BACKGROUND
For well over a century, adhesive capsulitis of the shoulder has remained
a complex disorder with variable clinical outcomes. In 1872, Duplay 1
described a condition he called peri-arthritis scapulo-humerale, and later
Codman 2
described this disorder as a frozen shoulder and stated adhesive capsulitis
of the shoulder remains "a class of cases which are difficult to
define, difficult to treat, and difficult to explain from the point of
pathology. "This remains true even today. It has been suggested that
the frozen shoulder is precipitated by degeneration of the supraspinatus
tendon and is associated with chronic inflammation of the subacromial
bursa and glenohumeral capsule. Furthermore, immunological pathogenesis
and chromosomal abnormalities of this condition have also been postulated.
Despite several theories and hypotheses, the pathogenesis and pathophysiology
of this disorder continues to be poorly understood.
Adhesive capsulitis of the shoulder is clinically described as having three phases:the freezing or painful stage, the frozen or progressive stiffness phase, and the thawing or resolution phase. Codman 2 stated that even the most protracted cases recover with or without treatment in approximately two years. However, other authors 3 have noted that this disorder may not be self-limited with long-term follow up revealing persistent loss of motion in many patients.
In 1995, we set out upon a comprehensive study to determine the prevalence of this disorder as well as the natural history of adhesive capsulitis of the shoulder. Furthermore, we evaluated the surgical outcome of those patients undergoing arthroscopic capsular release for refractory adhesive capsulitis of the shoulder. We are now in the early stages of evaluating the cellular biology of this orthopaedic unknown.
PREVALENCE
OF ADHESIVE CAPULITIS OF THE SHOULDER
Three hundred consecutive patients were studied prospectively at the Diabetes
Center and primary care practices at the Massachusetts General Hospital.
Patients completed a questionnaire and were examined by the same investigator
in order to minimize interobserver variability. Strict criteria were used
to determine the presence of a frozen shoulder.
The overall prevalence of adhesive capsulitis in the diabetic population and nondiabetic population was 12%and <1%, respectively. Separating the diabetic patients into type I and type II diabetics, prevalence was noted to be 16%and 7%, respectively. An increased prevalence of adhesive capsulitis was noted in female patients as well as those who had a longer duration of diabetes mellitus. However, after correction for duration of diabetes, no causation was noted between frozen shoulder and hemoglobin (Hb) A1c values. This was true despite not only the last known HbA1c value, but over the average HbA1c value when followed for a mean of four years. These findings support the hypothesis that adhesive capsulitis of the shoulder is associated with duration of diabetes but not associated with long-term glycemic control. There are several theories as to why diabetic patients are more prone to a frozen shoulder. We believe diabetes may affect fibroblastic proliferation and increased expression of cytokines, thereby making this disorder more likely in this select population.
 |
|
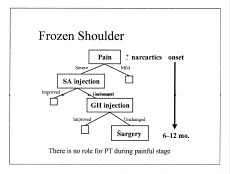
| Figure 1. Treatment protocol for adhesive capsulitis of the shoulder. |
NATURAL
HISTORY
The natural history of adhesive capsulitis remains variable. After reviewing
50 patients over a 10 year period, Rockwood and his colleagues 4
found "without exception, every patient regained a significant amount
of motion and returned to activities of daily living without pain. "In
contrast, Shaffer et al, 3
evaluated 62 patients and found that 30%of patients had measurable restriction
motion at an average of seven years follow up. This diversity in the literature
led us to embark on a prospective evaluation of the natural history of
this disorder in the general population. We have prospectively followed
well over 150 patients referred to our offices over the past five years.
Preliminary evaluation of these patients reveal 78%of patients were female
and the dominant arm was affected in 52%of patients. Complete resolution
of pain and return to full motion has been noted in the vast majority
of patients. However, diabetic patients have been reported to have poorer
outcomes when compared to the nondiabetic population. Our findings have
confirmed this as nearly 90%of nondiabetics were noted to have complete
resolution of this disorder compared to only 15%of diabetic patients.
Duration of symptoms were seen to typically last 12 to 18 months prior
to resolution of symptoms. Based on our preliminary findings, we have
proposed a treatment plan (Figure 1).
However, our study remains ongoing. We plan on completing this study when
200 patients have been enrolled with two-year minimal follow-up.
URGICAL
OUTCOMES
Over the past 5 years, we have been evaluating outcomes following arthroscopic
capsular release in the refractory frozen shoulder. Fifty-two patients
with idiopathic adhesive capsulitis of the shoulder have undergone arthroscopic
capsular release at the Massachusetts General Hospital. Patients have
been studied using the Constant and Murley 5
score system as well as the American Shoulder and Elbow Society Standarized
Shoulder Assessment and Shoulder Score Index. 6
 |
|
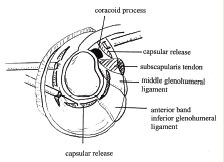
| Figure 2-A. Arthroscopic capsular release diagram. Note dual posterior portals for access to axillary recess for inferior capsular release. |
OPERATIVE
TECHNIQUE
After administration of anesthesia, gentle manipulation is performed by
for wardly flexing the arm slowly with gradually increasing force. Care
is taken to support the humerus just distal to the axilla. The manipulation
is often associated with an audible and palpable sensation of tissue rupture.
This process is then repeated with lateral elevation;however, internal
and external rotation often remains limited. Attempts of achieving increased
rotation may be performed, however, it is difficult to control the humerus
during this manipulation, and attempting to achieve such increased rotation
may be complicated by a fracture of the humerus.
An anterior and posterior portal is established in the usual fashion. An arthroscopic capsular release is then performed utilizing an electrocautery device. It is imperative that systemic muscle relaxants are not used by the anesthesiologist in order to be certain that if the release approximates the axillary nerve, the surgeon will see abrupt contraction of the deltoid muscle. The release begins at the middle glenohumeral ligament and continues inferiorly until external rotation with the arm at the side is noted to improve. Typically, the inferior glenohumeral ligament complex has been disrupted during the flexion component of the manipulation.
 |
|
| Figure 2-B. Arthroscopic photograph in lateral decubitus position. Note subscapularis muscle belly visible following anterior capsular release. |
If internal rotation remains limited, the arthroscope is then transferred to the anterior portal and utilizing the posterior portal as a working portal, a posterior capsular release is performed. Finally, if flexion remains limited, an inferior capsular release is performed through a second posterior portal, which is established one centimeter inferior to the initial portal (Figure 2). This gives excellent access to the axillary recess, although care must be taken to avoid injury to the axillary nerve during this portion of the release.
After release of the anterior and posterior structures, attention is then turned to the rotator interval. While visualizing the interval posteriorly, a rotator interval release is performed releasing all capsule in-between the subscapularis and the biceps tendon. Release extends superiorly to the anterior margin of the supraspinatus tendon. The coracoid process can be palpated just medial to the anterior arthroscopic portal. The coracohumeral ligament is divided by first dividing the rotator interval and then gently dividing all tissue lateral to the coracoid process as the electrocautery device is slowly brought from inside the joint towards the deltoid. Often the coracohumeral ligament is not identified as a discreet structure, however, dividing all tissues lateral to the coracoid process will release this ligament at its coracoid origin. Finally, if external rotation remains limited, one may consider releas-ing the intra-articular portion of the subscapularis tendon; however, caution should be taken to avoid excessive release of the subscapularis.
RESULTS
Pre-operative and post-operative results were compared using the paired
t -test. A regression analysis was used to evaluate any correlation between
length of follow-up and change in outcome. Preliminary findings with minimal
follow up at one year has revealed statistically significant improvement
in range of motion, pain, and objective shoulder scores following arthroscopic
capsular release. 7
We paid particular attention to the outcomes following the use of an indwelling
interscalene catheter. It has several theoretical advantages. It decreases
pain in the postoperative period thereby improving compliance with physical
therapy. Our findings have supported the use of an indwelling interscalene
catheter. We have found a significant improvement in the objective shoulder
scores system in those patients who underwent release following placement
of an interscalene catheter. We now are at the beginning stages of a prospective
randomized study evaluating the use of this catheter.
CELLULAR
BIOLOGY
The cellular biology and pathogenesis of adhesive capsulitis remains poorly
understood. Rodeo and colleagues 8
reported increased receptors for certain growth factors in those patients
with adhesive capsulitis. Similar findings have been noted by Bunker and
Anthony . 9
This prompted us to begin a study of the cellular biology of adhesive
capsulitis. Monoclonal antibodies will be used to localize cytokines in
the shoulder capsule of normal and frozen shoulder patients. We plan on
studying the presence and concentration of platelet-derived growth factor
(PDGF), basic fibroblast growth factor (bFGf), insulin-like growth factor
(IGF), as well as leucocyte common antigen, and macrophage/synovial antigen
in the shoulder capsules of these patients.
SUMMARY
We hope our research efforts will shed some light on this interesting
and often disabling disorder. Understanding the cellular biology of adhesive
capsulitis may have important treatment implications in the future.
Gary S. Perlmutter, MD is a Clinical Instructor in Orthopaedic Surgery, Harvard Medical School.
Kenneth Sabbagg, MD is a Clinical fellow in Orthopaedic Surgery, University of California at Los Angeles Medical Center, and a former resident, Harvard Combined Orthopaedic Residency Program.
William Apruzzese, BS, MPH is a research assistant, Massachusetts General Hospital.
Enrico Cagliero, MD is an Assistant Professor of Medicine, Harvard Medical School.
David M. Nathan, MD is a Professor of Medicine, Harvard Medical School.
Address correspondence to:
Gary S. Perlmutter, MD
Department of Orthopaedic Surgery
Massachusetts General Hospital
1 Hawthorne Place
Boston, MA 02114