This paper describes the preliminar y experience at Children's Hospital, Boston in the application of a vertical expandable prosthetic titanium rib (VEPTR) implant for the treatment of thoracic insufficiency syndrome (TIS)and congenital spinal deformity. The term thoracic insufficiency syndrome was first introduced in 1993 by Campbell 1 to describe the inability of the thorax to satisfactorily support lung growth, respiratory function or spine development due to congenital and acquired chest wall, spine and other syndromic deformities. Examples of TIS include unilateral hypoplastic thorax and spinal deformity associated with combined congenital scoliosis and rib fusions, and bilateral restrictive thoracic hypoplasia associated with Jeune syndrome (asphyxiating thoracic dysplasia)or Jarcho-Levin Syndrome (multiple vertebral and rib fusion anomalies). Conventional spinal arthrodesis for progressive congenital spinal deformity may exacerbate thoracic insufficiency by stopping growth of an already short spine. Moreover, there is no standard treatment for the usually fatal TIS associated with Jeune or Jarcho-Levin syndromes. Campbell and coworkers 2 pioneered the use of expansion thoracoplasty and VEPTR chest wall distraction to treat TIS. The initial procedure consists of one or more opening wedge thoracostomies and insertion of one or more VEPTR devices, one of which may include a spinal distraction hook (hybrid VEPTR device). The thoracostomies of the hemithorax are expanded maximally at the initial procedure and the devices are placed to stabilize the correction. Repeated surgeries to lengthen the VEPTR are performed on an outpatient basis at appropriate intervals to further correct deformities of the thorax and spine. The device and procedure are still under investigational protocol, but preliminary results 2 suggest that expansion thoracostomy and use of a VEPTR device directly treats segmental hemi-thoracic hypoplasia by lengthening and expanding the constricted hemithorax, and indirectly treats scoliosis without the need for spine fusion, with probable benefit for the underlying lung. Experience thus far suggests that this procedure is an alternative to early arthrodesis for some severe and complex congenital spinal and chest wall deformities, and may be an effective surgical treatment for TIS associated with Jarcho-Levin, Jeune and other constrictive thorax syndromes.
1.
INTRODUCTION
1. 1 THORACIC INSUFFICIENCY SYNDROME
Thoracic Insufficiency Syndrome (TIS)has been defined by Campbell et al
. 2 as the inability of the thorax to support normal respiration or lung
growth. TIS can be associated with severe malformations of the chest,
spine or ribs that result in small thoracic volumes and inadequate lung
development, thoracic stiffness and lack of compliance, or prior iatrogenic
alterations of spine or thorax resulting in respiratory insufficiency.
6, 7 Normally
the spine and ribs act together as a dynamic biomechanical structure,
which can only work efficiently at respiration within certain parameters.
3, 4 When
a significant deformity of the thoracic cage exists, it changes the dynamics
of this system, and can interfere with normal respiration and lung development.
Severely compromised respiratory function in the growing child is typically
associated with failure to thrive, as well as the need for frequent hospitalizations
associated with respiratory infections. 5
Although some TIS patients may appear to do well during early childhood,
as body mass increases the fixed thoracic volume may prove insufficient
in later childhood or adulthood. 6
The contribution of early spinal fusion to TIS is not well documented,
but is strongly suggested by experience. A recent preliminary radiographic
review (Campbell and Emans, unpublished data) 8 of eight Children's Hospital
patients who underwent spine fusion at age 5 years or younger was undertaken
as a pilot analysis for a related study. Average followup after fusion
was 12 years, and all patients had reached maturity. Thoracic spine length
averaged 50 percent of normal, as would be expected from spine fusion
performed early in growth. However, mean transverse diameter of the thorax
at maturity was only 19.3 cm, or approximately 50 percent of published
normal values. None of these patients had preexisting chest wall abnormalities.
Some patients may have had coexistent restrictive lung disease. Two additional
patients with thoracic hypoplasia following early spine fusion developed
severe respiratory insufficiency. The first patient, age 16 years, has
a vital capacity of 20 percent predicted and requires chronic nasal oxygen
and intermittent ventilator support. The second patient had a thoracic
spinal height of only 13 cm with a thoracic width of 18. 5 cm at age 19.
At age 22, her vital capacity was 20 percent predicted, and she developed
respiratory insufficiency with CO 2 retention. At age 25, she died of
respiratory infection. This preliminary review suggests that young children
undergoing spine fusion for scoliosis may go on to develop severe thoracic
hypoplasia, associated restrictive lung disease and respiratory insufficiency
in young adulthood. 2.
SURGICAL
INDICATIONS
2. 1 RIB FUSION AND PROGRESSIVE SCOLIOSIS
In normal patients, the thoracic spine is maintained in a state of equilibrium
by balance of opposing forces from the ribs. Imbalance in these areas
can result in spinal deformities. Rib fusion and scoliosis often occur
together in patients with congenital skeletal deformities. Congenitally
fused ribs typically cause curvature of the spine toward the area of involvement.
In some cases, rib fusion can also occur following thoracotomy. 9,
10
A study of patients with widespread thoracic congenital scoliosis treated with fusion found that patients with rib fusion had a significant reduction in pulmonary vital capacity values at follow-up. 11 Regardless of which deformity occurs first, the combination of scoliosis and rib fusion can severely restrict the thorax and not allow the lungs to develop properly.
 |
|
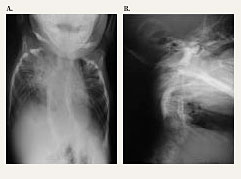
| Figure 1. AP and lateral chest radiograph of patient with Jarcho-Levin syndrome at 2 months of age shows crab-like chest appearance and limited bilateral lung aeration and multiple rib and vertebral body abnormalities. |
2.
2. HYPOPLASTIC THORAX SYNDROME
Hypoplastic thorax refers to underdevelopment of the chest. It is commonly
observed in rare congenital conditions, such as Jeune's Syndrome, achondroplasia,
Ellis van Crevald Syndrome, Jarcho-Levin Syndrome (Figure
1), and VACTERL syndrome (Figure 2).
The estimated incidence is 1 in 125, 000 births for Jeune's Syndrome,
13 and 1
to 4 in 25, 000 births for achondroplasia. 14 No incidence figures have
been reported in the literature for Ellis van Crevald Syndrome or Jarcho-Levin
Syndrome.
Only 43 cases of Jarcho-Levin Syndrome have been reported in the literature. 12 Jarcho-Levin Syndrome has been described as a lethal autosomal recessive form of short dwarfism. Also called spondylothoracic dysostosis, it is characterized by extensive vertebral and chest-wall abnormalities, including a symmetric "crab-like" chest that is caused by the ribs crowding and fusing at their origin at the spine and fanning out along their lengths. Patients affected with Jarcho-Levin Syndrome can have various numbers and shapes of ribs as well as vertebral segmentation defects consisting of fusion or absence of vertebrae, hemivertebrae, and butterfly vertebrae. Mild scoliosis, secondary to the multiple hemivertebrae, is present in most patients. The existence of multiple bony abnormalities of the thoracic cavity can cause marked respiratory compromise and lead to death. 12
 |
|
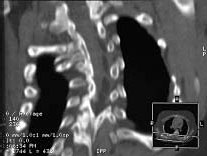
| Figure 2. CT-scan of a 2-year old with VACTERL syndrome and progressive congenital lordo-scoliosis with bilaterally diminished lung volumes and hypoplastic hemithorax. Multiple rib and vertebral body anomalies are present including a bony postero-lateral bar and concave rib fusions. Conventional treatment of this problem would be by anterior and posterior spinal fusion, which likely would halt the progressive curvature, but further shorten an already short thoracic spine and contribute to hypoplastic thorax and respiratory insufficiency (TIS). Alternatively, expansion thoracostomies and insertion of VEPTR device with repetitive distraction offers control of the progressive curve during growth while expanding the hemi thorax and encouraging lung growth. Ultimately spinal fusion would probably be needed, but preferably at an older age, after more spine, lung and thoracic growth was achieved. |
The condition is seen in two forms:mild and serious. The dominant type, known as spondylocostal dysostosis , seems to be a milder abnormality and patients may have an essentially normal life span although death at infancy has been reported. In contrast, the severe form of this condition is the autosomal recessive type and tends to be a more lethal form of the syndrome, with death due to respiratory insufficiency commonly occurring within the first 2 years of life. 12
Jeune's Syndrome is an autosomal recessive skeletal disorder with major manifestations in the thoracic cage. 14-22 The narrow bell-shaped chests and short horizontal ribs seen in children born with Jeune's Syndrome often result in early deaths due to respiratory failure. 18, 20, 21 Some patients with a mild form of the syndrome survive infancy, but develop progressive renal failure later in their childhood. A total of 93 juvenile cases involving respiratory problems have been compiled. 14-22 Of these 93 cases, 51 patients had died at the time the articles were submitted for publication. Deaths occurred from before birth (1 elective abortion, 1 stillborn) until the age of 4 years 2 months.
2.
3. FLAIL CHEST
In flail chest, the chest wall is destabilized either due to congenital
causes (e. g. , rib agenesis), acquired causes (e. g. , separation of
thoracopagus conjoined twins, resection of ribs because of tumor), or
trauma. Reportedly, 1 in 300 births has some sort of congenital chest
deformity. 31
However, only 42 known cases of congenital flail chest have been described
in children under the diagnosis of "Cerebro-costalmandibular Syndrome."
25 Children with this syndrome display rib gaps causing a very narrow
thorax, hollow chest and other deformities. Among the 42 juvenile cases
reported in the literature, 33 had associated respiratory difficulty,
and 25 died. No reconstruction or other intervention was described, nor
was there long-term follow-up on the survivors. Another study presents
data on 18 children with congenital chest wall deformities or malformations
of various degrees of severity. 26 Of these 18 children, 15 were either
stillborn or neonatal deaths.
 |
Figure 3. The VEPTR device is shown implanted in a child multiple congenital vertebral anomalies and progressive scoliosis. The implant's curvature conforms to the shape of the thoracic cage. The rod is placed vertically along the chest wall by attaching each end to healthy ribs above and below the opening wedge thoracosotomies. |  |
Figure 4. Vertical Expansion Prosthetic Titanium Rib (VEPTR) Device consisting of extensible titanium rod/sleeve constructs of varying length. Two radii of curvature are available for different applications to conform to or modify the surface contour of the thoracic cage. Ringlike capturing devices (rib cradle and end cap)on each end are placed around one or two healthy ribs above and below the expansion thoracostomies for chest expansion. The basic configuration consists of superior cradle, cradle end halves, cradle locks or rib sleeve, inferior cradle, or lumbar extension, and distraction locks. The inferior cradle may be replaced with a lumbar extension rod/hook combination to act as a spinal distraction device (hybrid device). With growth, the rod/sleeve is extended (distracted)through a small incision. When maximum length is achieved, the rod/sleeve is replaced with a longer construct. |
Thoracopagus conjoined twins may be separated surgically if they have independent hearts and great vessels. The obvious result is a large chest wall defect in one or both individuals. Although the literature estimates 50%survival for all separated conjoined twins, 27 mortality figures for separated twins with such chest defects have not been identified.
Resection of pediatric chest wall tumors typically necessitates the removal of several ribs, resulting in a large chest wall defect. 28 The long-term result of such extensive surgery is scoliosis, which curves toward the side of the rib resection. Scoliosis has been reported in 90 to 100%of patients who underwent thoracoplasty (surgical rib resection). 28 The scoliosis is progressive, and the younger the patient is at the time of resection, the more severe the progression.
Walton et al. 29 reviewed the case histories of 11 patients (five adults and six children)who presented with scoliosis after multiple rib resection for several disorders. All 11 cases developed progressive scoliosis with concavity directed toward the side of the rib resection, and the younger the age at the time of rib resection, the more severe the progression. The rate of progression was greatest during the first ten years after rib resection. The five patients who presented as adults were treated in several ways, with only one requiring spine fusion. However, five of the six children required spine fusion to prevent progression of scoliosis. Despite these surgical interventions, scoliosis towards the prior rib resection resulted in all cases.
3.
THE TITANIUM RIB IMPLANT
The titanium rib 2,
6, 31 is an implantable, expandable prosthetic device used in conjunction
with opening wedge thoracostomy to accomplish an expansion thoracoplasty.
The Vertical Expansion Prosthetic Titanium Rib (VEPTR)implant is a sliding
titanium construct, roughly rectangular in crosssection with two standard
curvatures, both conforming to the shape of the thoracic cage into which
it is being implanted. The construct is placed vertically along the chest
wall by attaching each end to healthy ribs above and below the site of
abnormality (Figure 3). In addition
to distracting and expanding the chest wall, it may act as a protective
internal splint over areas where ribs are missing. The implanted VEPTR
device can also indirectly apply distraction to the spinal column, controlling
or improving spinal deformity.
As shown in figure 4, the VEPTR consists of the:
- superior cradle
- cradle end halves
- cradle locks
- rib sleeve
- inferior cradle, or lumbar extension
- distraction locks
- low profile lamina hook, or sacral ala hook and connector (if lumbar extension is used)
- 2. 37mm rod for the attachment of osteotomized ribs to the VEPTR device in patients with Hypoplastic Thorax Syndrome dependent upon whether or not a lumbar extension is used.
The superior and inferior sections of this device each consist of two pieces, a cradle and cradle end half. The semicircular end of the cradle can be adjusted to different angles (0 ¼, 30 ¼right, and 30 ¼left) to accommodate patient anatomy, and is connected to the cradle end half by a cradle lock to encase the rib. The cross-section of the proximal ends of the rib cradles is "T-shaped" for enhanced strength. The superior cradle and inferior cradle (or lumbar extension)attach to the rib sleeve by distraction locks. The rib sleeve is the central section of the construct. It serves as a track into which the cradles slide. The hole in the rib sleeve lines up with one of the blind holes on the rib cradle. The position of the inferior cradle assembly along the rib sleeve depends on the desired length of the overall rib prosthesis construct.
3.
1 IMPLANTATION AND ASSEMBLY
The superior cradle is placed over the patient's upper rib(s) and secured
together with a cradle lock, encasing the healthy rib(s). The rib sleeve
slides onto the proximal end of the superior cradle and is secured with
a distraction lock. The inferior cradle slides into the rib sleeve and
is positioned and secured on the lower healthy rib(s). The inferior cradle
is distracted to the desired length, and the rib sleeve and inferior cradle
are secured together with a distraction lock. In situations where scoliosis
extends into the lumbar spine, a lumbar extension can be used in place
of the inferior rib cradle and cradle end half. The distal portion of
the lumbar extension is a 6. 0mm straight rod that allows for attachment
to the lumbar spine with a low profile spinal hook. When attachment to
the lumbar lamina is not possible, a sacral ala hook is attached to the
lumbar extension with a connector, and the device is positioned on the
patient's sacrum.
4.
SURGICAL TECHNIQUE
Patient Positioning
The patient is placed in a lateral decubitus position with thorax and
preferably the entire arm prepped and draped free. Monitor leads for somatosensory
potentials are attached.
Exposure
The exposure is designed to allow access to the entire chest wall for
device placement and expansion opening wedge thoracostomy. Repeat exposures
for rod lengthening will be needed, and the incision must be planned with
this in mind. When a hybrid device is needed, a separate short midline
spinal incision is used for placement of the spinal hook. The "J"
shaped skin incision starts as proximally as needed in the interval between
scapula and spine, extends distally as far as needed and then curves gently
anteriorly. The medial flap of the skin incision is mobilized medially
to permit a more medial muscular incision. A laterally based flap of all
the muscles attached to the scapula is developed and retracted anteriorly
and laterally, exposing the bony chest wall. The proximal and distal extent
of this flap depends upon the location of planned thoracostomy and device
placement. Dissection should be extraperiosteal, preserving vascular supply
to the ribs and leaving intercostal muscles and vessels as intact as possible.
A medially based flap of paraspinal muscle is elevated to provide exposure
down to the transverse processes of the spine. Cephalad and caudad placement
sites for the superior and inferior rib cradles and cradle end halves
are chosen. The upper cradle should generally not involve the first rib,
nor pass anterior to the middle scalene muscle to avoid endangering the
brachial plexus and vascular supply to the arm. The lower cradle should
not end on unstable or "floating" ribs. When ribs are small
or hypoplastic, the cradles and cradle end halves should encompass two
ribs. Usually the device is placed as far posterior, close to the spine
as possible, expanding the chest and controlling typical lordo-scoliotic
deformity. More than one VEPTR device may be needed with devices placed
at approximately 4 cm intervals.
Cephlad
Implant Insertion
An incision approximately 1. 5 cm is made under the superior osseous rib
where the prosthesis is to be attached;the medial periosteum is carefully
elevated with a Freer elevator. The orientation of the first rib to the
rest of the thorax is used to determine the appropriate superior cradle
angulation required (30 degrees right, left or 0 degrees). The Cradle
Trial is used here to prepare the interval for the Superior Cradle. The
Superior Cradle is then threaded in the interval between the periosteum
and the osseous rib and then rotated into its longitudinal position. Next
the Cradle End Half is threaded over the top of the rib through the same
interval and snapped into the Superior Cradle using a Cradle Lock Forcep
loaded with a Cradle Lock to encase the rib.
Caudal
Implant Insertion
The procedure for implantation for the distal portion of the prosthesis
proceeds in the same manner. The longitudinal alignment of the device
should be chosen to obtain the best perpendicular orientation of attachment
to both the proximal and distal ribs. Either a neutral or 30 degree rotation
is available for alignment of the cradle construct in relationship to
the Rib Sleeve. If a Superior Cradle is required more anteriorly, it is
recommended that it be placed on a more inferior rib anteriorly so that
it is distal to the neurovascular bundle. Once all the Superior Cradles
are in place, they can be rotated around the osseous ribs away from the
chest wall defect for inspection of the underlying lung.
 |
|
| Figure 5. In this child with VACTERL, fused ribs resulted in progressive scoliosis which was treated with two opening wedge expansion thoracostomies of the concave hemithorax with primary lengthening by a chest wall distractor. |
Expansion
Thoracoplasty Techniques
Enlargement and lengthening of the constricted hemithorax and indirect
control of spinal curvature is achieved by one or multiple opening wedge
thoracostomies. If a congenital chest wall defect is present, the remaining
soft tissues may be incised in line with the ribs to allow an opening
wedge. If there are bony fusions of ribs, as commonly present with congenital
spinal anomalies and constricted hemithorax (Figures
5 and 6), fused ribs are separated with an oscillating saw, protecting
the underlying parietal pleura, and opening wedge thoracostomy produced
in the newly created interval between previously fused ribs. Where there
are multiple contiguous rib fusions, ribs may be divided into groups and
opening wedge thoracostomies performed between groups. Posteriorly the
thoracostomy must extend back to the transverse processes to permit expansion
between adjacent ribs. Confluent bony bars joining ribs medial to transverse
processes should be resected down to the vertebral column. Anteriorly,
the thoracostomy must extend to near the costal cartilage to permit free
expansion of the thoracostomy interval. The thoracostomy is spread slowly
to allow the intact parietal pleura to stretch. If the pleura is torn,
artificial pleura of Gore-Tex sheeting is placed loosely over the underlying
lung and sutured at the periphery of the thoracostomy to parietal pleura,
leaving enough material for present and future expansion. A chest tube
is placed in the chest cavity and brought through to the skin.
 |
 |
||
| Figure 6. Three-dimensional CT-reconstructions are shown demonstrating multiple fused ribs, and vertebral anomalies resulting in progressive scoliosis which was treated with a VEPTR (Figure 6A). Thorax expansion is evident in figure 6B after thoracoplasty and opening wedge thoracostomy of the concave hemithorax with primary lengthening by a chest wall distractor. | |||
Once the desired correction of the hemothorax deformity is achieved, the assembled VEPTR devices are implanted unexpanded, then tensioned 0. 5 cm to stabilize it. Excessive initial distraction may lead to premature cutout of the device, but correction and expansion are easiest to achieve at the initial procedure. Intubation and ventilatory support are typically required for several days postoperatively. Patients usually are hospitalized for 7 to 10 days. To accommodate later growth of the thorax, the devices are lengthened through 3cm incisions in out-patient surgery, two to three times a year. When the expandability of the device has been exhausted, they are replaced by surgery on an outpatient basis.
5.
INVESTIGATIONAL PROTOCOL
The titanium rib implant and the expansion thoracoplasty procedures made
possible by its use were developed by Campbell and coworkers 2
at Christus Santa Rosa Children's Hospital in San Antonio, TX. The devices
were first implanted in 1989. A subsequent FDA sponsored feasibility study
was conducted involving 33 patients;the safety and efficacy data collected
during this study has enabled the surgical technique and the study
methodology to evolve
as well as allowing important clinical endpoints to be more clearly defined.
These
 |
|
| Figure 7. The VEPTR implant and expansion thoracostomies were used bilaterally to enlarge a small thorax in a child with Jarcho-Levin syndrome. |
The multi-center protocol includes a regimented study methodology, which is designed to be nonrandomized. Participating centers include Christus Santa Rosa Children's Hospital in San Antonio, Boston Children's Hospital and Children's Hospital of Pittsburgh. Boston Children's Hospital and Children's Hospital of Pittsburgh have enrolled 10 patients to date. Pre-operative evaluation includes pulmonary and general surgical evaluation, 3-D CT scan and standardized thoracic measurements. Long-term follow-up data will be collected by evaluating all patients annually after the immediate two-year evaluation until the final enrolled patient has been followed for two years. During the follow-up period, expansion or replacement of components of the VEPTR will be necessary to accommodate the patient's growth, and/or to further correct spinal or thoracic deformity. Patients will serve as their own control in that efficacy parameters will be measured and analyzed post-operatively in comparison to baseline values.
5.
1 CURRENT INCLUSION CRITERIA
To be enrolled in the study, the patient must be six months of age or
older, up to skeletal maturity as defined by closure of the epiphyseal
plates of the long bones and fusion of the iliac apophysis to the underlying
iliac crest (Risser sign +5). The primary indication of Thoracic Insufficiency
Syndrome is clinically and radiographically defined as (1) Flail Chest
Syndrome (congenital chest wall defect, acquired surgical chest wall defect,
chest wall tumor resection, surgical separation of conjoined twins, traumatic
flail chest, (2) Congenital constrictive chest wall syndrome, (3) severe
rib fusion with progressive thoracic scoliosis without vertebral anomalies,
(4) moderate rib fusion with secondary chest wall constriction by progressive
thoracic congenital scoliosis (thoracogenic scoliosis) (5) hypoplastic
thorax syndromes (Jeune's syndrome, Achondroplasia, Ellis van Crevald
syndrome, Jarcho-Levine syndrome), (6) progressive spinal deformity (scoliosis/kyphosis)
in patients without rib anomaly in patients of age 10 years or younger,
(7) progressive thoracic congenital scoliosis with absence of rib fusion,
(8) progressive scoliosis of neurogenic or idiopathic origin, and (9)
primary progressive Thoracic Insufficiency Syndrome (progression of chest
wall malformation, or worsening pulmonary insufficiency).
5.
2 EXPECTED OUTCOMES
The goal of this prosthetically aided widening of the chest is to facilitate
lung growth and to ultimately counteract, prevent or reverse thoracic
insufficiency. Additional goals include stabilization of the spinal and
clinical deformity, preservation of thoracic spine growth potential, with
the overall objective being improvement of volume, symmetry and function
of the thorax, and maintenance of these improvements during growth
6.
CHILDREN'S HOSPITAL EXPERIENCE
The VEPTR device is currently being used investigationally to treat patients
with thoracic insufficiency syndrome. At Children's Hospital in Boston,
the majority of the nine patients who have received the VEPTR implant
were treated for congenital scoliosis or a short thorax (Table
1). Although follow up is currently limited, preliminary results
of the patients with thoracic insufficiency syndrome secondary to progressive
scoliosis enrolled at this institution seem to corroborate findings of
an earlier feasibility study. 30 All nine primary and both secondary patients
treated at Boston Children's Hospital underwent one or more expansion
opening wedge thoracostomies of the concave hemithorax with primary lengthening
by the VEPTR device with further secondary lengthening at 4 to 6-month
intervals. The current average thoracic spinal height increase is 0. 8
cm/year. Complications observed included device cutout through the rib,
which was managed by extending the device to the adjacent rib below, and
transient neurapraxia of the upper extremity. Two patients with severe
Jarcho-Levin syndrome for whom surgical treatment was planned died of
respiratory insufficiency while awaiting enough growth to permit expansion
thoracostomy and insertion of the smallest available VEPTR device (Table
1, case AL and case RJ ).
7.
CONCLUSIONS
Expansion thoracoplasty using the Vertical Expansion Prosthetic Titanium
Rib implant (VEPTR)as a chest wall distractor is currently being performed
at the Christus Santa Rosa Children's Hospital in San Antonio, Texas,
the Boston Children's Hospital and Children's Hospital in Pittsburgh.
An initial review of the procedure appears to indicate that VEPTR expansion
thoracoplasty is successful in directly treating segmental hemithorax
hypoplasia from fused ribs, addressing thoracic insufficiency syndrome
by lengthening and expanding the constricted hemithorax, indirectly correcting
scoliosis in the young child without the need for spine fusion, with probable
benefit to the underlying lung. Further study of the method and clinical
result will indicate how the VEPTR-system can be further materially improved.
Kai-Uwe Lewandrowski, MD is a Clinical Fellow in Orthopaedic Surgery at Harvard Medical School.
Robert Campbell, MD is an Assistant Professor in Orthopaedic Surgery at University of Texas Health Science Center at San Antonio, TX
John B. Emans, MD is an Associate Professor in Orthopaedic Surgery at Harvard Medical School.
Address correspondence to:
John Emans, MD
Department of Orthopaedic Surgery
The Children's Hospital
300 Longwood Avenue
Boston, MA 02115