More than 42, 000 people undergo surgery for rupture of the anterior cruciate ligament (ACL) annually. 15 The human ACL does not heal spontaneously after rupture. While some have been found to heal with primary repair, the limited success of this procedure 1, 7, 16 has led many orthopaedic surgeons to treat symptomatic ACL rupture with removal of the ruptured fan-shaped ligament and replacement with an isometric tendon graft. 5, 8 While ligament reconstruction appears to initially restore gross stability in most patients, longer follow-up demonstrates many post-operative patients have abnormal structural laxity, suggesting the reconstruction may not with- stand the physiologic forces applied over time. 2 The loss of ACL function has been found to result in early and progressive radiographic changes consistent with joint deterioration.6
 |
Our work focuses on development of a new, cell-based treatment approach: namely, guided tissue regeneration of the ACL after rupture. This approach involves placing a regenerative template, or scaffold, between the ends of the ruptured ligament to facilitate ingrowth of cells into the gap between the remnants. The scaffold could be designed to encourage not only cell migration and proliferation, but also to encourage vascular and nerve ingrowth, as well as collagen and protein production.
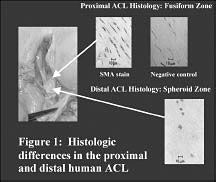
The development of this new method has involved the systematic investigation of several questions related to the biology of the human ACL. To date, we have started the process of defining the cellular distributions in the intact ACL (Figure 1), 13 the histologic response to rupture in the human ACL (Figure 2), 10 and the ability of cells in both the intact 11 and ruptured ACL 14 to migrate to an adjacent scaffold in vitro.
 |
||
|
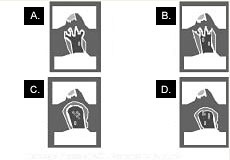
Figure 2 : Schematic illustrating the four phases of the response to rupture in the human ACL. A. Inflammation
0 to 3 weeks Int. Hyperplas Mop-ends Mononuclear |
Our initial work focused on defining the histology of the intact human ACL. By studying longitudinal sections of human ACLs retrieved from patients undergoing total knee arthroplasty, we were able to discover the nonuniformity of cell morphology, cell distribution, and blood vessel distribution throughout the ligament in this patient population. Previous histologic descriptions of ACLs from young animals have suggested a uniform distribution of fibroblasts in a wavy, or crimped, collagen extracellular matrix. In our study of ACLs from human knees with degenerative joint disease, three distinct regions were found, which differed in the cell nuclei morphology and cell number density. 13 This finding is important for future experimental work using this tissue as a cell source as cells obtained from one region not only look differently (Figure 1), but behave differently. Work we presented at the 2001 Orthopaedic Research Society Meeting in San Francisco identified differences in response to TGF-B1 for cells from the proximal and distal ACL. 9
As guided tissue regeneration relies on viable cells in the injured tissue, we also analyzed the cellularity and vascularity in ruptured human ACLs. For this study, ACL remnants were retrieved from 23 patients undergoing ACL reconstruction. After retrieval, the ligaments were fixed and sectioned longitudinally. We found that the ACL differs from tissues which successfully heal in two important ways: first, the remnant is resynovialized, and second, at no time point after rupture is any tissue observed to course between the ruptured ligament ends. 10 The lack of any blood clot in the knee, even in the specimens obtained 10 days after rupture, is consistent with the work of Harrold in the 1960s, when he demonstrated that blood does not clot in the intra-articular synovial environ- ment of the dog. 4 Thus, while extra-articular ligaments, like the medial collateral ligament (MCL), have a blood clot form in the injury site that is subsequently invaded and remodeled by fibroblasts, 3 the ACL doesn't have a blood clot for cells to invade after rupture due to the intrasynovial fibrinolytic environment. Without blood clot to act as the initial provisional scaffold, there is no possibility of scar formation, despite the fact that other processes associated with wound healing, namely revascularization, do occur in the ACL remnants.
 |
||
|
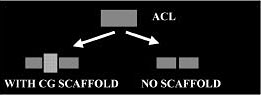
Figure 3: Schematic of experimental design to determine if ACL cells would migrate into an adjacent collagen-glycosaminoglycan (CG) scaffold. |
Our next project was to determine whether the cells intrinsic to the ACL were capable of migrating to an adjacent scaffold if one were provided (Figure 3) . In this inves- tigation of cell migration from intact ACL explants into 3-D collagen-glycosaminoglycan (GAG) matrices, two important findings were made. First, no tissue formation was seen between fascicles that were simply reapposed without an intervening scaffold. The cell density at the edges of the fascicles increased, but no new matrix was visualized. The addition of a scaffold into the gap resulted in cell migration into the gap between fascicles (Figure 4) . 11 We have recently completed studies using radiolabeled proline to demonstrate that the cells in the scaffold are producing new collagen. 12 This suggests that ACL cells are similar to cells in ligaments that heal, such as the MCL, in that they are able to migrate into an adjacent provisional scaffold and begin to make collagen in the wound site. 14
 |
||
|
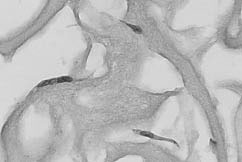
Figure 4: Histomicrograph of ACL cells which have migrated 1 mm into a CG scaffold after two weeks in culture. |
The second important finding of that study was that in specimens where contact was lost between the ligament fascicle and the scaffold -even with a gap of only 50 micrometers - no migration was seen between the fascicle and scaffold. A gap this small is often not visible grossly, and can only be seen microscopically. 14 This might explain the failure of some primarily repaired ligaments, which appear to be grossly in contact, but may in fact have microscopic gaps still present between the frayed ends of ligament. It now seems likely that unless a critical area of the fascicle ends are maintained in microscopic contact, migration into the wound will not occur for the ACL cells in great enough numbers to result in functional healing.
In summary, the clinical problem of the ruptured ACL remains significant. In light of the long-term problems of knee laxity and osteoarthritis associated with loss of ACL function and reconstruction failure, new treatment methods which preserve as much of the complex structure and function of the ligament as possible hold some theoretical promise for improved patient outcomes. The study of the cell biology of the ACL, the response to rupture in the ligament, and the migration potential of cells of the ACL provides a starting point for investigating guided tissue regeneration as a potential treatment method for ACL rupture. Future directions of research include optimization of the regeneration template, both in terms of substrate and additives such as growth factors, determination of the effect of synovial fluid on substrate integrity, and in vivo testing of this method. Continuing to pursue these basic science questions may lead to a new treatment method for patients with ACL rupture.
Martha M. Murray, MD is a Clinical Fellow in Orthopaedic Surgery at Harvard Medical School.
Address correspondence to:
Martha M. Murray, MD
Orthopaedic Research Laboratory
Brigham and Women's Hospital
75 Francis Street
Boston, MA 02115