|
|
|
| Click here to visit our web site |
|
INTRODUCTION Tibial osteotomy had been a procedure routinely performed in patients with malalignment and unicompartmental disease over the age 50. The average age for tibial osteotomy in the Coventry series (1) was 63 years old. It would be difficult for a surgeon to do a tibial osteotomy at this age today because of the reproducible long-term results with modern total knee. In 1994 the Center for Disease Control and Prevention reported that by the year 2020 osteoarthritis will have the largest increase in numbers of new patients of any disease in the United States. (2) Approximately 60 million Americans referred to as “Baby Boomers” are at risk, representing 20% of the U. S. population. In particular, unicompartmental arthrosis is becoming more prevalent among patients in their 20’s, 30’s, and 40’s, particularly as baby boomers age and activity levels remain high because of their interest in sports. Previously, patients in this age group were not treated for their unicompartmental arthrosis. Unicompartmental and total knee arthroplasty can not offer these younger patients the high functional level of activity they desire. Sharma et al. have demonstrated that the risk of early radiographic progression of unicompartmental osteoarthritis with malalignment is 4 times more common in a varus knee and 5 times more common in a valgus knee than a neutrally aligned knee. (3) Osteoarthritis in the malaligned limb with unicompartmental disease remains a problem in the young athlete and adult. Tibial osteotomy remains the procedure of choice in the limb with unicompartmental osteoarthritis with malalignment. If we are to use tibial osteotomy in our treatment algorithm to help these young patients then it is important to avoid both technique-related problems and patient-related issues that have lead to the disfavor of tibial osteotomy as a treatment option. TECHNIQUE-RELATED ISSUES AGAINST HTO
PATIENT-RELATED ISSUES The author has found that these problems can be avoided or eliminated by appropriate osteotomy technique selection, patient selection, and careful pre- and post-operative planning and care. PROCEDURE SELECTION AND PLANNING The authors experience is similar; if the patient is relatively slim (i. e. ideal body weight less than 1. 32 times normal), a nonsmoker, highly motivated, and has unicompartmental medial disease with varus deformity, then he/she is a good candidate for an osteotomy. A range of motion arc of 90° or better is desired. Patellofemoral symptoms are accepted and may be dealt with by a concomitant tubercle osteotomy. Attention to a clinical varus thrust and baseline leg length discrepancy is also important. Preoperative radiographs include long axial alignment x-rays on 54” cassettes to include the hip, knee and talus standing in extension. Rosenberg (anteroposterior view of knee bent 45°), standing AP, lateral, and skyline films should also be performed. Radiograph measurement of leg length is also important. The mechanical axis is measured from the center of the femoral head to the center of the talus. If this line falls through the medial joint compartment with evidence of peripheral osteophyte formation, flattening of the articulation, subchondral bone sclerosis, and/or joint space narrowing, then the patient is a candidate for osteotomy surgery, provided that they do not have subluxation of the tibiofemoral joint or lateral symptoms. Lateral symptoms must be further investigated to rule out lateral compartment degenerative changes or meniscal tear. The desired angular correction is to place the mechanical axis through the center of or just to the lateral downslope of the lateral intercondylar spine. A simple angular correction as measured on the long axial standing films is a good practical guide. Pass a line from the center of the femoral head to the desired lateral intercondylar spine. A second line from the center of the talus then intersects this same point. The acute angle between the two is the angular correction desired. Ligamentous instability of the medial complex should be assessed; if there is medial laxity, this can be accounted for at the time of osteotomy to ensure that marked over correction does not occur. ALGORITHM
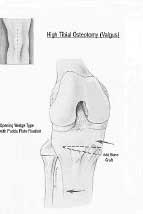
There are several companies that presently manufacture calibrated osteotomy jigs in 1 and 2 degree increments, allowing for very accurate and reproducible Coventry-type closing osteotomy corrections. A closing wedge osteotomy can generally be performed without elevation of the tibial tubercle up to 10° of angular correction. Removal of the medial portion of the fibular articular surface, leaving the proximal tib-fib joint capsule intact is preferred with corrections of 8° or less (figure 1a). It is difficult to accept corrections of 10° or greater without performing a mid-shaft fibular osteotomy; this allows for an easy closing osteotomy, without completely releasing the proximal tib-fib joint and rendering the lateral complex lax. For osteotomy corrections between 10° and 14°, the tibial tubercle is generally elevated and a retro-tubercular osteotomy is performed. This allows the osteotomy to be performed more distally on the tibia so as not to remove too much bone and produce a metaphyseal-diaphyseal mismatch (figures 1b,1c). This is typically performed with a concomitant mid-shaft fibular osteotomy. Fixation of both osteotomies is performed. If there is leg length shortening on the affected side, or if inferomedial joint line obliquity with a varus thrust exists, then an opening wedge osteotomy is performed (figure 2a). This is performed proximal to the pes anserinus insertion in an oblique fashion proximal to the tibial tubercle, directed towards the proximal tib-fib joint but not through the lateral cortex. Opening wedge osteotomies may correct up to approximately 15° before the medial hamstrings become too tight to allow further opening on the medial column of the knee (figures 2b,2c).
For corrections greater than or equal to 15° the author prefers a reversed dome osteotomy below the tibial tubercle with a mid shaft fibular osteotomy. This usually requires a blade plate fixation to allow a stable construct (figures 3a,3b,3c).
TECHNIQUE CLOSING WEDGE OSTEOTOMY If the angular correction is 8° or less, the calibrated jig is applied to the proximal tibial joint margins and a transverse cut is made to but not through the medial tibial cortex. The angled cut is then made to the medial cortex, with the knee in extension and the posterior neurovascular structures protected with sponges. If the desired correction is greater than or equal to 10°, a separate 4 cm incision is made between the superficial posterior and lateral muscular compartments at the level of the mid-shaft fibula, through the skin and the fascia only. Blunt finger dissection is performed to the posterolateral corner of the fibula, where the periosteum is sharply incised with a knife and a circumfrential subperiosteal dissection is then performed. Retractors are applied to the fibula. An oblique osteotomy is then made with a saggital saw, and the osteotomy is allowed slide on itself once the proximal tibial osteotomy is closed. After the tibial osteotomy is fixed, the fibular osteotomy is then plated with a 1/3 semi-tubular 4-hole plate. This allows comfort postoperatively and rapid union of the fibula. If the osteotomy of 10° or greater intersects the patellar tendon, then the tibial tubercle is osteotomized and elevated, leaving its distal aspect intact. The closing wedge osteotomy is then performed. The osteotomy closure is performed slowly with a compression device through an L-plate so as not to fracture and render unstable the medial cortex (the cortex is usually pre-drilled). The tubercle is fixed with one or two 3. 5 mm screws in compression mode through the posterior cortex. Usually, if there is some lateral patellar facet disease, a full thickness lateral release will be performed and the closing wedge bone graft is placed under the tibial tubercle in order to elevate it. The sponges are then removed and the tourniquet let down. Electrocautery is used for hemostasis, and two arms of a hemovac drain are placed in the wounds. One is placed posterior to the tibia, loosely re-approximating the iliotibial band to the superior aspect of the anterior lateral muscle compartment. The anterior aspect of the muscle fascia is left completely open. Closure of the subcutaneous tissues and skin follows. A second drain is placed in the wound flap outside of the muscle compartment. The drains are left in for 3 days postoperatively. During the first 48 hours, a continuos epidural pain management program is utilized and monitored by a 24-hour Pain Service. The muscle compartments are clinically inspected every 4-8 hours and as needed. VenodyneTM foot pumps are used immediately after surgery to diminish swelling and risk of deep venous thrombosis. They are the preferred mechnical compression device, as they improve venous return without imparting pressure on the muscle compartments. OPENING WEDGE OSTEOTOMY A longitudinal incision is made from the superior pole of the patella to the inferior aspect of the tibial tubercle. A full thickness medial subcutaneous flap is then made. The pes anserinus tendons are identified on the subcutaneous border of the tibia medially. The superior aspect of these tendons are then incised and the tendons are retracted. A transverse incision is made through the periosteum in the deep portion of the medial collateral ligament, from the posterior aspect of the tibia to the anterior aspect of the tibia, proximal to the pes insertion. The MCL is then subperiosteally dissected to within 1 cm of the joint line, leaving intact the deep and superficial aspects of the medial collateral ligament. The patella tendon is skeletonized on its insertion distally. With the knee flexed, the posterior aspect of the tibia is similarly dissected. Small wet sponges are packed behind the knee to the level of the lateral tib-fib joint and proximally to the level of the joint, and this is easily palpated. Under image intensification a guide wired is placed obliquely from the pes insertion proximally to the patella tendon insertion at the level of the proximal tibial-fibular joint. A guide is then placed over the top of this and an osteotomy is made with an oscillating saw under image intensification guidance to but not through the lateral cortex of the tibia. Opening wedge tines are then used to open the medial aspect of the tibia. The correct amount of angular correction is documented with an intraoperative guide wire assessment placing a Bovi TM cord from the center of the femoral head to the center of the talus, confirming that the mechanical axis falls through the lateral intercondylar spine. This will coincide with the desired degree of angular correction. Pudda plates are then placed (figure 2). 6.5 mm cancellous screws are used proximally through the plate; bicortical 4.5 mm screws are used distally. Tri-cortical iliac crest bone graft is used on the posterior, medial and anterior openings. Cancellous bone graft is packed deep within the osteotomy surfaces. A medium hemovac drain is then placed posterior to the tibia, and the soft tissues are placed over the plate and loosely repaired. Postoperative wound care and analgesic is as per closing wedge osteotomy. REVERSE DOME OSTEOTOMY The exposure is identical to that performed during a closing wedge valgus osteotomy. Prior to osteotomy, however, the chisel for the blade plate is placed 8-10o oblique to the tibiofemoral joint, which is usually a 15-20 mm offset from the tibia. After chisel placement, the reverse dome is made usually with a series of drill holes through a pre-made drill guide from anterior to posterior. The drill holes are connected with small 1/8” osteotomes, first on the anterior cortex, followed by the posterior cortex and then the mid-shaft fibular osteotomy. The blade plate is then placed and the angular correction is made under manual valgus force, distracting and re-approximating the tibial osteotomy. An articulated compression device is then used through the blade plate to provide compression to the osteotomy site and to obtain the angle of correction desired. Postoperative wound care and analgesia is similar to that for a high tibial closing wedge osteotomy. POSTOPERATIVE CARE CONCLUSION Tom Minas, MD is Director, Cartilage Repair Center, Brigham and Women’s Hospital and an Associate Professor, Harvard Medical School. Address correspondence
to: |
||||||||||||||||||||||||||||||
|
Print Manuscript • View References • Download PDF version • Close window |