INTRODUCTION
Percutaneous vertebroplasty is a procedure which augments a weakened vertebra
by injecting a substance through a percutaneous, fluoroscopically guided
needle placed into the vertebral body. The injected compound, typically
polymethylmethacrylate (PMMA) cement, restores some of the mechanical
properties of the vertebra, thereby helping to stabilize the spine and
relieve the patient of pain.
Growing clinical experience with vertebroplasty has increased our understanding of the proper indications and our awareness of the procedure's limitations and contraindications. Reported complications underscore the high level of risk associated with this procedure, and the technical aspects of vertebroplasty continue to be refined. The mechanism of action underlying vertebroplasty has been studied but remains under debate, despite basic science studies which have addressed this question.
We will review the procedure itself, as well as the clinical indications, and the basic science behind vertebroplasty. We will also describe current applications of the technique and clinical results, and suggest further areas of investigation to improve vertebroplasty and safely broaden its use.
 |
|
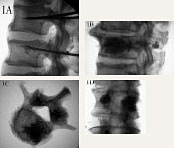
| Figure 1. A. Lateral fluoroscopic view showing transpedicular needle placement into the vertebral body (lower vertebra) . Lateral B. and axial C. views after unipedicular PMMA injection. D. AP view after bipedicular injection. |
INITIAL
DEVELOPMENT
Vertebroplasty was first developed in France, with preliminary reports
in 1987. 1
The earliest procedures were through an open surgical exposure. In these
first cases, vertebroplasty was used to treat benign, aggressive hemangiomata
which were destroying the vertebral body and producing pain secondary
to pathological microfracture or overt fracture. Shortly after ward, the
technique was developed percutaneously. 1,
2
Subsequently, vertebroplasty was used for pain relief or spinal stabilization of osteolytic tumor foci. Currently, the two most common conditions treated with vertebroplasty are osteoporotic compression fractures and spinal metastases. 3-5
PROCEDURE
Percutaneous vertebroplasty may be performed to augment weakened vertebrae
at the cervical level, though most clinical experience is in the thoracolumbar
region. The approach is anterolateral with the patient supine for a cervical
procedure, and posterolateral or transpedicular with the patient prone
for thoracolumber injections.
Sedation along with local anesthesia allow for intraprocedure monitoring of neurological status;alternatively, general anesthesia may be used. 6 Imaging consists of biplanar fluoroscopy 6 in most cases, and occasionally CT and fluoroscopy together. 5 A 10-12 gauge needle is used to enter the lumbar vertebral body under fluoroscopic guidance (12-13 ga. Ðthoracic spine, 15 ga. Ðcervical spine) . When needle position is satisfactory, the injectable compound (such as PMMA) is prepared and mixed with radio-opaque barium sulfate or tantalum powder to increase fluoroscopic visibility. Because of the high viscosity of PMMA, it is necessary to inject the material via several small (1-2 cc) syringes. The material is injected into the vertebral body, under continuous fluoroscopic monitoring. The lateral view is especially important because one risk of the procedure is leakage of cement into the spinal canal or neural foramina. Leakage may occur through venous channels, lytic posterior body wall lesions, or an iatrogenically perforated medial pedicle wall. Injection is stopped when cement reaches the posterior wall on a lateral view, or when it is seen to enter parts of the vertebral venous plexus, where venous embolism to the lungs is a theoretical concern. Deramond et al. 7 have described a second injection through the other pedicle if filling is <50 %on fluoroscopy (Figure 1) . Pre-procedure CT scanning helps to identify anatomical features predisposing to leakage, such as lytic cortical defects. Leakage through endplates into the disk space has been noted to be asymptomatic and inconsequential. 6-9 Leakage into the paravertebral soft tissues potentially threatens the femoral nerve in the lumbar region, and the intercostal nerves in the thoracic region.
Injection may be uni-or bi-pedicular, and typically up to 2-3 levels are treated in one session. After ward, the patient is positioned supine and observed carefully for 24 hours. Immediate post-procedure CT scan and plain films are reviewed for leakage. Common side effects include post-procedure fever, which is thought to be an inflammatory response to the cement, and is treated with non-steroidal medications. Transient exacerbation of pain, also thought to be mediated by inflammation, can also occur. New paresthesias or partial motor deficits on post-procedure exam are treated with steroids in the absence of obvious physical compression of the nerve roots or spinal cord by cement leakage. If any leakage associated with a neurological change or deficit is detected during or after the procedure, a stand-by orthopedic or neurosurgical team must be available to decompress the neural elements and remove the leaked cement. There have been a few reported instances of this serious complication. 8-10
Initial hospitalization averaged 4 days, 8 although this has decreased to 1-2 days. Patients are allowed to get out of bed and bear full weight the day after the procedure.
BASIC
SCIENCE
Although vertebroplasty has been used with good clinical effect, the underlying
basic science is poorly understood. One question concerns the mechanism
for pain relief. The pain in vertebral neoplasms is thought to be due
to irritation of nerve endings in the bone and compression of neural tissue
by mass effect. In addition, microfracture from weakening can cause pain
through stretch of these same nerve endings in osteoporotic vertebrae
or lytic tumoral lesion. The pain relief from injected PMMA has been attributed
to 1) thermal necrosis of nerve endings by the exothermic cement-curing
reaction, 2) toxic effect of the cement monomers on tumor cells, arresting
secretion of pain-mediating substances, and 3) stabilization of microfractures
and vertebral collapse. The exact role of each mechanism is unclear, 11
but the onset of pain relief observed clinically is rapid, usually in
2-3 days.
The volume of injected cement does not predict clinical effect. This early observation by Cotton et al. 9 based on post-procedure CT scans led to biomechanical studies of the relationship between volume of cement injected and strength. Dean et al. 12 have shown in human adult cadaveric lumbar vertebrae that the volume of cement injected does not correlate with strength as tested on a standard materials testing machine. Tohmeh et al. 13 showed in cadaveric osteoporotic vertebrae that unipedicular PMMA injection led to significantly increased vertebral strength over vertebra receiving no injection, and restored stiffness as effectively as bipedicular injection. This suggests that the pattern of cement distribution within the vertebral body matters just as much, if not more, than the total volume. 12, 13 So far cement distribution within the vertebra has not been studied carefully, and no prospective, randomized clinical study has compared universus bi-pedicular injection.
The materials used in vertebroplasty have also been studied. Disadvantages of using PMMA center around the potential catastrophic effects of thermal damage to the dural sac, cord, and nerve roots if leakage were to occur. Surgical evacuation of leaked cement in the spinal canal has been reported. 8, 10 The inability of PMMA to undergo remodeling, the inability to use it to deliver growth factors or chemotherapeutic agents, and the need to add radio-opaque agents and to lower viscosity (with unclear consequences on its long-term endurance) 14 are all additional concerns about this material in vertebroplasty.
Alternative injectable materials are being developed for use in vertebroplasty. Osteoconductive coral granules have been studied in human cadaveric vertebrae as well as in vivo in a sheep model. 15 Use of these granules led to increased bone formation and higher numbers of osteoblasts compared with control conditions. Such a material offers promise because it can act as a carrier for growth factors or cytokines. Dhert et al. 16 studied a bioresorbable calcium phosphate cement (Bonesource, Stryker-Howmedica) in a burst fracture model using human non-osteoporotic cadaveric vertebrae. They used an inflatable balloon (Inflatable Bone Tamp, Kyphon Inc. ) in a transpedicular route before cement injection to compress trabecular bone within the vertebral body and to create a cavity for the cement. The clear advantage of this technique is injection of cement under less pressure into a pre-formed cavity, decreasing the chance of leakage into the canal or neural foramina. Further work is needed to assess the biomechanical properties of bioresorbable cements in augmented vertebrae and in vivo performance. Finally, Belkoff et al. 17 studied a glass-ceramic bioactive composite material in a cadaver study. Orthocomp (Orthovita) restored more strength and restored original stiffness, significantly better results compared to Simplex P (Howmedica) and untreated levels. Advantages of this compound include greater natural radioopacity, and a lower temperature of setting than PMMA. Ongoing research is focused on developing optimal materials and on perfecting both delivery techniques and intraprocedure monitoring. Understanding the mechanism of action of vertebroplasty will allow us to refine the technique and better define the intra-procedure goals. These advances will improve clinical practice by reducing the time needed for the procedure, improving safety and reducing complications.
CLINICAL
EXPERIENCE
Clinical decision-making regarding the use of vertebroplasty has typically
involved a multidisciplinary team with input from a radiologist, orthopedic
surgeon, neurosurgeon, and (in the cases of tumors) an oncologist and
a radiation specialist. Most procedures to date have been performed by
neuroradiologists, with some orthopedists and neurosurgeons gaining experience
recently.
Indications for the procedure vary according to the underlying diagnosis. General contradications include uncorrectable coagulation disorders (because a large diameter needle is used) , and absence of a back-up orthopedic or neurosurgical team for emergent spinal decompression of cement leakage. Poor pulmonary status and difficulty lying prone are relative contraindications. Other considerations are specific to the condition being treated.
VERTEBRAL
HEMANGIOMA
The earliest cases of percutaneous vertebroplasty were for painful hemangioma
of the vertebral body, refractory to medical treatment. When radiographs
show aggressive hemangioma and there is pain but no neurologic signs,
vertebroplasty is combined with an injection of alcohol into the contralateral
part of the vertebra, to sclerose the hemangioma. When neurologic signs
are present, especially when an epidural mass is responsible, vertebroplasty
has been combined with same-day injection of N-butyl cyanoacrylate to
thrombose the hemangioma followed by next-day surgical laminectomy, hemangioma
resection from the epidural space, and fusion. 18
Small numbers of patients have been treated in each of these categories,
with no complications reported. 7,
8 In particular, 11 of 12 patients with vertebroplasty and alcohol
injection for radiographically aggressive hemangioma had lasting pain
relief. 7
SPINAL
TUMORS
Tumors of the spinal column most frequently involve the anterior elements,
effect an older population, and represent metastatic lesions. Treatment
options for these patients may be limited by comorbid medical conditions,
primary tumor burden elsewhere in the body, and nutritional deficiency;these
factors may make vertebrectomy and strut graft fusion through an anterior
approach unreasonably risky. Yet some treatment is still needed to offer
pain relief from pathologic fractures, and to achieve stabilization of
weakened vertebrae to prevent deformity from further collapse. Radiation
is a mainstay of treatment, but may have only a partial effect, and the
onset of pain relief is typically delayed by 2 weeks.
In this context, percutaneous vertebroplasty has been used for treatment of patients with painful, collapsing vertebrae due to metatstatic cancer or myeloma. It may suffice as an alternative to a large anterior procedure and offer adequate pain relief and stability. It may be combined with radiation or chemotherapy or both, and it is an attractive option for a recurrent metastatic focus when the radiation limit for the field has been reached. Specific indications include painful fracture refractory to medical management, and worsening collapse of a vertebral body. 6 Multifocal metastatic disease, in which vertebrectomy would not be curative, is a particularly appropriate indication.
Relative contraindications include loss of vertebral body height >60-65%, 6 though this is debated and may change as basic science investigation offers possibilities such as the inflatable bone tamp. Soft tissue extension of the vertebral metastasis, and cortical defects, especially of the posterior body wall, are also relative contraindications. 9
Good results have been reported in several series. 6-9 Two series 6, 7 have treated and followed 101 and 44 patients, with marked pain relief in 80%and 73%of cases, respectively. In the latter study, the pain relief and spinal stabilization persisted at an average follow-up of 7.1 months. The results in cases of vertebroplasty without accompanying radiation indicated that vertebroplasty is as effective as radiation, and in some ways more versatile. 6
 |
|
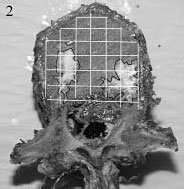
| Figure 2. PMMA (black outline) within a vertebral body cut open in the axial plane, with reference frame (white grid) superimposed. |
OSTEOPOROTIC
COMPRESSION FRACTURES
Vertebral compression fracture due to osteoporosis is a common problem,
with an estimated annual incidence of 500, 000 new patients in the U.
S. 19 Medical
advances aimed at slowing or arresting bone loss from aging have only
partially solved this problem, and the population effected is expected
to grow steadily as life expectancy increases. Traditional conservative
treatment for these fractures consists of nonsteroidal anti-inflammatory
agents and brief use of narcotic analgesics, a short period of immobilization,
followed by gradual mobilization, activity modification, and possibly
a spinal orthosis and physical therapy. This regimen is often successful
but has shortcomings:bedrest is fraught with complications in an elderly
population, including pulmonary compromise and decubitus ulcer formation.
Furthermore, pain relief is neither immediate nor a guaranteed outcome.
Consequently, percutaneous vertebroplasty has been used to treat osteoporotic
compression fractures, with a growing clinical experience suggesting considerable
pain relief, lasting for the duration of the limited follow-up of most
of these studies. 5,
7, 11, 19, 20 The initial indication for vertebroplasty in this condition
was pain of 4-5 weeks duration persisting despite conservative therapy.
Recently, vertebroplasty has been used more acutely after fracture in
older patients who have medical comorbidities that portend complications
due to immobilization.
Percutaneous vertebroplasty was performed for painful osteoporotic compression fractures in 16 patients in a prospective study by Cortet et al. 11 They noted significant changes in pain and function scores, with these improvements persisting at 6 month follow-up. A large French series with 80 patients reported pain relief in over 90%of patients, with immediate onset and prolonged effect. Follow-up is reported as 1 month to 10 years, but detailed analysis is not provided. 7 Jensen et al published the earliest clinical experience with vertebroplasty in the U. S. , treating 29 patients for 49 osteoporotic fractures. They reported pain relief in 26 patients (90%) within 24 hours, though long-term follow-up was unavailable. 20
Barr et al. 5 had similar results but longer follow-up and more precise pain and function grading, with 24 of 38 patients (63%) reporting marked improvement in pain and function, moderate relief in 12 of 38 (32%) , and no relief in 2 of 38 (5%) . Average follow-up was 18 months, and no recurrent collapse of the treated vertebra was noted. Of note, several patients developed new back pain in the same region as the treated vertebra;in one patient, an adjacent vertebra had sustained a compression fracture, which was then treated successfully. This finding underscores the need for long-term follow-up to define the natural history after treatment, specifically concerning changes at adjacent levels. 7, 20
OUR
RESEARCH
Using osteoporotic elderly human cadaveric spines, we have been studying
different injectable compounds, including special preparations of PMMA
cements with increased radioopacity and a degradable biological cement
(Biocement D, EBI, Parsippany, NJ) . By injecting known volumes of these
materials into vertebrae, we note the ease of injection and measure injection
pressures. We are also developing a quantitative system to describe the
distribution of filling by cutting open vertebrae in the axial plane,
dividing the cut surfaces into multiple sectors, and. noting which sectors
are filled with cement (Figure 2) .
This should allow for subsequent correlation between the pattern of filling
in injected vertebrae as assessed by pre-testing CT scanning and biomechanical
performance in compressive testing of these same vertebrae.
SUMMARY
Vertebroplasty has three main clinical uses:for painful or collapsing
vertebrae due to hemangioma, spinal metastases, or osteoporotic bone loss.
Pain relief is prompt (within 1-2 days) and durable, as assessed by current,
limited clinical follow-up. The most significant potential complication,
thermal or mechanical damage to neural tissue in the canal or foramina,
can be avoided by careful patient selection and proper technique.
Controversies abound regarding the technical details, basic science and clinical practice of vertebroplasty. Optimizing intra-procedure imaging and developing safer delivery systems are technical considerations remaining to be solved. Basic science investigation will address the importance of the pattern of cement distribution and will identify the best materials, whether PMMA or biodegradable preparations. An animal model may ultimately help solve the mechanism of action. Clinical questions concern the timing of treating osteoporotic fractures, and the long-term effects of treatment, especially at adjacent levels. Well-designed, randomized, propective trials with careful follow-up will allow us to address these questions methodically. As with any evolving technique, we expect more investigation in all of these areas to shape our understanding of vertebroplasty and to guide its use as an effective clinical tool.
Ajeya P. Joshi, MD is a Clinical Fellow in Orthopaedic Surgery at Harvard Medical School.
Paul A. Glazer, MD is a Clinical Instructor in Orthopaedic Surgery at Harvard Medical School.
Address correspondence to:
Paul A. Glazer, MD Department of Orthopaedic Surgery 330 Brookline Avenue Beth Israel Deaconess Medical Center Boston, MA 02114