Original Submissions
Current Issue: Volume 14 |  PDF
PDF
Inside the Value Revolution at Children’s Hospital Boston: Time-Driven Activity-Based Costing in Orthopaedic Surgery
Department of Orthopaedic Surgery, Children’s Hospital Boston, Boston, MA
Keywords: Operating Room Workflows, Safety Culture, Central Processing
PDF
Introduction
It is an exciting, and potentially turbulent time in the evolution of health care delivery in the United States. Despite decades of debate and piecemeal political reforms, the health care system remains inefficient in many ways and is becoming increasingly expensive. Increases in national health care expenditure continue to outpace inflation, exceeding 17% of the gross domestic product.1 Rising health care expenditures compromise both the economic stability of the United States and the treatment of the sick and injured. In addition, attempted regional and national health care reform has shouldered health care providers with further responsibility. The pressure is on providers to treat more patients, while offering better care at lower costs. “Better for less” is the demand. In this climate of change, physicians must educate themselves in the vocabulary of the epidemiological, political, ethical, and economic forces that influence the evolving health care economy, both to inform provider perspectives and to provide meaningful comment as reform progresses.
Based on the seminal work of Harvard Business School Professors Michael Porter and Robert Kaplan in value-based health care delivery,2-5 the Department of Orthopaedic Surgery at Children’s Hospital Boston has initiated a series of projects aimed at improving value in health care delivery - investigations specifically focused on reducing costs while maintaining or improving health outcomes.
Value in Healthcare Delivery
Value is a measurement of the relative quality and cost of a service or product. In health care, value should be measured in terms of patient health outcomes achieved per dollar spent to achieve those outcomes.3,5
Value = Health Outcomes / Cost
Health outcomes, as defined by Porter, do include patient satisfaction with health.6 Through value improvement, patients, payers, providers, suppliers, and the government can all benefit while strengthening the economic stability and sustainability of the U.S. health care system. Cost reduction without regard to outcomes are “dangerous and self-defeating, leading to false ‘savings’ and potentially limiting effective care.”3 In contrast, by giving due consideration to health outcomes, value improvement respects the integrity of patient care while achieving lasting, meaningful reductions in cost.
Practice Pattern Variation
The first project in our “value improvement” series was an investigation of single hospital variation in practice patterns. Providers today are often criticized for providing “too much” care – amassing “unnecessary” costs without improving patient health outcomes. In some instances, it is clear that too many tests are ordered, too many appointments are scheduled, and too many dollars are spent. Physicians may argue that patient health and safety are sufficient motivation for providing more care, but health economists counter that fee-for-service payment systems foster a culture of “excessive” care by reimbursing providers for volume of care rather than the quality of care delivered.7 Profligate malpractice litigation is also an acknowledged factor in incentivizing defensive medicine and care excesses.8
Our investigation examined practice pattern variations in the treatment of torus (or “buckle”) fractures of the pediatric distal radius (Figure 1). Multiple randomized, controlled trials have demonstrated that distal radius torus fractures can be safely and effectively managed with removable splinting or bandaging and home removal.9-13 In order to evaluate compliance with established treatment standards for distal radius torus fractures, our investigation sought to characterize the variation in practice patterns at a single tertiary-care institution, and determine costs associated with this variation. The study retrospectively reviewed medical records from a single calendar year, and defined excess medical care based on published recommendations by van Bosse et al and Farbman et al.14,15 The study found that there is great variability in management practices for torus fractures in children despite the inherent stability of the fracture pattern. These findings suggest there are opportunities to streamline care, thus reducing costs, saving patient and provider time, and reducing exposure to unnecessary radiation. The results of this investigation were presented at the 2012 Annual Meeting of the Pediatric Orthopaedic Society of North America.

A torus (or “buckle”) fracture of the pediatric distal radius resulting from a compressive load. There is costly variability in management practices for torus fractures in children despite the inherent stability of the fracture pattern.
All Rights Reserved. Permission For Use Required.Standardized Clinical Assessment and Management Plan (SCAMP)
To seize the opportunities for cost savings and value improvement due to practice pattern variations, the Department of Orthopaedic Surgery at Children’s Hospital Boston has also developed a Standardized Clinical Assessment and Management Plan (SCAMP) for pediatric distal radius fractures. A SCAMP is an algorithm based on best practices, designed to guide decisions made by physicians in the treatment of a specifically defined medical condition. Furthermore, a SCAMP facilitates identification of provider deviations from the treatment algorithm, to allow for appropriate modification and improvement of the plan over time (Figure 2). By standardizing best practice patterns, SCAMPs can help providers maximize value and prepare for financial success as the system evolves towards bundled payments. This transition in payment models has been a great concern among providers, especially since 2009 when the Massachusetts Special Commission on the Health Care Payment System recommended that the fee-for-service payment model be replaced with a bundled payment model with pay for performance measures.7 The SCAMP for pediatric distal radius fractures will be launched in 2012, and is expected to provide multiple opportunities for cost savings and value improvement.
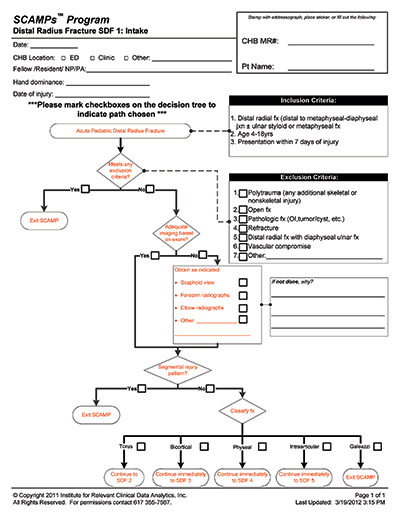
Example of an algorithm from a Standardized Clinical Assessment and Management Plan (SCAMP) developed for managing pediatric distal radius fractures at Children’s Hospital Boston. This algorithm depicts the initial care for bicortical distal radial fractures. Rectangles indicate services provided. Diamonds indicate decision points.
All Rights Reserved. Permission For Use Required.Measuring Value
The supporters of value-based health care acknowledge the fact that there are challenges in measuring both outcomes and cost.3,16 Historically, medical investigation has focused primarily on improving health outcomes, the numerator of the value equation. This research has resulted in tremendous advances in health care quality over the last 25 years. However, measurement of these advances is difficult, as health outcomes are defined by various standards according to the plethora of medical conditions and the multiple dimensions of each conditions. Outcomes must be risk-adjusted in order to be measured fairly, and the “full cycle of care” for many chronic illnesses may be indefinite. While important work on the numerator of the value equation should continue, physicians and researchers must take an equally rigorous approach to cost, the denominator, in order to improve value. The development of advanced medical treatments and assessments tends to progress more rapidly than our ability to understand fully which advances offer the highest value.
The measurement of costs is just as challenging. The system of health care delivery is complex, highly fragmented, and highly variable. Additionally, the involvement of third party payers (government and private health insurers) perverts incentives in ways that encourage ambiguity in cost data. Interestingly, however, recent designs to overhaul the health care payment system have brought to light an odd dichotomy between reimbursement and cost measurement – it seems their granularities are inversely proportional. It seems as payments become more broadly defined, costs must be measured more finely. Historically, payers have reimbursed providers for specific services rendered, but costs have been evaluated more generally at the level of the department, service, or support activity, rather than at the specific patient level. With recent efforts to bundle payments more broadly – either episodically (over a defined episode of care) or globally (over a defined time period of care) – providers are seeking more rigorous, patient level cost estimates. If patient outcomes and the costs of achieving those outcomes are not well-defined and measured, it will be impossible to evaluate the benefits or losses that result from system changes, or guide future decision making. This is not to say that resource costs are not currently measured specifically. For instance, the salary of a provider and the cost of supplies are readily available and indisputably accurate – but the cost of a provider or supplies per patient, per medical condition, or per outcome remains amorphous.
For example, many hospitals and physician organizations currently use a Ratio of Cost to Charge (RCC) approach to costing. The RCC is calculated by dividing the total costs for the year by the total annual charges for services rendered. The estimated cost of a service, such as a surgical procedure or an office visit, is then calculated by multiplying the charge for that service by the RCC. This methodology does allow hospitals or physician organizations to evaluate financial positions on the whole, but it does not allow evaluation of how much it costs to deliver care to a specific patient, or how those costs compare with health outcomes achieved for that patient. Another method in wide use is the Relative Value Unit (RVU) approach, which can theoretically generate refined cost estimates. RVUs are estimates of the relative time, complexity, and value of a service, used to more accurately allocate costs to individual procedures and activities. In theory, RVUs can accurately reflect real costs, but in practice allocation methodologies tend to be imprecise. This lack of granularity often leads to unintended cost distortions. It may be possible to improve cost estimates using RVUs with rigorous methodology.
With the purpose of determining the accuracy of current cost accounting techniques at Children’s Hospital Boston, a pilot study was initiated to evaluate the orthopaedic cast room. The investigation compared an alternative costing technique, Time-Driven Activity-Based Costing (TDABC) with the existing cost accounting system, which relies on less granular cost accounting techniques such as the aforementioned RCCs and RVUs. In the investigation, three types of casts were evaluated: long leg casts, Petrie long leg casts, and club foot casts. At the outset of the study, cast technicians and physicians both expected that the cost of a long leg Petrie cast would amount to roughly twice the cost of a single long leg cast, reflecting the time and complexity of Petrie cast application. However, according to the RCC and RVU methodologies currently utilized at Children’s Hospital Boston, a single long leg cast was estimated to have a higher cost than a Petrie cast. In contrast, the TDABC analysis produced cost estimates that made better intuitive sense: the estimated cost of a Petrie cast was roughly twice that of a single long leg cast (Figure 3). The findings of the cast room study provided evidence to support the hypothesis that cost estimates from current accounting methods often do not necessarily reflect the true costs of care (The application of TDABC in this investigation has been so successful that it is being adopted as a case study for use at the Harvard Business School and other business administration programs).
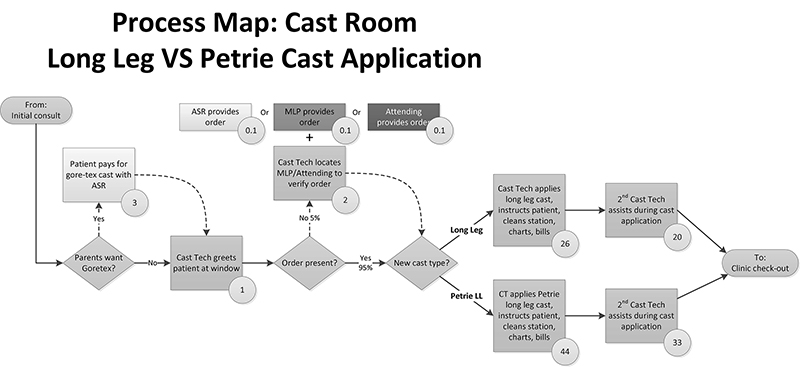
Example of a process map developed as part of the Time-Driven Activity-Based Costing project at Children’s Hospital Boston examining the costs of services in the orthopaedic cast room. This process map follows patients through cast application. Rectangles indicate care provided by specific medical personnel (physicians, midlevel providers, cast technicians, ambulatory service representatives, etc.). Diamonds indicate decision points. Circles indicate average time (in minutes) required for specific services. This map shows that the cast technician’s labor cost of a long leg cast is roughly half that of a Petrie long leg cast (46 minutes versus 77 minutes). In order to determine the full cost of this service, the time estimates illustrated in this process map must be multiplied by provider cost rates (inclusive of overhead and indirect costs), and added to direct costs such as casting supplies (see step 4 of TDABC). This map also illustrates the cost associated with a minor communication lapse (untimely completion of the cast order).
All Rights Reserved. Permission For Use Required.Explanation of TDABC
TDABC is a complicated name for a simple concept:
Total Cost = Cost Rate x Time
To carry out a TDABC analysis, the hourly cost rate of each resource that contributes to a specific patient’s care is multiplied by the amount of time each resource spends contributing to that patient’s care. The total cost of all contributing resources can then be summed in order to calculate the cost of treating a specific patient for a complete cycle of that patient’s care:
Total Cost = (Cost RateResource A x TimeResource A) + (Cost RateResource B x TimeResource B) + …
- 1. Define the medical condition of interest. For acute conditions, investigate all costs related to that condition from the beginning to the end of an episode of care. For chronic conditions, define the cycle of care as a period of time, such as a year.
- 2. Chart the principal activities involved in a patient’s care for the medical condition, along with the locations of those activities. Develop process maps of each activity in patient care delivery, documenting the various providers that directly interact with the patient.
- 3. Obtain time estimates for all interactions between health care providers and patients.
- 4. Estimate the cost of supplying patient care resources by estimating the direct costs of each resource involved in caring for patients. The direct costs include compensation for employees, depreciation or leasing of equipment, supplies, or other operating expenses. Also identify and attribute all the support (indirect) resources necessary to supply the primary resources providing patient care. These data are gathered from the general ledger, the budgeting system, and other IT systems.
- 5. Determine the practical capacity for each employee or resource (hours available for patient care).
- 6. Calculate the capacity cost rate for each employee or resource using data gathered in steps 4 and 5.
- 7. Calculate the total costs of providing care for a medical condition over the entire cycle of care. Begin by simply multiplying the capacity cost rates (including associated support costs) for each resource used in each patient process by the amounts of time the patient spent with the resource. Then, sum up all the costs across all the processes used during the patient’s complete cycle of care to produce the total cost of care for the patient.
When all processes have been mapped and measured in this way, they can be evaluated retrospectively, currently, and prospectively for respective inefficiencies and advantages. Costs that are higher than expected can be identified, and detailed data can easily be examined to understand cost drivers.
Further Applications of TDABC
In addition to the cast room study, The Department of Orthopaedic Surgery at Children’s Hospital Boston has initiated a detailed pilot study investigating the use of TDABC in pediatric distal radius fractures. With the assistance of the Harvard Business School, our department has served as one of the early pilot sites for investigative work in TDABC, along with the Department of Plastic Surgery at Children’s Hospital Boston (Boston, MA), the University of Texas MD Anderson Cancer Center (Houston, TX), and the Schon Klinik (Munich, Germany).
Throughout the progress of our pilot study with TDABC, we have experienced the many advantages that detailed cost estimates offer, including the identification of avoidable inefficiencies and cost distortions, the ability to perform prospective margin analyses of possible changes in care pathways, and insight for operational and strategic planning.
In our experience, the greatest concern with implementation of a TDABC system in a hospital or medical facility is the tremendous initial effort required to launch such a system. The fluid nature of medical care necessitates ongoing investment of time in maintaining a TDABC system as well. From our vantage, TDABC would benefit from a technology solution that seamlessly collects data on process flow, time stamping, and cost rates - thereby permitting efficient real time cost analysis and focus on value improvement.
Directly, TDABC is not expected to reduce costs or improve value – it is simply a tool that permits the accurate measurement of costs. The tree-sized weed that is the “health care cost crisis” in the garden of the American economy cannot be uprooted simply by trimming the leaves in distal radial fracture care or in the orthopaedic cast room. In both of these settings, costs are relatively low and patient outcomes are typically excellent. However, the fact that tremendous opportunities for value improvement exist in these simple settings suggests that the opportunities for capturing value in more complex and expensive conditions are potentially enormous. The largest drivers of health care costs include the overuse of new and expensive technology, defensive medicine practices due to potential malpractice litigation, and beginning-of-life/end-of-life care. If TDABC is found to be an effective tool for pruning the branches of excess cost, perhaps in the future it can be applied to cut roots.
Ultimately, the collection of more accurate cost and outcomes data will permit our society to abandon the current inefficient fee-for-service payment system, and move towards value-based reimbursement system, in which providers are reimbursed for creating value and not for providing services. A value-based reimbursement system will realign financial incentives with patient outcomes, driving costs down and quality up.
References