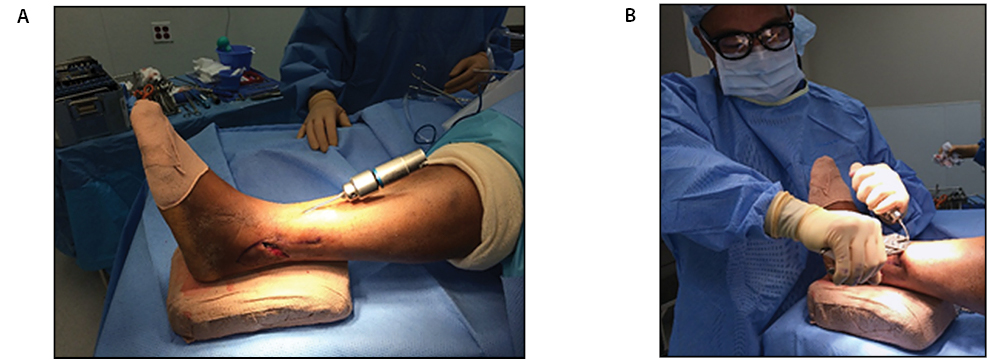
A retrospective review was undertaken for all patients treated using extra-articular calcaneo-tibial Schanz pin stabilization by the senior author. Patients who sustained ankle trauma and required external fixation, whether for temporary stabilization, as definitive treatment, or as an adjunct to internal fixation, were identified. Patient demographics, diagnosis, treatment, duration of extra-articular ankle pin stabilization and any complications sustained from pin placement were documented. Figure 1A, 1B, and 1C are illustrative of a representative patient.

Surgical Technique
In our technique, the patient is typically placed in the lateral decubitus position which facilitates pin placement due to ease of fluoroscopy. However, the pin can be placed with the patient supine or prone depending on the requirements of concomitant procedures. While multiple pins of varying diameter can be utilized, it is our preference to use a single 4 mm non-threaded Schanz pin placed from the calcaneal tuber in to the anterior tibial cortex which in our experience provides adequate rigidity when properly indicated. We prefer a non-threaded pin to facilitate removal.
The pin is placed mid-line into the postero-inferior calcaneal tuber. The pin is advanced slowly under fluoroscopic guidance at a trajectory that will penetrate the posterior tibial cortex while avoiding the subtalar and tibiotalar joints. The pin is then advanced through the medullary canal and engages the anterior tibial cortex for additional stabilization. Bi-cortical purchase may facilitate retrieval in the case of pin breakage. If preferred, the pin can also be placed anterograde from the anterior tibia into the calcaneus, which eliminates a plantar incision and external pin location.
The pin is bent prior to cutting so as to prevent migration into the bone. Bending of the heavy Schanz pin can be difficult given its diameter and relative short working length. A simple method if there are difficulties is to disengage the wire driver from the drill which may then be used as a lever arm. A plier is used to grasp the wire at the heel and is used as a counter torque (Figure 2 A,B). The wire is bent then cut in standard fashion using a bolt cutter.
Care must be taken to avoid iatrogenic penetration of the subtalar and tibiotalar joints. The pin should be centered midline or slightly lateral on the axial plane. A more medial starting point and/or medial trajectory when advancing the pin can endanger the tibial neurovascular structures.
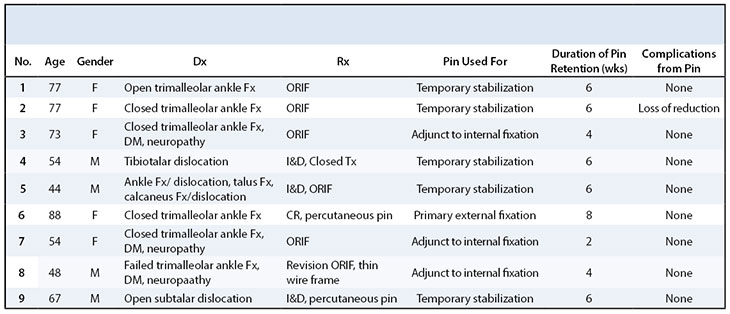
Nine patients underwent temporary extra-articular calcaneo-tibial Schanz pin stabilization for ankle trauma as demonstrated in Table 1. Mean age was 64 years. Five patients had pin fixation performed for temporary stabilization prior to definitive fixation, or for soft-tissue management. Three patients underwent pin fixation in combination to definitive fixation and one patient had the pin alone used as definitive treatment. The average length for which the extra-articular calcaneo-tibial Schanz pin stabilization was retained was 5.3 weeks. There were no pin-tract complications and no breakage of the pin. One patient lost reduction secondary to noncompliance with weight-bearing restrictions (Figure 3). Mean follow-up was approximately 7 months.

Temporary stabilization of the ankle can be required for many reasons in the trauma setting. Various external fixation methods have been used effectively for these purposes and have been previously well described in the literature.5-7 While some patients require the additional rigidity and flexibility in construct design afforded by traditional external fixation, others may require a less rigid construct for temporary stabilization or as an adjunct to internal fixation.
Construct costs for traditional external fixation for these purposes may be high with significant variability amongst surgeons. Logan, et al. recently demonstrated significant variability in cost of lower extremity external fixator constructs as placed by orthopaedic staff and trainees for damage control purposes.8 As part of a larger study, 20 orthopaedic staff and trainees were asked to place an external fixator on a full length lower extremity Sawbones model (Sawbones, Vashon Island, Washington) for a theoretical ankle fracture/dislocation in damage-control fashion. Each participant was provided a Synthes large external fixator set (Synthes, Inc, West Chester, PA) which is routinely utilized at all of the affiliated institutions in our prorgam, and an orthopaedic traumatologist assessed each construct for minimal adequacy of construct stability. The average whole sale cost of the external fixator constructs was $5622 +/- $1545. This can be compared to the whole sale cost of a 4 mm Schanz pin (Kmedic , Wayne, PA) utilized by the senior author which is $9.27 in this cohort of patients who did not require formal external fixation. While clearly cost-effective when indicated, it is important to recognize that cost of external fixation or Schanz pins may vary widely from institution to institution based on contract pricing and other variables.
Although we describe results from a small cohort of 9 patients, the above case series demonstrates the relative safety and effectiveness of this technique. While no comparative patient cohort using traditional external fixation was examined, we feel that extra-articular calcaneo-tibial Schanz pin stabilization for acute ankle trauma is a valuable technique for surgeons to consider when the ankle joint may be too unstable for splint or cast immobilization yet traditional external fixation techniques may not be required or are not cost-effective. However, to the best of our knowledge there are no biomechanical studies comparing extra-articular pin stabilization to traditional external fixation, and care must be taken. Patient non-compliance with weightbearing restrictions can, for example, result in loss of fixation. While higher energy injuries to the lower extremity resulting in severe soft tissue and/or bony injury likely require formal external fixation, the use of extra-articular ankle pin stabilization may be effective in cases where the injury is length stable, but the ankle or subtalar joints are unstable. We prefer this technique over trans-articular ankle pin fixation mainly due to:11
- the avoidance of iatrogenic injury to the tibio-talar and subtalar joint cartilage
- demonstrated equivalent construct stability
Potential complications include those inherent to any external fixation including pin tract infection, pin breakage, iatrogenic fracture at pin site, intra-articular penetration and injury to surrounding neurovascular structures.
Extra-articular calcaneo-tibial Schanz pin stabilization is in our opinion an easy and safe technique for temporary stabilization of the traumatized ankle and should be considered when the ankle joint may be too unstable for splint or cast immobilization alone yet traditional external fixation techniques may not be required or are not cost-effective. Future studies examining more patients undergoing this technique are required to further elucidate its efficacy and safety.






{kind=link}
{kind=link}
{kind=link}
{kind=link}