
A Systematic Review of Taping for Pain Management in Shoulder Impingement
Abhiram R. Bhashyam, MD, MPP, Catherine A. Logan, MD, MBA, MSPT, Sean M. Rider, MD, Brian Schurko, MD, CDR (ret) Matthew T. Provencher, MD
The authors report no conflict of interest related to this work.
©2018 by The Orthopaedic Journal at Harvard Medical School
 PDF
PDFBACKGROUND Despite research interest and popularity of use, the efficacy of shoulder tension taping in the management of shoulder impingement is unknown.
PURPOSE To review high-level evidence (randomized controlled trials [RCTs]) on the efficacy of tension taping for pain management and patient-reported function in patients with shoulder impingement.
DATA SOURCES Pubmed/MEDLINE, Embase, Cochrane, SPORTDiscus, and CINAHL databases
STUDY SELECTION Data sources were reviewed using a Boolean search strategy with keywords (“taping,” “kinesio-taping,” “kinesiotaping,” and “shoulder impingement”) for level 1 English-language studies between 1995 and 2015 that evaluated the efficacy of tension taping for shoulder impingement pain.
STUDY DESIGN Systematic Review
DATA EXTRACTION Included articles were critically appraised using the Physiotherapy Evidence Database (PEDro) scale for RCTs. Primary variables were Visual Analog Scale (VAS), Shoulder Pain and Disability Index (SPADI), and Disabilities of the Arm, Shoulder, and Hand (DASH) outcome scores.
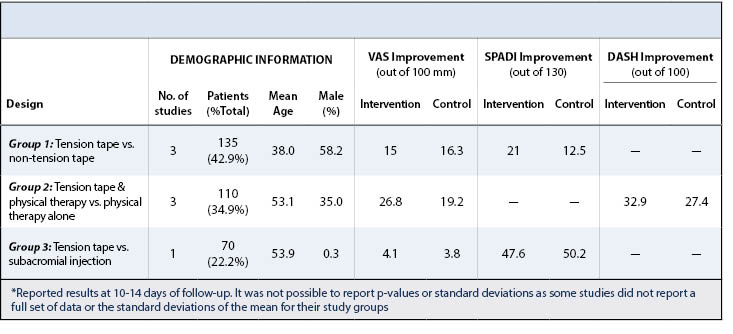
RESULTS Seven articles with 315 total patients (44.2% male, mean age: 48.0 years) were included with three types of randomized control trials. The types of trials included: (1) Evaluation of a standalone treatment (tension tape versus non-tension tape) (three studies with 135 patients (42.9% of total patients)), (2) Evaluation as an adjunctive modality (Tension tape with and without physical therapy) (three studies with 110 patients (34.9% of total patients)), and (3) Comparison versus injection (tension tape versus subacromial injection) (one study with 70 patients (22.2% of total patients)). Tension tape used in isolation was no better than non-tension tape or subacromial injection. Only Group 2 (tension tape with physical therapy) demonstrated up to 2 weeks (average VAS improvement of 26.8 versus 19.2 and average DASH improvement of 32.9 versus 27.4, in intervention versus control groups, respectively).
CONCLUSION This review of tension taping studies demonstrates that, for up to 2 weeks, taping for shoulder impingement may reduce pain and improve shoulder function scores when used as an adjunct to physical therapy.
LEVEL OF EVIDENCE I
KEYWORDSTaping, kinesiotape, shoulder impingement, subacromial impingement, rotator cuff tendonitis, external outlet impingement
Shoulder taping is widely used by physical therapists, athletic and personal trainers, and sports medicine physicians as an aid for prevention and treatment of shoulder pathology and dysfunction, particularly shoulder impingement.1 Primary impingement results from the rotator cuff impinging against the undersurface of the acromion, coracoacromial ligament, and the acromioclavicular joint, leading to pain and inflammation.2-5 The majority of shoulder impingement syndrome is primarily managed non-operatively with rest, activity modification, physical therapy, and/or injections. Rehabilitation focuses on restoration of glenohumeral kinematics and muscle activity patterns through multiple therapeutic techniques and modalities, including kinesiotaping.1-3
Kinesiotaping was initially described in the 1990s by Dr. Kenso Kase, with the theoretical purpose of supporting injured muscles and joints by lifting the skin and allowing improved blood and lymph flow.1 Kinesiotaping, also referred to as tension taping, is an elastic therapeutic tape that claims to stretch to 120-140% of its original length, then recoils to its initial length after application, exerting a pulling force to the skin. Proposed benefits include the facilitation of joint and muscle realignment, improved circulation, decreased pain and increased proprioception.6-8 Tape is typically applied in three-day intervals. Taping has been used as both an isolated treatment, and as an adjunct to traditional physical therapy to manage pain and increase function in various musculoskeletal injuries.9
The benefits of taping for shoulder impingement are unclear, and recent evidence regarding its efficacy has been conflicting, although taping remains wide-spread in clinical practice by patients, athletic trainers, physical therapists, and medical professionals.10 Five systematic or scoping reviews have been conducted on taping since 1995. Only one scoping review focused solely on shoulder conditions.10 Among the review articles, only five included papers considered taping for shoulder conditions. The purpose of this systematic review is to examine the current literature and develop better understanding of the efficacy of taping to reduce pain and affect patient-reported function in the setting of shoulder impingement.
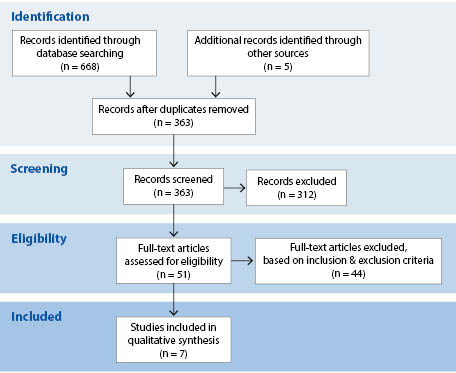
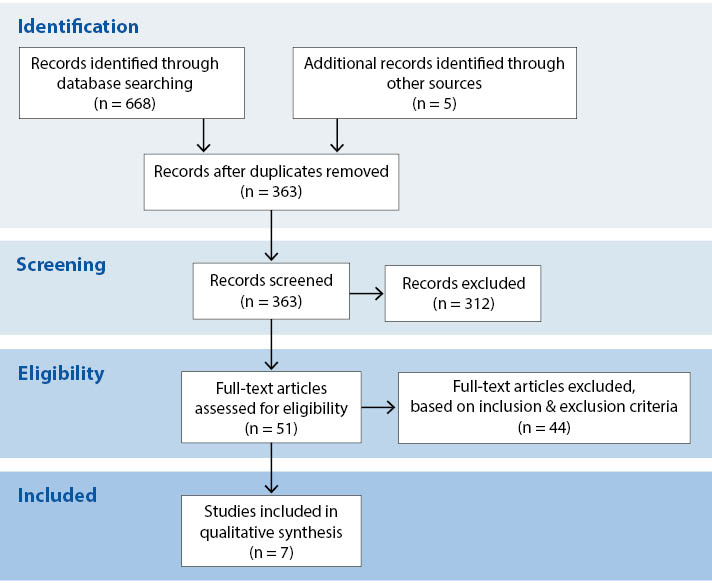
A systematic review method was used based on the framework outlined by Wright et al.11 A systematic literature search of PubMed/MEDLINE, Embase, CINAHL, SPORTDiscus and the Cochrane databases was performed, covering a time period from 1995 to 2015. Our combination search strategy employed the following keywords: (“kinesiotape” OR “kinesiotaping” OR “taping” OR “tape”) AND (“shoulder” OR “shoulders” OR “glenohumeral” OR “scapula” OR “rotator cuff” OR “subacromial”). This search identified a total of 363 unique articles, which was narrowed to 51 English-language articles after review of titles and abstracts germane to tension taping. This group of 51 full-text articles was then summarized using Preferred Reporting Items for Systematic Reviews ad Meta-Analyses (PRISMA, which is an evidence-based minimum set of items for reporting systemic reviews and meta-analysis) guidelines12 and reviewed using the following inclusion/exclusion criteria by two independent reviewers:
- Design Level I studies (randomized controlled trials)
- Participants All ages with confirmed recent diagnosis of shoulder impingement, subacromial impingement syndrome, external outlet impingement or rotator cuff tendonitis
- Intervention Non-surgical management of shoulder pain using elastic taping in isolation or as an adjunct to another non-surgical therapeutic modality
- Comparison No taping, sham (non-tension) taping, physical therapy or other non-operative intervention
- Outcome pain or function
- Exclusion criteria full-thickness rotator cuff tears, arthritis, shoulder instability, referred shoulder pain, calcific tendinitis
Seven studies met our criteria and were included in this systematic review. The study search and selection process are outlined using PRISMA guidelines in Figure 1.
Data Extraction and Summary
Selected articles were reviewed by two authors (ARB, CAL) and information was extracted and recorded using a customized form. The first author of this study initially reviewed all articles which were then reviewed by the remaining authors to ensure consensus and accuracy in reporting results. The following categories of information were extracted for each article based on recommended guidelines: objective, study design, study population, intervention group, control group, and outcome (including results, metrics, and statistics).11 Articles were grouped into three categories based on the control group used in the study design. A checklist method hierarchy to determine selection, performance, detection, and attrition bias was used for each article. Then a quality of evidence grading was referenced using the validated Physiotherapy Evidence Database (PEDro) database for randomized controlled trials (RCTs) and clinical practice guidelines for physical therapy (www.pedro.org.au). A systematic grading using the PEDro scale was performed for any RCTs that were not currently included in the database. A weighted mean (based on number of patients per paper) was used to report aggregate mean values for outcomes.13 It was not possible to report p-values as some studies did not report a full set of data or the standard deviations of the mean for their study groups.
Outcome Measures
The Visual Analog Scale (VAS) was used in the included studies to assess pain severity on a 0-100 mm scale. It is considered a valid and reproducible method of assessing pain, with clinically significant improvement defined as greater than 2 cm reduction, but it is prone to response bias.10 Similarly, the Shoulder Pain and Disability Index (SPADI, maximum score of 130) and Disability of Arm and Shoulder questionnaire (DASH, maximum score of 100) are self-administered questionnaires that consist of 2 dimensions: pain and functional activities. Both surveys are reliable and region-specific instruments.14,15
Demographic Information and Study Characteristics
Seven studies (315 total patients) were included in this systematic review (details regarding study selection can be found in the Methods and Figure 1). Studies were grouped into three randomized control trial study designs:
- Tension tape (intervention) vs. Non-tension tape (control group defined as taping applied without appropriate tension for therapeutic benefit)
- three studies with 135 patients; 42.9% of 315 total patients
- one study included physical therapy in both arms
- Tension tape and physical therapy vs. physical therapy alone
- three studies with 110 patients; 34.9% of total patients
- Tension tape vs. subacromial injection
- one study with 70 patients; 22.2% of total patients
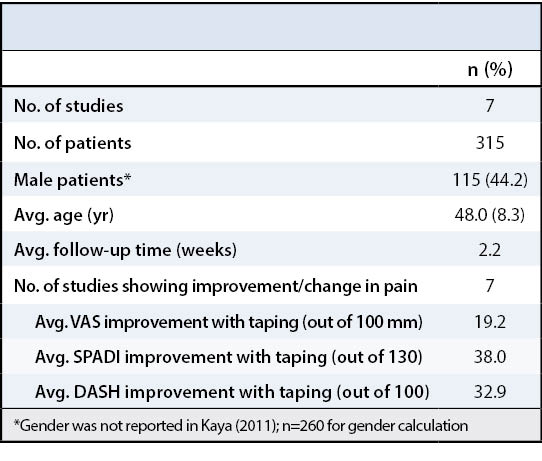
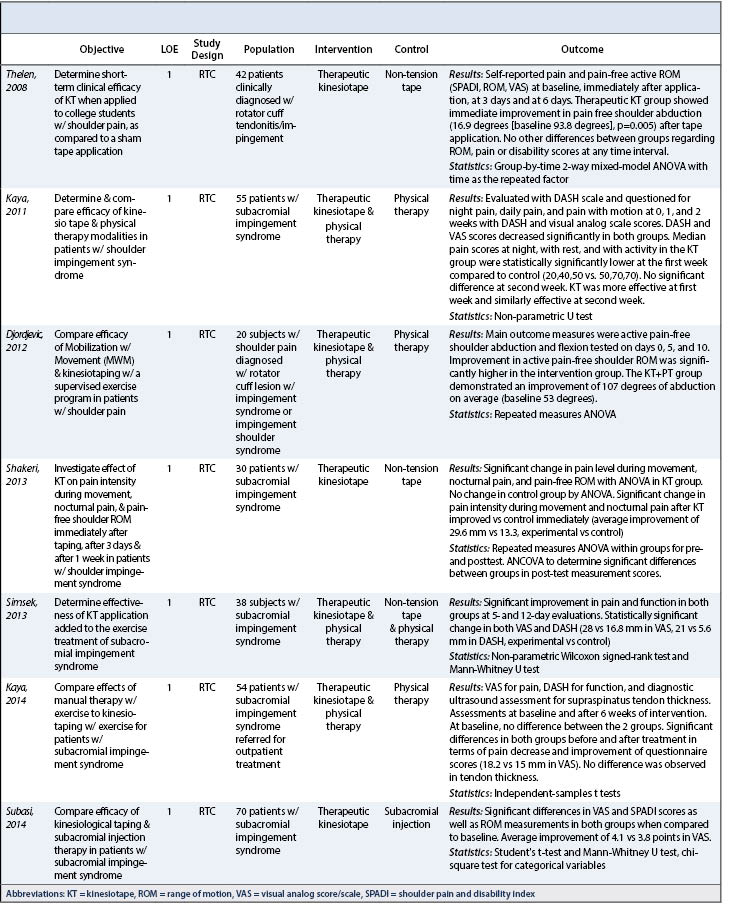
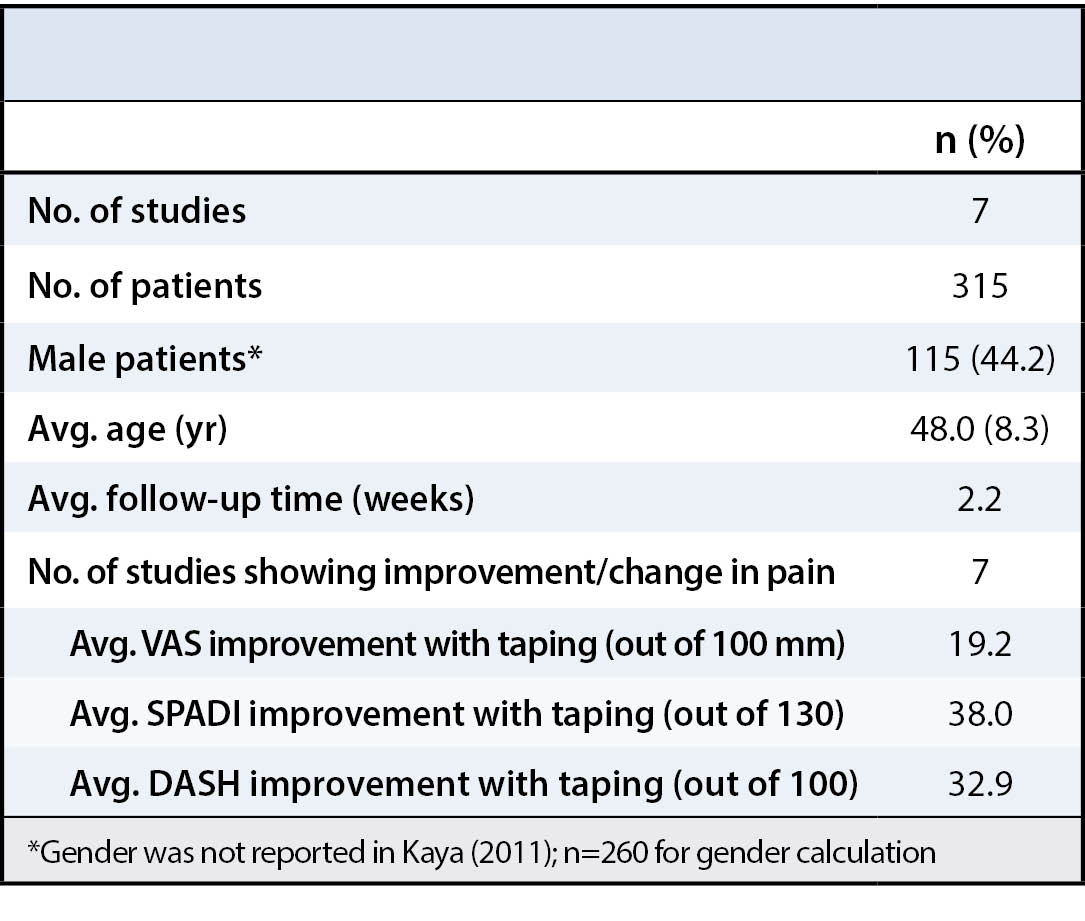
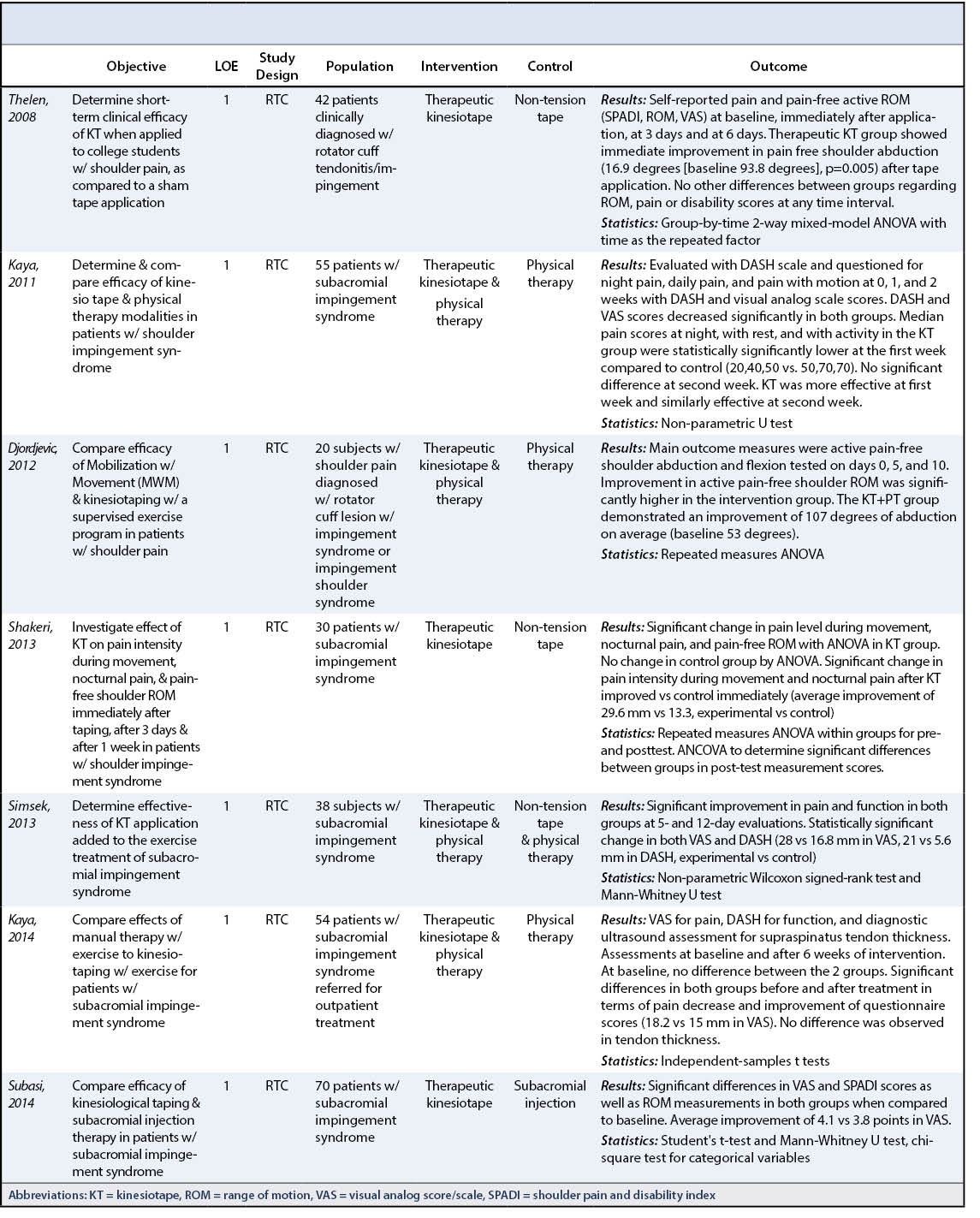
Average age of included patients was 48.0 ± 8.3 years and 44.2% were male. Taping strategy included tension tape with Kinesiotape® (Linden, UT) in all included studies. Average follow-up time was 2.2 weeks. Patient follow-up in the included studies ranged from immediate assessment after application of tape to 6 weeks post-application. Common intervals of assessment (post-application of tape) included 3 hours, 6 hours, 24 hours, 1 week, and 2 weeks. The most common duration of follow-up was 2 weeks. See Table 1 for a demographic summary of all studies included in this review. Narrative results of individual studies are summarized in Table 2.
Study quality
Study quality was assessed based on the PEDro scale. Ratings for all articles are provided in Appendix 1. Scores ranged from 5 to 9, with a median score of 7 and a mode of 9. A maximum score of 10 can be obtained through the PEDro scale, but due to the uniqueness of taping and the inability to blind the applying therapist, the achievable maximum score was 9.
Outcome measures
Pain was assessed using VAS in all 7 papers, SPADI in 3 papers, and the DASH in 2 papers. Seven studies showed improvement in shoulder pain. Among all studies, average VAS improvement with taping (out of 100 mm) was 19.2 mm, average SPADI improvement (out of 130) was 38.0, and average DASH improvement (out of 100) was 32.9.
Group 1: Tension tape vs. non-tension tape
Small improvement in pain scores up to 3 days were seen for all patients. Up to 7 days of pain improvement was seen for 21 of 36 intervention patients. Neither study reported clinically significant improvement in pain beyond 2 weeks.
Group 2: Tension tape and physical therapy vs. physical therapy alone
Up to 7 days of small improvement in pain was seen for all patients. No studies reported clinically significant improvement in pain beyond 2 weeks.
Group 3: Tension tape vs. subacromial injection
Treatment and control groups were similar after 1 week (3.8-4.1 mm improvement in VAS). Detailed study results are presented in Table 3.
The most important finding of this systematic review demonstrated that shoulder taping may be used as an adjunct to physical therapy for effective short-term pain modulation in shoulder impingement. After 7 days, however, all experimental taping groups are similar to control groups with no additional improvement in pain scores. Taping is widely used in clinical practice and thought to be a useful intervention for therapists in a wide range of conditions including subacromial impingement, anterior shoulder instability, and whiplash; however, recent systematic reviews have suggested that taping is largely ineffective.10,16,17 While those systematic reviews considered taping across multiple anatomic locations and injury types, a recent scoping review suggested that selective use of taping for upper extremity conditions may be useful after examining existing studies from all levels of evidence.10 We focused our systematic review on the use of taping for pain modulation in subacromial impingement. Our findings are consistent with other reviews conducted by Morris et al. and Taylor et al.,10,18 who concluded that taping may be an effective adjunct for pain management alongside physical therapy for a short duration of treatment. While these reviews explored the use of taping on a variety of conditions and locations, our review builds on their limited data for the short-term effectiveness of taping for the shoulder. Studies in this review that considered pain as an outcome found a reduction in shoulder pain after taping with immediate effect, that may last up to one week. However, this improvement was superior to the control group only when therapeutic taping was combined with physical therapy. The highest quality evidence from RCTs by Thelen et al. and Kaya et al. support this finding.19 In contrast, there is very little evidence to support the use of taping as a long-term strategy for pain control in patients with shoulder impingement as none of the seven studies using pain as an outcome measure found a clinically significant effect after two weeks. This finding is tempered by the fact that follow-up in almost all these studies was relatively short (maximum follow-up of six weeks).
Limitations
This systematic review was limited by a small number of articles included (n = 7); however, our study is the largest systematic review focused on the specific use of taping for pain management in shoulder impingement. Taping is still a relatively new technique and only a few high-quality studies based on its application to the shoulder have been conducted at present. While all of the studies included in this review focused on shoulder impingement, there was still significant heterogeneity with very few studies investigating precisely the same population or taping technique, making meta-analysis challenging. For example, we cannot definitively conclude that taping in isolation is less effective than taping combined with physical therapy, given that these two study designs used patients from significantly different age groups. In addition, it was not possible to perform statistical testing since some studies did not report standard deviations for their data. Hence, our results are subject to bias (direction unknown) given the variation in methodology of included papers.
A major limitation of all the articles included in the systematic review was short follow-up time frames and a total reliance on patient-reported data (e.g. VAS, SPADI, and DASH). Future studies should focus on longer term benefits of taping explicitly in order to better understand if taping has any long-term benefits. Future studies should also add outcome measures for pain that are not patient reported (e.g. analgesic use) since response bias is likely in all current studies on taping. Lastly, our review only included studies published in English which may mean that we missed relevant published research published in other languages.
This systematic review demonstrates that tension taping combined with physical therapy may reduce pain in recently diagnosed shoulder impingement versus physical therapy alone up to two weeks.






{kind=link}
{kind=link}
{kind=link}
{kind=link}