ABSTRACT
A wide variety of cartilage repair procedures are currently being employed
clinically to treat lesions in the articular surface. However, we still
know little about the reparative process elicited by each and the functionality
of the resulting tissue. That no procedure has been demonstrated to regenerate
articular cartilage underscores the importance of distinguishing the
specific tissue types that result from each procedure so that an evaluation
of their properties and assessment of their serviceable lifetimes can
be made. This is especially critical given the myriad methods available
to treat the same lesion and the wide range of resulting tissues.
Over the past 5 years, the Orthopaedic Research Laboratory of the Brigham and Women's Hospital has employed an animal model to address these issues. A defect made to the level of the tidemark in a canine model has been used in several investigations of a variety of articular cartilage repair procedures. Longitudinal study of the make-up of the reparative tissue in defects treated by autologous chondrocyte implantation and in untreated controls has been carried out through 18 months post-operatively. Direct comparison of a wide variety of repair methods including microfracture has been performed in cross-sectional studies at 16 weeks postoperatively. These results have provided useful insights into the make-up of the tissues resulting from these procedures and an appreciation of the dynamic remodeling that can occur with time. These data may be useful for the comparison of cartilage repair procedures and could be used to design future strategies for cartilage repair.
INTRODUCTION
In recent years several procedures have been introduced for the treatment
of defects in articular cartilage. Many of these treatment modalities
have yielded promising clinical results in the first postoperative year
of their use. However, our incomplete understanding of the composition
and structure of the reparative tissues that form at the treatment sites
and of the effects of the treatments on the neighboring tissues compels
the investigation of these procedures in animal models that enable complete
evaluation.
Understandably, a principal parameter for assessing the value of a new cartilage repair procedure is pain relief. However, it follows that as we know so little about the source and cause of the pain that propels the patient to surgery, we are illequipped to directly relate the symptomatic relief to any aspect of the procedure or feature of the reparative tissue. Moreover, we cannot predict the course of the outcome:How long will the pain relief last? Confounding aspects of the assessment of new cartilage repair procedures include a lack of understanding of the natural history of certain lesions and the impact of concurrent procedures such as osteotomy and meniscal and ligamentous repairs on the symptomatic relief. Would the lesion sufficiently heal and the symptoms be relieved with no treatment? Is it the adjunctive procedure, such as osteotomy, that has provided the relief or the cartilage repair procedure? Finally, when relying on pain as the principal outcome, one must also consider the possibility of a placebo effect.
Objective measures of the reparative tissues filling the defects can deepen our understanding of treatment effects and can provide a rational basis for their comparison. Such comprehensive objective evaluations require the use of animal models. Biopsies of tissue from human subjects are available for study only occasionally and rarely from asymptomatic individuals. Certain noninvasive diagnostic techniques (viz . , magnetic resonance imaging) still require further development before they can provide a detailed assessment of the physical and chemical changes in the lesion with treatment.
Animal models can be of value for both longitudinal and cross-sectional studies. The former can provide a useful picture of the chronology of the reparative process induced by the procedure. These data can provide a foundation for the evaluation of biopsies from human subjects and thus may be of predictive value. Cross-sectional studies are of value for the direct comparison of repair procedures with respect to selected measures. This paper provides a brief review of the use of animal models for the assessment of cartilage repair procedures and reviews the findings obtained from one such animal model. Much of this paper is drawn from a recent review.
ANIMAL
MODELS FOR EVALUATING CARTILAGE REPAIR PROCEDURES
Studies of the healing of cartilage defects have been carried out in many
animal models including the rabbit, 2,
3 goat,
4 sheep,
5 dog, 6,
7 and horse. 8
The thickness of the cartilage and the chondrocyte behavior in these species
differ markedly from the thickness and cellular behavior in human tissue.
Moreover, all animal models are limited in their ability to mimic human
conditions particularly with respect to joint mechanics. Finally, the
principal outcome in the human pain cannot yet be meaningfully evaluated
in the animal models. These limitations notwithstanding, animal models
have been of great value in the assessment of the benefits and potential
problems of new cartilage repair procedures.
A principal limitation of the most commonly employed animal model, the rabbit, is that the defect depth is limited by the thickness of the articular cartilage in the rabbit knee joint (generally less than 0. 5 mm) . The thicker articular cartilage layer (approximately 0. 5 to 1. 0 mm) in the dog improves this condition, and the activity level and loading more closely resemble human conditions.
Healing may be affected by animal age, as studies performed in adolescent species have reported good healing compared to other studies. 9 While it has been known for many years that chondrocyte response to injury may be age dependent, only recently has a study conclusively shown agedependent differences in repair in the rabbit. 10 Because a treatment modality that would work only in young patients (prior to skeletal maturity) would be limited in its applications, adult models are preferred for assessing more clinically applicable tests of efficacy.
THE
CRITICAL SIZE DEFECT: THE EFFECTS OF DEPTH ON HEALING
There is, in effect, no "critical size defect "the size of
defect above which no healing ensues for articular cartilage because
even a defect as thin as a knife-edged incision may manifest no sign of
healing, i. e. , no filling with reparative tissue. The critical dimension
of a defect in articular cartilage that serves as a determinant of the
process of healing is depth: defects that do not penetrate the calcified
cartilage versus those that do. For the purpose of this paper, the former
will be referred to as "chondral "and the latter, "osteochondral.
"
Defects fully contained in articular cartilage (i. e . , chondral defects) may persist with no sign of reparative tissue filling the lesion 11 or may heal with limited filling by fibrous tissue, fibrocartilage, or hyaline cartilage. Remarkably, in some cases, the reparative tissue that fills such (untreated) defects displays the structure of articular cartilage. Such findings suggest that articular cartilage has potential for regeneration. However, such regeneration has never been fully demonstrated throughout the defect.
When healing occurs in chondral defects, the source of the cells filling such lesions remains in question. The first of the following possibilities seems the most likely:
- blood and marrow (i. e . , marrow stromal stem cells) accessing the lesion through undetected fissures through the calcified cartilage and subchondral bone;
- cells from synovial processes growing over the intact cartilage surface to gain access to the defect;and
- cells settling
out from synovial fluid.
Ironically, the least likely source of cells is the surrounding articular cartilage, because the cells are so restricted in their movement by their extracellular matrix. The fibrin clot that is required to serve as the provisional scaffold to retain cells in the defect could be derived from various sources. These include blood from undetected fissures through the calcified cartilage (as in 1 above) or blood within the joint from the synovium caused by the trauma or surgery that produced the lesion.
While complete regeneration of chondral defects in the postnatal animal has never been reported, such regeneration has recently been reported in the fetus. 12 Variable healing of defects in the postnatal mammal has been found to be similar for many species and the same for immature as well as mature animals. 11 In contrast, defects that penetrate the subchondral bone more regularly show filling of the defect with reparative tissue due to the introduction of reparative cells from blood vessels and the marrow. 13 While complete filling with hyaline cartilage has been reported it did not persist.
Little is known about the course of healing of defects that extend to the tidemark, but that do not initially penetrate the subchondral plate. Such lesions can occur as a result of trauma and are now often created surgically as degraded cartilage is debrided from the joint surface in preparation for certain cartilage repair procedures. In one technique cartilage is removed to the tidemark in preparing a defect for implantation of cultured autologous chondrocytes injected under a periosteal graft. 14 Careful characterization of untreated lesions is critical to the understanding of new treatments to regenerate articular cartilage. However, there are no clinical reports of how an untreated full-thickness chondral lesion heals, and work in animal models has produced limited data. Grande, et al . 3 studied four such defects in rabbits. After six weeks, two of four untreated defects contained no repair tissue, while the other two animals displayed reconstitution of the matrix in approximately 16% of the cross-sectional area of the defect, predominantly in the sides and corners. Brittberg observed six similar defects in the rabbit at twelve weeks, reporting 29% filling with a predominantly "disorganized, dense fibrous tissue ". 14 There is a need for more complete characterization of the spontaneous healing of this type of defect.
METHODS
OF EVALUATION
There are three primary methods for evaluating the outcome of healing
cartilage in an animal model:histology, biochemistry, and mechanical properties.
Interestingly, none of these match the criteria used for evaluating clinical
success: pain relief and function. Other clinical assessments that can
be made through arthroscopic procedures include viewing or probing the
surface. However, these results do not always correlate with patient symptoms,
and thus are not used as reliable indicators of healing.
In experimental work, most authors use histological methods to evaluate cartilage repair. Various factors in the repair process can be evaluated by histology:types of tissues filling the defect (including both cell and extracellular matrix characteristics) , attachment to adjacent structures (cartilage, calcified cartilage, or bone) , and the health of the adjacent tissues. The method of staining may also be useful in eliciting biochemical information. For example several staining methods are specific to sulfated glycosaminoglycans (Safranin O, alcian blue) , while immunohistochemical stains can be used to demonstrate the types of collagen and cartilage specific proteins. Finally, histology can reveal structural information, primarily collagen organization, which may provide information regarding the functionality of the reparative tissue.
A semi-quantitative schema for assessing the degree of degradation of articular cartilage the Mankin scale 15 has recently been applied for the quantitative assessment of the success of cartilage healing in reparative procedures. 16, 17 However, this approach must be exercised with caution. The use of an ordinal semi-quantitative scale limits use of parametric statistical methods. More recently, quantitative histological methods have been for the evaluation of the reparative tissue in defects in animal models. 7, 18 In one approach, heretofore applied to rabbit investigations employing osteochondral defects, the strategy is to obtain a quantitative description of the degree of cartilage restoration:repair dimensions, degree of attachment, surface roughness and repair location. 18 The other approach, 7 implemented for the analysis of the reparative tissue in chondral defects in a canine model, determines the areal percentage of selected tissue types in the defect and the percentage bonding to the adjacent articular cartilage and underlying calcified cartilage.
Other methods of analysis are more specialized and may complement histological analysis. The measurement of mechanical properties of reparative tissue may indicate the degree to which the tissue functionally replaces normal cartilage. The major variables include modulus of elasticity and permeability. Biochemical analysis is normally focused on synthesis of the major components of the cartilage extracellular matrix:collagen and proteoglycans. Use of these methods has been limited, in part, due to the destructive nature of the typical ex vivo testing procedures which prevents histological analysis of the same tissue.
It would be desirable to have information from all of these tests. However, practical limitations of the research, including the limited size of defects and expense of animal models, often make this impossible. For a preliminary investigation of healing, histology provides the widest range of information and is widely accepted. Mechanical and biochemical evaluations are more appropriate for specialized follow-up studies. Advances in mechanical testing, including non-destructive probes which may be used in vivo , promise to expand its implementation in the analysis of cartilage repair.
CARTILAGE
REPAIR METHODS BEING EVALUATED IN ANIMAL MODELS
In general, efforts to regenerate tissues focus on manipula-tion of the
three pillars of tissue engineering:cells, matrices, and soluble regulators.
Most of the recent approaches for cartilage repair of chondral defects
include one or more of the following techniques:
- Providing a matrix, carrier, or support for cells to facilitate, or direct, synthesis of new cartilage.
- Providing a new population of cells to express the chondrocytic and to synthesize new cartilage. This source may be an autogenous or allogeneic tissue graft, or cells manipulated in culture.
- Inducing existing chondrocytes to more actively repair the defect through enhanced proliferation, migration, and synthesis, often through the use of soluble regulators (i. e., cytokines or growth factors) .
This paper addresses the first two of these methods. A procedure for providing access of cells from blood and marrow to the defect through "microfracture " 19 of the calcified cartilage and subchondral bone is included for comparison.
An important factor to consider in treating a defect in articular cartilage is the post-procedure motion and loading to which the joint will be subjected. Before or after injury, there is clearly an acceptable range of loading and motion outside which cartilage begins to degrade. No loading at all can lead to joint degeneration, while excessive loading can create pathology in the cartilage and underlying bone. A series of studies in animal models has demonstrated the ability of controlled motion to improve the reparative process in certain defect types subjected to certain treatments. 20 While not the subject of this work, the postoperative loading should be investigated in any model of cartilage repair.
COMPARISON
OF SELECTED PROCEDURES IN A CANINE MODEL
The following summarizes investigations conducted in the Orthopaedic Research
Laboratory of the Brigham and Women's Hospital over the past 5 years involving
several students, research fellows, and faculty. The consistency among
the studies was assured by having most of the surgeries performed by one
individual (H-P. Hsu, M. D.) and most of the histological evaluations
overseen by one individual (H. A. Breinan, Ph. D.) .
A canine model was employed for reasons of cartilage thickness, accessibility of the surgical site, reproducibility of the lesion, animal activity, and loading of the joint. An adult animal was used to reflect the challenge of repair most often seen clinically. The chondral lesion that was implemented mimics situations that are often the direct result of injury or debridement. In this work the following procedures were evaluated:
a) cultured autologous chondrocytes (CACs) injected under a periosteal flap; 7, 21
b) periosteal, 7, 21 type I and II collagen, and fascia flaps alone; 6
c) CAC-seeded collagen matrices; 6, 22 and
d) microfracture-treated defects with and without aug mented implantation of a collagen scaffold. 22
Untreated defects were used as controls. 23 Reparative tissue filling the defects was evaluated after selected time periods. A longitudinal study of the first of these procedures was conducted through 18 months post-operatively. Results of all procedures were compared in a cross-sectional study performed 13-16 weeks post-surgery.
The chondral defect was a 4 mm diameter hole created in the articular cartilage of the trochlear groove of the stifle joint (knee) of the adult mongrel dogs. 7, 23 The trochlea was selected over sites on the femoral condyles and tibia because it was more accessible surgically while having a comparable thickness of articular cartilage. It was chosen instead of the patella because, in the dog, it provided a larger surface area to accommodate 2 defects, 4 mm in diameter, while having an articular cartilage thickness comparable to that of the patella. Moreover, it had a flatter profile than the sites on the patella. Finally, the patello-femoral articulation is highly loaded, thus providing a meaningful test of the cartilage repair procedure.
CHRONOLOGICAL
CHANGES IN THE COMPOSITION OF THE REPARATIVE TISSUE IN DEFECTS IMPLANTED
WITH CULTURED AUTOLOGOUS CHONDROCYTES
7, 21
By 1. 5 months, reparative tissue formed in defects treated with the CACs
and in the two control groups:defects implanted with the periosteum alone
and untreated defects. The average filling was about half of the defect.
Most of the tissue filling the defect was fibrous tissue or fibrocartilage
(Figs. 1 and 2) , with little hyaline and rarely articular cartilage.
In some cases, features consistent with remnants of the periosteum cover,
or cell overgrowth, were present. The elongated fibroblasts and collagenous
matrix of the fibrous tissue were aligned parallel to the surface. Immunohistochemistry
revealed the presence of type I collagen and the absence of type II collagen.
This fibrous tissue was occasionally found to contain cleavages running
longitudinally and the tissue was separated from the calcified cartilage
in some cases. Of note was the fact that when this fibrous tissue was
integrated with the tissue forming the base of the lesion, that tissue
was cartilage which communicated with the subchondral bone. It was also
interesting that the fibrous tissue often appeared to integrate with the
surrounding articular cartilage, and in some cases it appeared that this
alone was retaining the reparative tissue in the defect. In the 1. 5-month
specimens, when present, chondrocytic cells were in greater numbers near
the base of the lesion than in the middle or surface regions of the reparative
tissue. Evidence of resorption of the underlying bone with fracturing
of the subchondral plate could be found in some sections with reparative
tissue bridging between the bone and the defect site.
Defects evaluated after 3 and 6 months displayed a striking increase in the amounts of hyaline and articular cartilage (Figs. 1 and 2) as the relative percentage of fibrous tissue decreased. Analysis of variance revealed significant effects of time on the percentages of fibrous tissue (P<0. 0002) and hyaline cartilage (p<0. 03) . After 3 months, the CAC-treated sites were found to have more total filling (two-tailed paired t-test;p=0. 04) and combined hyaline and articular cartilage (p=0. 0003) than the untreated controls. There were, however, no statistically significant differences in these variables after 6 months.
 |
||
|
1. Histology of chondral defects treated with cultured autologous chondrocytes after (a) 1. 5, (b) 3, (c) 6, and (d) 12 months postoperative. (a) Hematoxylin and eosin stain and (b-d) Safranin O/fast green stain. |
e distribution of tissue types within the defect was notable in that the hyaline cartilage, when present, was found near the base of the lesion and at the corners with fibrocartilage superficial to it and fibrous tissue was almost always on the surface. This fibrous tissue frequently displayed delamination and fibrillation. Type II collagen immunolabelling of the hyaline cartilage and some of the fibrocartilage was in evidence. Also of note was the presence of articular cartilage along the base of the lesions in several specimens. This cartilage showed a normally appearing integration with a calcified cartilage layer. It was not infrequent, however, to find vertical clefts through the hyaline and articular cartilage. Compared to the 1. 5-month postoperative time period, at 3 and 6 months the fibrocartilage tended to display increased amounts of safranin O staining. The staining for proteoglycan in the hyaline cartilage also increased with postoperative time reaching normal levels in some areas. Bone formed in small quantities at the base of one defect; however, no neovascularization was found in the defect area at this time. The histological features of the reparative tissue at 3 and 6 months postoperative, when compared to the 1. 5-month findings, suggested a remodeling process. During this remodeling phase, the ACI-treated group contained more hyaline and articular cartilage, and less fibrous tissue than untreated controls (no periosteal controls were included at this time) . At 12 and 18 months there was no significant effect of the cultured autologous chondrocyte-implanted defects when compared with controls. The percentage of the defects filled with reparative tissue was less than that in the 6-month defects (Figs. 1 and 2)
 |
||
|
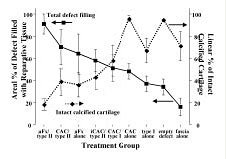
3. Graph depicting an inverse relationship between total defect filling and remaining intact calcified cartilage for 15-week canine implant groups and controls. µfx, microfracture;type I and II, collagen implants;CAC, cultured autologous chondrocytes; and iCAC, initial experiment. The coefficient of determination (R2) for the areal percentage fill versus the percentage of non-intact calcified cartilage is 0. 61 by linear regression analysis. |
 |
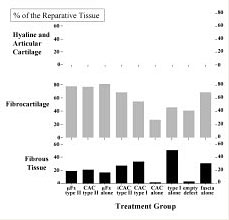
2. Composition of reparative tissue in all groups at 15 weeks. Mean contributions from each tissue type are normalized by the total percent defect filling for the group. . µfx, microfracture;type I and II, collagen implants;CAC, cultured autologous chondrocytes;and iCAC, initial experiment. |
.
COMPARISON OF REPARATIVE TISSUES IN DEFECTS TREATED BY SELECTED PROCEDURES,
AFTER 15-16 WEEKS
There was wide variability in the tissue types comprising the reparative
tissue in the chondral defects that underwent treatment with the variety
of cartilage repair procedures (Fig. 2) . There were certain trends noted
in the distribution of selected tissue types throughout the lesion. Hyaline
cartilage was always found superficial to intact calcified cartilage,
while damaged calcified cartilage was covered only by fibrous tissue or
fibrocartilage. When found, articular cartilage was superficial to an
intact calcified cartilage layer, and appeared to form more frequently
in the corners of the defects. Fibrous tissue was most commonly found
at the surface of the reparative tissue and was generally superficial
to fibrocartilage.
The percentage of the original area of the chondral defects that filled with reparative tissue varied widely from less than 20% for defects treated with a fascia cover alone to more than 90% for microfracture-treated lesions in which a type II collagen matrix was implanted (Fig. 2) . Untreated defects displayed approximately 40% fill. At this time period, the lesions in which CACs were implanted under a periosteal flap were found to be filled to approximately 50% with tissue.
The relative amounts of the specific tissue types comprising the reparative tissue also varied widely (Fig 2) . There was so little articular cartilage in any group that this category was combined with hyaline cartilage for the purpose of this analysis. The greatest percentage of hyaline cartilage was found in the CAC-implanted group followed by the untreated controls (Fig. 2) . The majority of the reparative tissue in the other treatment groups consisted of fibrocartilage. The greatest amount of fibrous tissue was found in the defect implanted with the type I collagen scaffold alone.
Of some interest was the marked difference in the treatments in which the CACs were implanted alone versus seeded in a collagen matrix. The cell-seeded matrix had approximately 45% more reparative tissue in the defect (Fig. 2) but the make-up was predominantly fibrocartilage compared to the hyaline cartilage that predominated in the defects treated with the CACs alone (Fig. 2).
There was a meaningful inverse correlation between the percentage of the defect filled with reparative tissue and the percentage of the intact calcified cartilage (Fig. 3) . Linear regression indicated that 61% of the variation in the fill with reparative tissue was explained by the amount of intact calcified cartilage (R 2 =0. 61) .
LESSONS
TO BE LEARNED
None of the procedures investigated in the canine model resulted in the
regeneration of articular cartilage in the majority of the defect. Moreover,
it is not yet possible on the basis of the animal study to determine which
procedure would be the most suitable for a specific clinical problem.
There are, however, lessons that can inform future research.
THE
REPARATIVE TISSUE IN CHONDRAL DEFECTS COMPRISES SEVERAL TISSUE TYPES
For every cartilage repair procedure there are several tissue types comprising
the reparative tissue. This heterogeneity of the make-up of the reparative
tissue cannot be as appreciated using certain methods of evaluation that
assign a single grade to the repair. Moreover, until we understand the
role that each tissue type can play in the tribology of the reparative
tissue at the site we will not be able to meaningfully predict the functionality
of the repair.
THE
REMODELING OF REPARATIVE TISSUE IN CHONDRAL DEFECTS CONTINUES BEYOND ONE
YEAR
The remodeling of the reparative tissue is notable for 1) the degree to
which it occurs, and 2) its time scale. Lesions that have a predominance
of fibrous tissue within 6 weeks postoperative, can present with predominantly
hyaline cartilage after several ensuing months. Of particular interest
in this regard is that fibrous tissue of a similar character would be
considered a terminal scar if found in lesions in other organs. Moreover,
the replacement of such fibrous tissue with hyaline cartilage or even
fibrocartilage demonstrates the full degree to which degradation of the
early-formed tissue (i. e . , the fibrous tissue) must have occurred and
been followed by the de novo synthesis of cartilage. That the profile
of tissues filling the treated defects after 12 months can be so different
than that seen at earlier time periods provides some indication of the
time scale over which the remodeling occurs. These lessons signal the
caution that must be exercised in anticipating the final state of a reparative
process by analysis of a single biopsy (particularly if taken within one
year of the procedure) .
COMMUNICATION
WITH SUBCHONDRAL MARROW CAN OCCUR EVEN WITH DEFECTS THAT ARE INITIALLY
CONTAINED WITHIN ARTICULAR CARTILAGE
The chondral defect employed in this work, which in some cases became
osteochondral over time, needs to be distinguished from more shallow defects
in which the bone is always preserved. Complete removal of cartilage subjects
the subchondral plate to mechanical forces high enough to cause fractures
during the healing period. In addition, it might be suspected that the
very thin calcified layer and limited subchondral plate in the canine
are more susceptible to damage at surgery. A similar finding was recently
reported in a goat model 24
in which articular cartilage also was removed down to the calcified cartilage.
Despite the fact that damage to the calcified layer and reactions in the
bone significantly affect the repair mechanisms and are not predictable,
the canine model is able to distinguish among a wide variety of cartilage
repair procedures. Moreover, the conditions extant in the canine chondral
defect during the process of healing reflect conditions in debrided defects
in human subjects. Not only may perforations of the subchondral plate
occur postoperatively as they may have in the dog model, but in many cases
defects are being treated that display frank bleeding at the time of the
treatment for which some type of cautery is often required.
THE
AMOUNT OF DEFECT FILLING AND THE MAKE-UP OF THE REPARATIVE TISSUE IS RELATED
TO THE AMOUNT OF DISRUPTION OF THE SUBCHONDRAL PLATE
The value of employing a chondral defect was indicated in part by the
relationship between the degree to which the calcified cartilage and
subchondral plate was disrupted, the degree of defect filling, and the
make-up of the reparative tissue. The less the disruption and remodeling
of the subchondral plate, the less the filling of the defect but the greater
the relative percentage of hyaline cartilage comprising the reparative
tissue. These findings demonstrate the importance of the presence of an
intact calcified cartilage layer to the regeneration of articular cartilage.
On the other hand, the defects that had the greatest percentage of hyaline
cartilage also had the least amount of filling. The importance of the
degree to which the lesion has been filled with reparative tissue with
a serviceable surface layer is evidenced by the prior report that defects
filled with the greatest amount of hyaline cartilage but only 50% filling
failed to survive to 1 year implantation . 7, 25 It is not yet possible
to determine the relative effects of the degree to which a defect is filled
with reparative tissue and the composition of that tissue (i. e. , fibrocartilage
versus hyaline cartilage) on the function of reparative tissue in cartilage
defects. Longer-term clinical follow-up of microfracture 19
and CAC implantation 14
will help to answer this question.
It is not yet possible to determine the relative effects of CACs and collagen matrices on the remodeling of the calcified cartilage and subchondral bone, and on the longerterm outcome of treatments employing these elements. This further underscores the multifactorial nature of the problem of treating cartilage defects.
That the degree to which the calcified cartilage and subchondral bone has been disrupted has a significant effect on the amount of reparative tissue in the defect indicates that the blood and marrow are important sources of reparative cells and the provisional scaffold (i. e . , the fibrin clot) . These results also indicate an association between the degree to which the calcified cartilage layer is damaged and the type of tissue at the base of the defect. Hyaline cartilage is generally found superficial to intact calcified cartilage, while damaged calcified cartilage is covered by fibrous tissue or fibrocartilage. It was not determined whether the hyaline cartilage formed preferentially on intact calcified surfaces, or the formation of the hyaline cartilage played a role in healing damaged calcified cartilage. The fact that hyaline cartilage was more frequently found overlying an intact calcified cartilage layer suggests the importance of an avascular environment for the formation of this tissue type. Moreover, a calcified cartilage layer exposed by surgery may be important in facilitating the bonding of reparative tissue to the base of the defect. Generalized demineralization of calcified cartilage exposed to joint fluid or focal cell-mediated resorption followed by remineralization may be necessary for incorporation newly synthesized collagen fibers.
SUMMARY
In this study, as in the majority of animal models, the primary outcome
variable was histology, whereas in clinical work it is pain relief. In
addition, the activity level and conditions of loading can differ from
the animal model to the human subject. To what extent the canine model
provides an accelerated reflection of healing in the human has not yet
been established. As with any animal model, the results from this work
should be interpreted with caution and efforts should be made to verify
them in human studies.
Myron Spector, PhD is a Professor in Orthopaedic Surgery (Biomaterials) at Harvard Medical School.
Address correspondence to:
Myron Spector, PhD
Orthopaedic Research Laboratory
Brigham and Women's Hospital
75 Francis Street
Boston, MA 02115