|
|
|
| Click here to visit our web site |
| INTRODUCTION
Image-guided surgical navigation has the potential to improve the accuracy of critical aspects of orthopedic reconstructive surgery and to create new, less morbid procedures that are primarily based on image-guidance. The technology allows the surgeon to predict the effect of proposed surgical steps before they are made. The position of surgical instruments can be displayed in real-time on multiple radiographic projections simultaneously – an impossibility with traditional fluoroscopic techniques. The current review explains the basic principles of surgical navigation and its applications to orthopedic reconstructive surgery. PRINCIPLES OF SURGICAL NAVIGATION
TRACKING METHODS
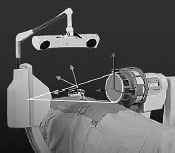
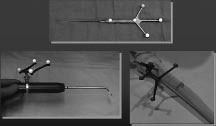
Optical tracking can be performed with the use of a stereoscopic infrared camera (Figure 1). Instruments and bones are tracked by rigidly attaching small frames on them with 3 or more spheres that reflect light or L. E. D. s that emit light (Figure 2). If the camera can see the reference frame, the position of the rest of the instrument or bone can be instantly calculated.
IMAGING METHODS The center of the hip can be calculated by moving the hip joint while the optical camera tracks the femoral skeletal reference frame. The center of rotation of the femoral reference frame is the center of rotation of the hip. The center of the distal femur is directly digitized with a pointer that has a reference frame attached to it. With the center of the hip and knee inputted, the mechanical axis of the femur is defined and can be tracked continuously during surgery. If a navigated saw or cutting jig is placed on the distal femur, the angle between that plane and the mechanical axis of the femur can be calculated. Using image-free techniques, all major angular and distance measurements can be tracked during total knee surgery. Image-based navigation systems have the ability to display surgical instruments onto a background of two- dimensional (2D) or three-dimensional (3D) images of the body. While all image-based navigation systems have the capability of tracking in an image-free mode, image-free navigation systems are more limited in their applications. Imaging for image-based navigation can be done either before or during surgery. PRE-OPERATIVE IMAGE ACQUISITION INTRA-OPERATIVE IMAGE ACQUISITION CLINICAL APPLICATIONS TO THE HIP AND KNEE
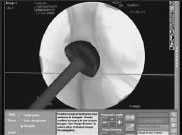
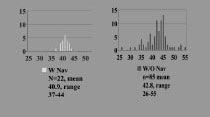
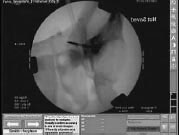
About the hip, surgical navigation techniques can be applied to primary and revision hip arthroplasty and osteotomy. For primary hip arthroplasty, navigation of acetabular component preparation and insertion is the greatest need, since acetabular component malposition is the cause of almost 50% of all hip dislocations. (1,2) Surgical navigation can track the position of acetabular reamers during the reaming process and the exact angle of acetabular component insertion (Figures 3 and 4). Our study of 22 primary total hip arthroplasties performed with surgical navigation clearly demonstrates that all poorly positioned cups are eliminated if navigation is used (Figure 5). Elimination of poorly positioned cups with the use of surgical navigation would decrease the incidence of dislocation, revision for dislocation, polyethylene wear, and osteolysis due to polyethylene wear. (2) These data suggest that patients undergoing total hip arthroplasty with image-guided surgery may be far better off. Application of surgical navigation to revision total hip arthroplasty has the further advantage that cement may be removed more rapidly and safely if the progress of high-speed burrs could be tracked from multiple fluoroscopic angles simultaneously. Better knowledge of the location of these instruments may both save time and decrease the risk of bone perforation. Osteotomy of the pelvis and femur can be aided by surgical navigation in a variety of ways. Intra-operative navigation of osteotomes and blade chisels (Figure 6) is clearly beneficial. Tracking
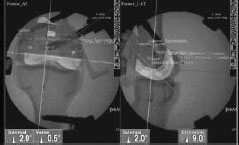
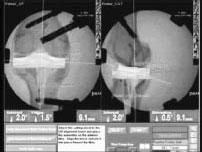
these instruments with virtual fluoroscopy would greatly decrease the need for obtaining additional images throughout the procedure. With regard to knee reconstruction, the keys to a successful total knee arthroplasty are proper alignment, ligament balance, and implant sizing. All of these can be performed with great accuracy using surgical navigation. One study of surgical navigation for total knee replacement has already shown that implant and limb alignment are more accurately achieved with navigation than without. (3) More sophisticated applications of surgical navigation for total knee replacement allow the surgeon to see bone resection depths, alignment, and the actual size and location of the proposed implants on virtual fluoroscopy before a single bone cut is made (Figures 7 and 8). (4) Other applications of image-guided surgery for the hip and knee include accurate placement of percutaneous SI joint screws, fracture reduction and rod insertion, interlocking screw insertion, removal of buried hardware, and ligament reconstruction.
CONCLUSION ACKNOWLEDGEMENTS Stephen B. Murphy, MD is a Clinical Instructor in Orthopaedic Surgery at Harvard Medical School. Reuben Gobezie, MD is a Resident in Orthopaedic Surgery in the Harvard Combined Orthopaedic Residency Program. Address correspondence to: |
|
Print Manuscript • View References • Download PDF version • Close window |