
Retrograde Humeral Nail for treatment of an isolated femoral shaft fracture in a patient with Mucolipidosis Type IV: Surgical decision making and outcome
Ishaq O. Ibrahim, MD and Edward K. Rodriguez, MD, PhD
The authors report no conflict of interest related to this work.
©2020 by The Orthopaedic Journal at Harvard Medical School
 PDF
PDFCASE A 33-year-old woman with Mucolipidosis Type IV, a rare lysosomal-storage disease with phenotypic similarity to cerebral palsy, was transferred to our level-1 trauma center for treatment of an isolated femoral shaft fracture. Bony abnormalities associated with the patient’s underlying syndrome added significant complexity to the management of an otherwise common injury pattern. Successful care of her femur fracture was ultimately achieved with a retrograde humeral nail.
CONCLUSION A retrograde humeral nail may be considered a viable treatment option in the care of lower extremity long bone fractures in patients with small stature or circumstances where resources are limited.
LEVEL OF EVIDENCE Level IV Case Report
KEYWORDS Mucolipodosis, femur fracture, intramedullary nailing, retrograde humeral nail, displasia
In-born errors of metabolism (IEMs) comprise a large class of genetic disorders characterized by isolated gene defects that lead to breakdowns in essential metabolic pathways. In-born errors of metabolism may have a number of orthopedic manifestations including bony dysplasia, joint contractures, and scoliosis.1,2 Femoral shaft fractures occurring in such patients may present a unique challenge to orthopedic surgeons. Closed treatment may impede patient care, and may increase risk for nonunion or malunion.3-5 Similarly, abnormal bony geometry may preclude use of traditional fixation devices, and poor bone quality may increase risk for iatrogenic fracture and implant failure. Importantly, any intervention must consider the patient’s global function and specific goals of care.
We describe the unique case of an isolated femoral shaft fracture occurring in a patient with Mucolipidosis type IV, a rare lysosomal storage disease characterized by static encephalopathy, psychomotor retardation, and small stature.6 The orthopedic manifestations of Mucolipidosis type IV are not well described, but mirror those of cerebral palsy for which the condition is commonly mistaken.6-8 We describe the novel treatment of our patient’s femur fracture with a retrograde humeral nail. The patient’s guardian was informed that the details of this case would be submitted for publication and provided consent.
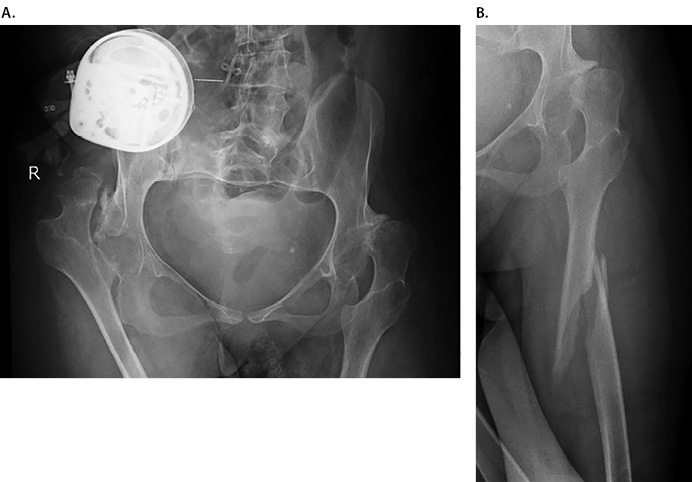
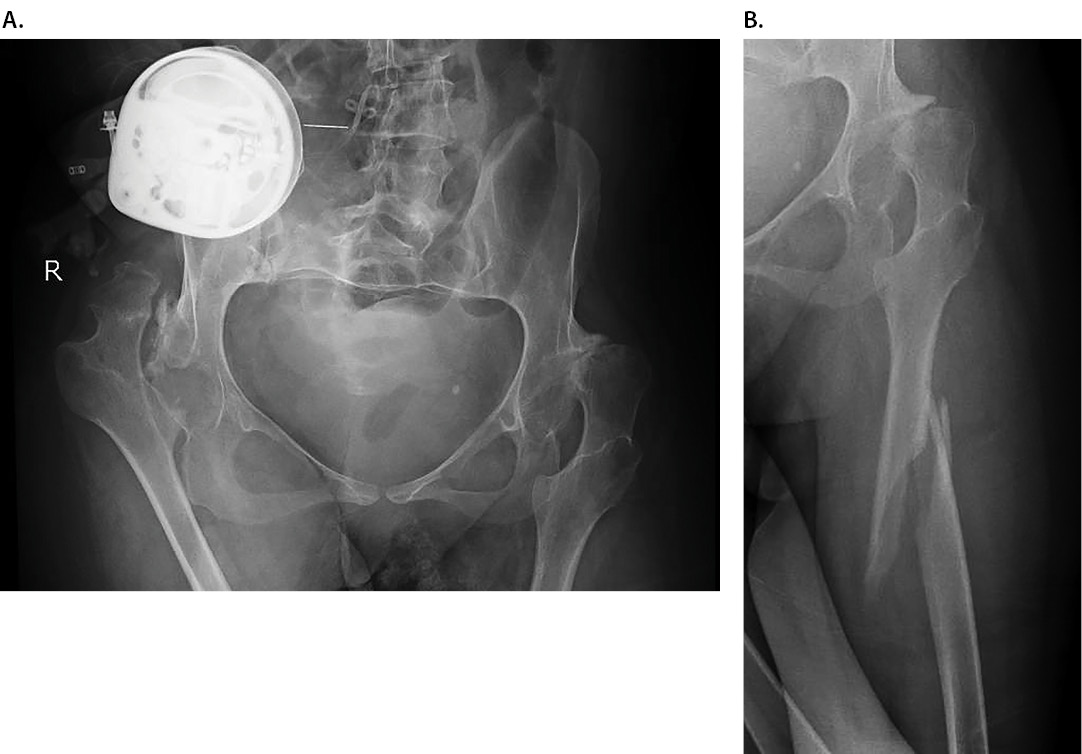
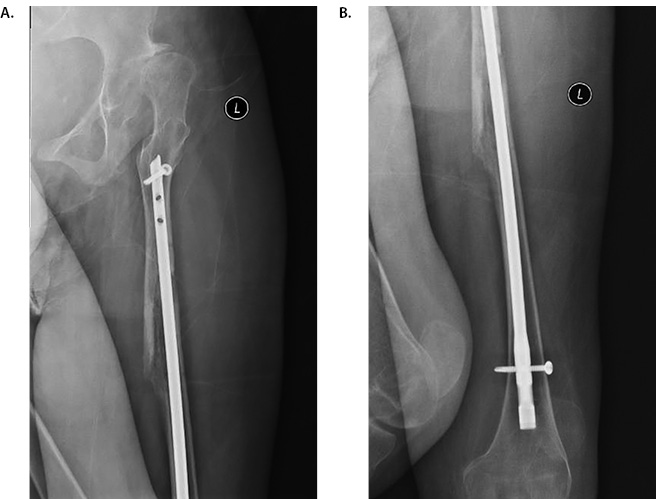
A 33-year-old non-verbal and non-ambulatory female with history of Mucolipidosis type IV was transferred to our Level-1 trauma center for treatment of an isolated left femoral shaft fracture. She was dependent in all activities of daily living requiring full assist for bed-to-chair transfers, the context in which her injury had occurred. She received continuous feeds via percutaneous gastrostomy tube and was treated for spasticity with an intrathecal implanted baclofen pump. Physical examination was notable for small stature, global developmental delay, and spastic quadriplegia. She had elbow and wrist flexion contractures and her bilateral lower extremities were internally rotated with hip flexion and adduction contractures. Injury films revealed an oblique, subtrochanteric femur fracture with mild shortening and valgus angulation (Figure 1A). The femur itself was dysplastic, with a narrow medullary canal and significant coxa valga (Figure 1B). Pelvic radiographs revealed diffuse osteopenia, acetabular dysplasia, and mild thoracolumbar scoliosis. There was severe subluxation of the left hip and complete dislocation of the right hip.
To facilitate patient care, including hygiene and transfers, operative fixation was favored. Several technical concerns were taken into consideration during preoperative planning. Intramedullary fixation was favored over plate osteosynthesis to minimize surgical dissection and risk for infection given the patient’s non-ambulatory status. Her narrow medullary canal, however, was unlikely to accommodate a standard femoral nail and special order pediatric nails were not immediately available at our institution. Smaller diameter humeral nails have been previously described for treatment of femoral shaft fractures in adolescents and other patients of small stature.9,10 In each case, however, the nails were inserted in an antegrade fashion via a trochanteric entry point. In our case, the extreme valgus of the patient’s femoral neck made cephalomedullary nailing unfeasible. As such, the decision was made to attempt intramedullary fixation via a retrograde approach.
The patient was placed supine on a radiolucent operating table. The left lower extremity was prepped and draped in the normal sterile fashion. The distal femoral starting point was accessed via a standard infrapatellar approach. The intercondylar notch was identified and the starting guidewire was placed just anterior to Blumensat’s line. Extreme care was utilized during over-reaming of the distal femoral cortex and subsequent passage of the ball-tipped guide-wire. Cannulation of the proximal fracture fragment was very challenging and ultimately required direct reduction of the fracture via a small lateral incision (Figure 2). The canal was not reamed given the patient’s thin cortices. A 7 x 310-millimeter Titanium Cannulated Expert Nail (Synthes, West Chester, Pennsylvania, USA) was subsequently passed over the guidewire. The 5-degree proximal bend in the nail was manually straightened to permit passage through the femoral canal. The nail was subsequently locked proximally with a single bolt and distally in a similar fashion to maintain rotational alignment. The patient was discharged back to her assisted facility on post-operative day three following an uneventful hospital stay.

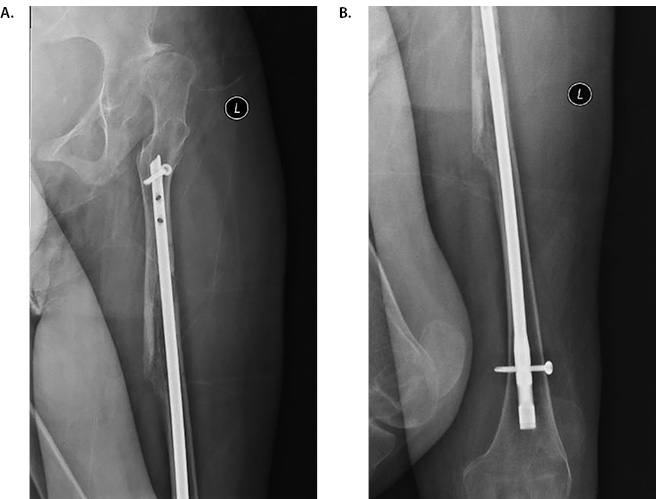
The patient was seen in clinical follow up 2 weeks postoperatively at which time radiographs demonstrated stable fracture alignment. She had resumed bed to chair transfers at this time. She was seen again in follow up 3 months after surgery at which time the fracture had healed (Figure 3A and Figure 3B). At this time, the patient had been having pain and discomfort from her chronic right hip dislocation and hip flexion contracture. This was subsequently managed with resection arthroplasty and soft-tissue releases. At the time of this report, the patient is doing well now one year status post fixation of her femur fracture and has returned to her baseline function.
To our knowledge, this is the first case report to describe successful treatment of a femoral shaft fracture with a retrograde humeral nail. The bony dysplasia associated with our patient’s underlying syndrome added significant complexity to the management of an otherwise common injury pattern. Careful preoperative preparation and contingency planning was essential to a favorable operative outcome.
Sparse literature exists regarding the patient’s underlying diagnosis of Mucolipidosis type IV, a rare lysosomal storage disease occurring secondary mutation in the MCOLN1 gene. The disease exhibits autosomal recessive inheritance with high carrier frequency in individuals of Ashkenazi Jewish descent.7,8 The orthopedic manifestations of this condition are not well-described, but appear to mirror those of cerebral palsy and similar static encephalopathies occurring early in development. Global function in our patient was similar to that of a cerebral palsy patient with gross motor function classification level (GMFCS) five. The hip pathology observed in our patient was also similar to that observed in cerebral palsy patients with increased adductor tone leading to hip subluxation and eventually dislocation. Muscular imbalance similarly produces valgus angulation of the femoral neck and increased propensity for dislocation of the femoral head. Imaging was also notable for moderate thoracolumbar scoliosis, presumptively neuromuscular in origin. Prior studies in patients with cerebral palsy have found a high rate of low-energy fractures, particularly in non-ambulators as a result of low bone density.3-5 Fracture care in these patients is challenging as appropriate immobilization may be hindered by limb contractures and casting may place the patient at risk for skin breakdown. Jones dressing and splint immobilization has been previously recommended for management of most femoral shaft fractures in non-ambulatory patients with cerebral palsy.3 Intramedullary fixation, nevertheless, may be favorable when safe and appropriate.
Careful preoperative planning was essential for successful fracture repair. Earlier studies have described antegrade humeral nail insertion for treatment of femoral shaft fractures in older children and adolescent patients.9,10 Antegrade nailing could not be considered in this case given the patient’s extreme femoral neck valgus. It is important to note that the humeral nail utilized in our case is designed with a 5-degree proximal bend to permit off-axis entry in the humeral head.11 This bend also facilitates retrograde insertion of the nail in the distal humerus via a posterior cortical entry site proximal to the olecranon. For successful, atraumatic passage of the nail through the distal femoral cortex in our patient, it was essential to correct this bend prior to passing the nail. The biomechanical implication of manually correcting the prebend in the nail is not known and has not been previously examined in the literature. Minor plate bending and contouring, however, is routinely employed in fracture fixation surgery without apparent biomechanical disadvantage.
In conclusion, a retrograde humeral nail may be considered a viable treatment option in the care of lower extremity long bone fractures in patients with small stature or circumstances where resources are limited.





{kind=link}
{kind=link}
{kind=link}