
Physician Self-Assessed Empathy Does Not Correlate with Patient Perceptions of Physician Empathy
Anne-Britt E. Dekker, MD, Mark Keulen, MD, Gregg Vagner, MD, Matt Driscoll, MD, Brannan Smoot, MD, Sean Gallagher, MD, Teun Teunis, MD PHD, Tom Crijns, MS, David Ring, MD PhD, Lee M. Reichel, MD
The authors report no conflict of interest related to this work.
©2019 by The Orthopaedic Journal at Harvard Medical School
 PDF
PDFBACKGROUND The medical field increasingly recognizes the value of empathic dialogue with patients. Possible gaps between clinician-based perceptions of clinician empathy, and patient perceptions of empathy, are areas for improvement of the patient-doctor relationship.
QUESTIONS / PURPOSES We tested the hypothesis that there is no correlation between physician self-assessed empathy (measured with the Jefferson Scale of Physician Empathy, JSPE) and mean patient rating of clinician empathy (measured with the Consultation and Relational Empathy, CARE). Secondarily, we hypothesized that there is no correlation between the doctor’s emotional quotient (measured with the Assessing Emotions Scale, AES) and mean patient perceived empathy (CARE). Additionally, we explored factors that were independently associated with higher patient perceived empathy.
METHODS This cross-sectional multi-center study included 121 new patients seeking care at one of six orthopedic surgeon offices. Measures that were collected included CARE, AES and JSPE. We sought factors associated with the CARE measure, accounting for age, sex, surgeon age, AES and JSPE score.
RESULTS There was no association between physician self-assessed (JSPE) and mean patient rated clinician empathy using the CARE measure (β -0.018, 95% CI -0.49 to 0.45, SE 0.24, P=0.94), and no correlation between doctor emotional quotient (AES) and mean perceived empathy (CARE).
CONCLUSION We found no association between the measured surgeon self-assessed empathy or graded emotional quotient and mean patient perceived empathy. Further research should address the extent to which these findings reflect limited surgeon self-awareness of their effectiveness of empathic communication or patient factors that account for lower perceived empathy.
LEVEL OF EVIDENCE Level II Prognostic Study
KEYWORDSPerceived Empathy, Effective Communication, JSPE, CARE, AES
Effective communication strategies conveying empathy and compassion increase patient satisfaction, improve treatment adherence, decrease malpractice claims1 and improve physician diagnostic accuracy.2,3 Conversely, a deficit in empathy is associated with physician burnout and exhaustion.4-6 Although there is no agreement on what comprises effective empathy, there is general agreement on its definition: “the ability to understand and share the feelings of a patient”.4,7 Previous studies among medical students found that higher self-reported empathy measured with the Jefferson Scale of Physician Empathy (JSPE, student version) was associated with clinical competence measured by their ratings for clinical clerkships.8,9
Effective communication includes awareness of one’s opportunities for improved mutual respect, listening, and shared discussion.10 These communication strategies could be linked to enhanced patient perceived empathy. A recent study of 90 patients treated by 36 residents found a moderate correlation between the physician self-perception of empathy (JSPE) and the Jefferson Scale of Patient Perceived Empathy (JSPPE) (r = 0.48, p < 0.05).11 In addition, another study showed no correlation between internal medicine residents self-rated and their patient-rated empathy.2
A better understanding of the gap between physician self-assessment and patient perception of empathy might identify opportunities for improvement in the patient-clinician interaction. We tested the correlation between physician self-assessed (JSPE) and patient perceived empathy (CARE, Consultation and Relational Empathy) among orthopedic surgeons, hypothesizing that there is a correlation between JSPE and CARE measures. Second, we hypothesized that there is a correlation between the doctor’s emotional quotient (measured with the Assessing Emotions Scale, AES) and CARE. Third, we sought factors that were independently associated with a higher patient perceived empathy.
This cross-sectional multi-center cohort study was approved by our Institutional Review Board. Verbal informed consent was obtained from all eligible patients that agreed to participate in the study.
Study Design
This cohort included new, English-literate patients aged 18 to 89 years, with health insurance and employed across a wide variety of industries, seeking care for a musculoskeletal problem at the ambulatory offices of one of the six participating orthopedic surgeons between December 2016 and June 2017. After the visit with the orthopedic surgeon, a research assistant not involved in patient care provided a tablet computer with predesigned questionnaires.
Patient questionnaires included basic demographics, surgeon name and office location, and CARE measure.19 This measure consists of ten items, each on a 5-point Likert scale ranging from 1 (poor) to 5 (excellent), asking questions such as:
- “How was the doctor at: (1) Making you feel at ease? (2) Letting you tell your story? (3) Really listening?”
The summed score of all items ranges from 10 to 50 points, with higher scores indicating greater empathy. When one or two ‘does not apply’ responses were given, the mean average for the other scored questions was used. We excluded one patient that gave more than two ‘does not apply’ responses on the CARE Measure, making it invalid according to the instructions for how to score the instrument.
Six surgeons completed questionnaires recording demographics including years in practice, AES,21 and JSPE.15 Surgeons with different subspecialties were included:
- Upper Extremity
- Lower Extremity
- Arthroplasty
The Assessing Emotions Scale consists of 33 items on a 5-point Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree), such as:
- “I know when to speak about personal problems with others”
- “I expect that I will do well on most things I try"
- “I find it hard to understand the nonverbal messages of others"
Scores range from 33 to 165. The JSPE is a 20-item scale that is measured on a 7-point Likert scale ranging from 1 (strongly disagree) to 7 (strongly agree), such as:
- “My doctor understands my emotions, feelings and concerns"
- “My doctors asks about my daily life"
Scores range from 20-140.
Statistical Analysis
An a priori power calculation determined that a sample size of 82 patients was needed to answer our primary study question with 80% statistical power (with α = 0.05) to detect a medium effect size (0.30) correlation between patient-perceived empathy and physician rated empathy. We decided to increase the sample in order to include more surgeons to make the results more generally applicable. Continuous variables are described as mean and standard deviation, and discrete variables are described as proportions.
No bivariate analyses were performed because we intended to include all measured variables in the final model (enter method). We hypothesized there was a correlation between CARE and JSPE measures as well as CARE and AES. However, for study purposes, we tested the null hypothesis that there was no correlation between measures. We created a multivariable linear regression to determine factors associated with patient perceived empathy on the level of the surgeon. Age and work experience of the surgeon (in years) were found to be collinear, so we omitted surgeon experience from the multilevel linear regression analysis. Results were reported as regression coefficients (β) with 95% confidence intervals (CI). A two-tailed p-value of < 0.05 was considered statistically significant.
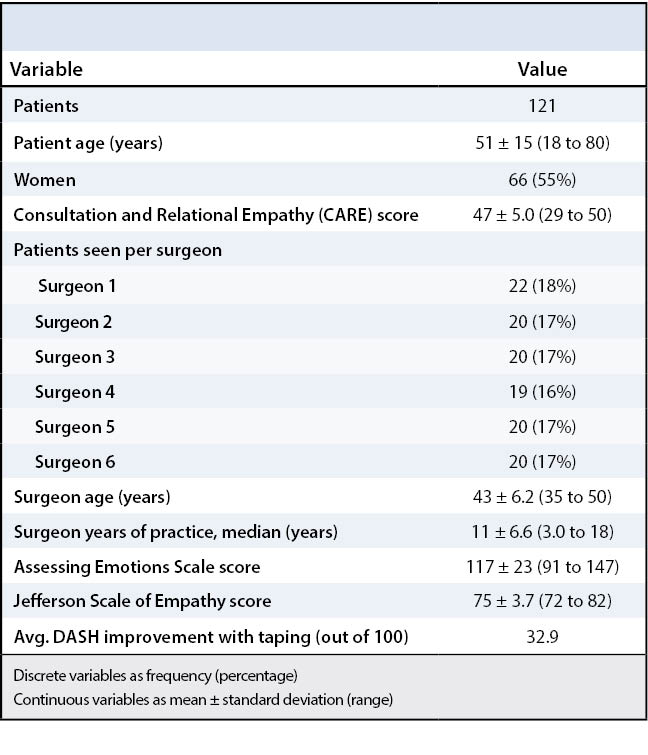
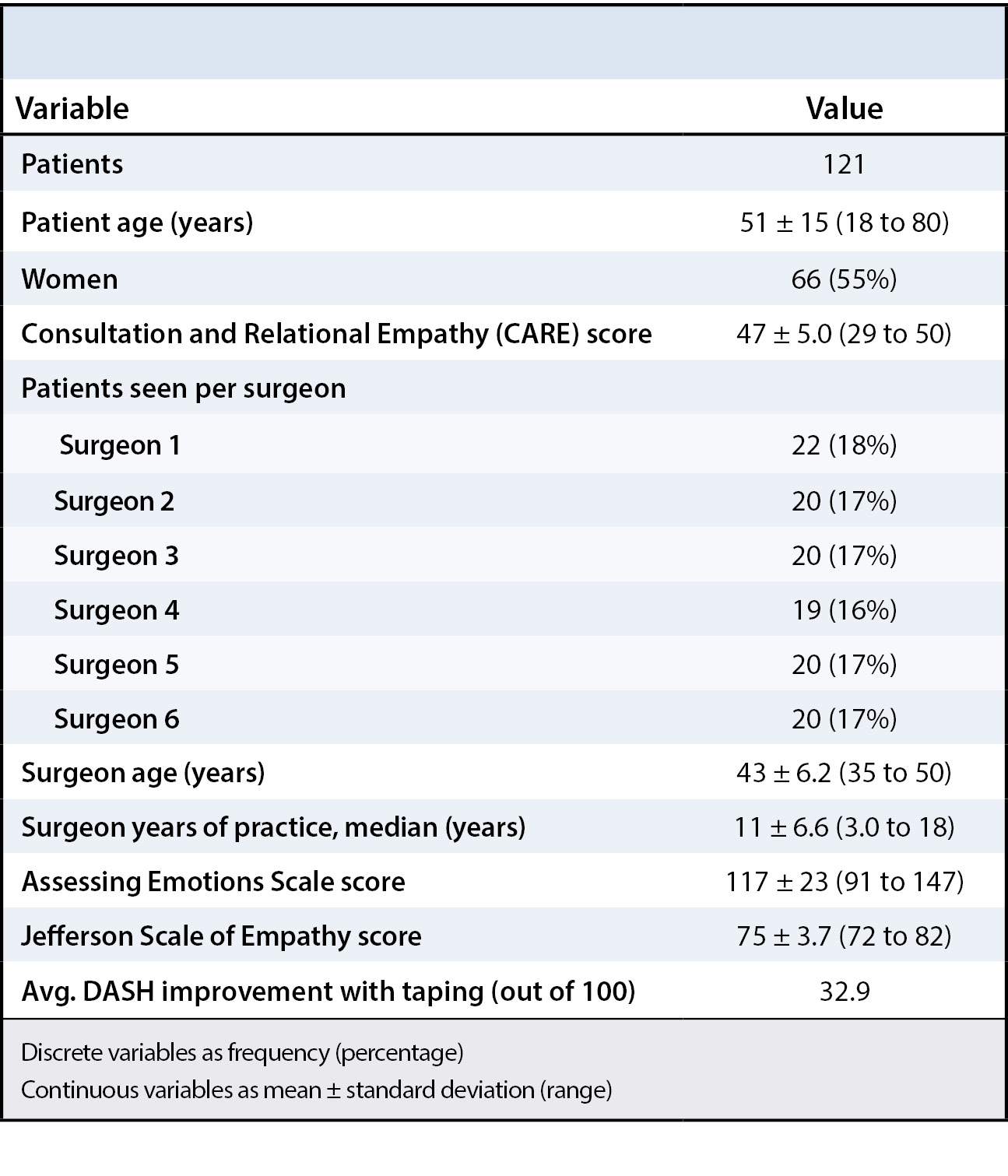
The 121 patients composing our cohort included 55 (45%) men and 66 (55%) women with an mean age of 51 years (SD 15). The six participating surgeons had a mean age of 43 years (SD 6.2) and on average were in practice for 11 years (SD 6.6) (Table 1). The mean CARE score among 121 patients was 47 (SD 5.0, range 29 to 50). The mean AES score was 117 (SD 23, mean 91 to 147), and the mean JSPE score was 75 (SD 3.7, range 72 to 82).
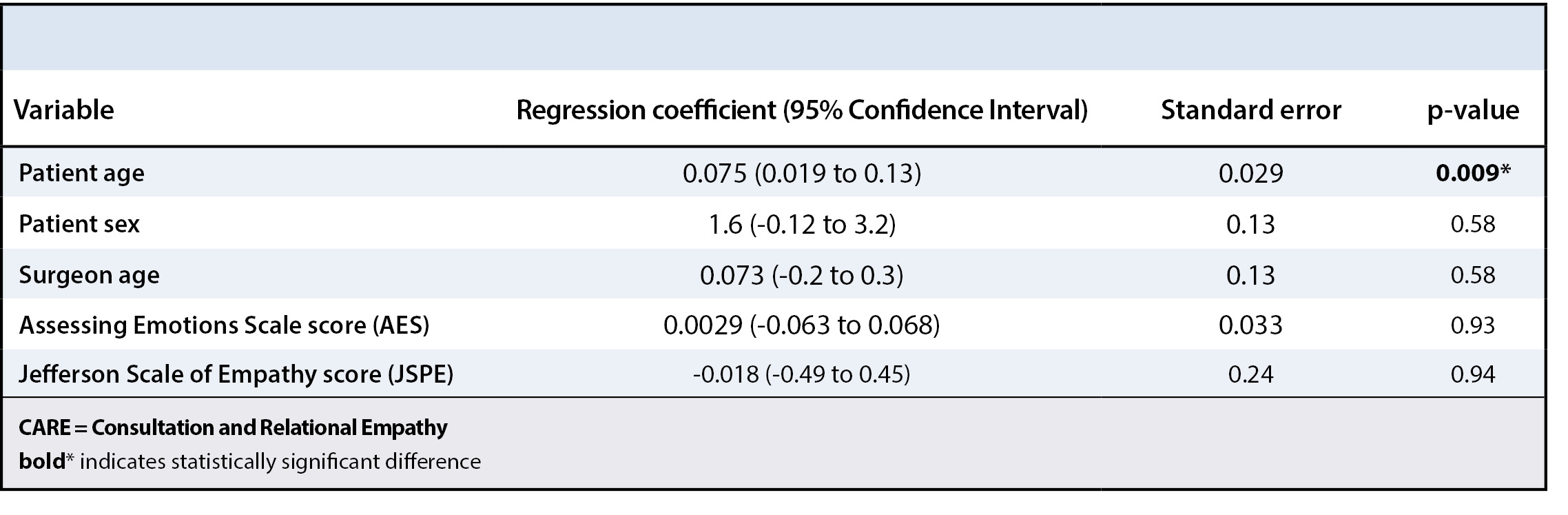
The multilevel linear regression model on the level of the surgeon demonstrated that there was no association between the physician self-assessed empathy (JSPE) and mean patient rated empathy using the Consultation and Relational Empathy (CARE) measure (β regression coefficient [β] -0.018, [95% CI -0.49 to 0.45], standard error 0.24, p = 0.94) (Table 2).
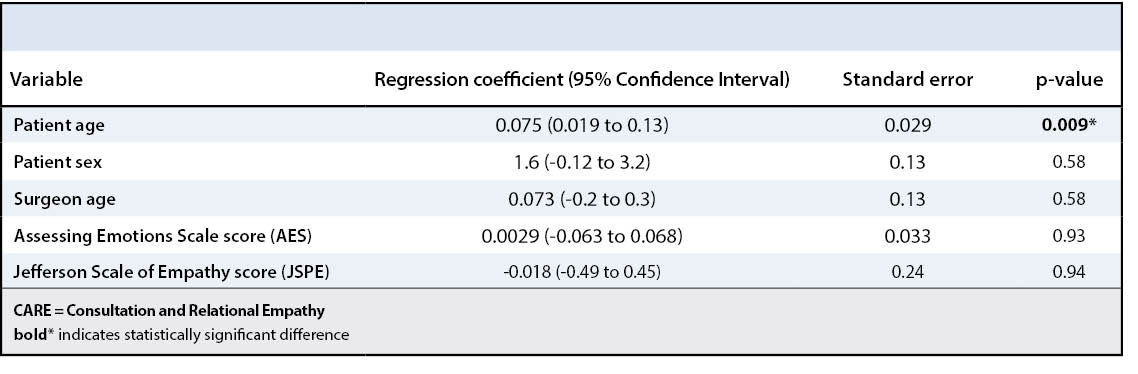
There was no correlation between doctor’s emotional quotient (AES) and mean perceived empathy (β 0.003, 95% CI -0.063 to 0.068, standard error 0.033, p = 0.93).
Greater patient age was independently associated with higher perceived empathy (β 0.075, 95% CI 0.019 to 0.13, standard error 0.029, p = 0.009). Patient gender, surgeon age, the AES score and JSPE score were not independently associated with perceived surgeon empathy.
The medical field increasingly recognizes the value of empathic dialogue with patients. It improves patient satisfaction, treatment adherence, and clinical outcomes with fewer complications.14,15 Physician benefits include fewer malpractice claims, better diagnostic accuracy, less stress, and less burnout.16,17 If there is a gap between a clinician’s self-perception about empathy and the patient’s perception of their empathy, that might suggest important opportunities for improving patient-clinician relationships. In the current study, the orthopedic surgeon self-assessed empathy (JSPE) and mean patient rated empathy (CARE) were unrelated. Additionally, surgeon emotional quotient (AES) and patient perceived empathy (CARE) were unrelated.
This study has several limitations. As this study was conducted among six orthopedic surgeons at four outpatient clinics in a large, relatively affluent city, our results may have limited generalizability to other regions, populations, and treatment settings. Another limitation is that we did not account for differences in diagnosis, medical background, or socioeconomic level. Although this might further decrease the generalizability of our study results, we believe that our sample is representative of employed patients with health insurance that normally present at an outpatient orthopedic surgery office. Further, the surgeons were aware of the existence of this study, which may have caused them to subconsciously alter their empathic behavior. Also, test results might have been influenced by patients not wanting to negatively rate their physician after just having had a clinic visit with them. Finally, the existence of the “ceiling effect,” which is often inherent to the use of empathy measures, and the limited variation in surgeon self-assessed empathy scores, may have affected the analysis.
We found no correlation between CARE and JSPE. Consistent with our findings, a study of internal medicine residents and their patients found no correlation between resident self-rated and patient-rated empathy (r = 0.24, p = 0.223).2 Conversely, according to a study of 90 patients treated by residents, one-quarter of the variation in self-reported physician empathy scores was accounted for by variation in patient perceived physician empathy.11 One interpretation of our findings is a strong ceiling effect: most patients scored the CARE measure at or near its limit for maximum empathy. Such a limited spread in the measure of perceived empathy may affect the statistical analysis. To advance the study of clinician-patient relationships, we need a measure of empathy that creates a better distribution of scores. Currently to our knowledge, no empathy measure without this ceiling effect exists. Our research group is currently developing new satisfaction and empathy measures with less of a ceiling effect and less censoring. While patients perceived their physician’s empathy as near perfect, the surgeons scored relatively low on the JSPE. In addition, the average JSPE score of participating surgeons was notably lower compared to other studies (75 versus 110, respectively).6,7,18-20 Given that orthopedic surgeon communication effectiveness scores such as CG-CAHPS (the Clinician and Group Consumer Assessment of Healthcare Providers and Systems) are the lowest nationally of any medical specialty, this may represent a measure of self-awareness.21 But, on average, there was no correlation with perceived empathy. We have a sense that there may be a limited correspondence of perceived empathy and effective communication strategies, and we plan to study this hypothesis using videotaped visits and ratings of effective communication.
Secondarily, we hypothesized that there is no correlation between AES and CARE. The AES is an emotional intelligence scale consisting of appraisal of emotion in the self and others, regulation of emotion in the self and others, and utilization of emotion in solving problems. The participating surgeons scored relatively low on the AES measure, compared to 39 samples of various groups in a general population.13 Due to the nature of their work, surgeons are possibly more distant and emotionally detached, which might be the reason for the low AES score. In addition, studies show that the degree of empathy shown by medical students decline during their education.22-24 Both factors may contribute to a lower AES.
Thirdly, we were interested in the factors that were independently associated with perceived physician empathy. Specific physician characteristics potentially linked to perceived empathy in prior studies include physician age, sex and years in clinical practice.4,6,13,21
In our study, only greater patient age was significantly associated with greater perceived empathy. A possible explanation for this finding is that older patients tend to have more respect for the physician, and therefore give a higher perceived empathy score. Alternatively, physicians might have more compassion for the elderly and the effect of musculoskeletal problems on their quality of life. Physician gender6,7,19,21 and years in clinical practice25,26 did not correlate with perceived empathy or satisfaction in prior studies. One study found that consultation length was significantly associated with perceived empathy (β = 0.19, p < 0.001).18 However, another study showed that the perceived level of physician empathy and not the duration of the visit was the most important factor in patient satisfaction.25
There is no association between surgeon self-assessed empathy or graded emotional quotient and perceived empathy. There may be other factors that contribute to perceived empathy that have not been fully elucidated. Further research should address factors associated with perceived clinician empathy. In addition, it may be worthwhile to study interventions to improve communication effectiveness and surgeon self-assessed empathy to determine if such interventions improve perceived clinician empathy.
AD would like to acknowledge the grants received from Koninklijke Nederlandse Akademie van de Wetenschappen (KNAW), Michael Fonds and Leids Universitair Fonds.







{kind=link}
{kind=link}