Original Submissions
Current Issue: Volume 14 |  PDF
PDF
Osteochondral Interpositional Allograft for Revision of a Malunited Olecranon Fracture, Olecranon Malunion Revision: A Case Report
1Investigation performed at aMassachusetts General Hospital, Boston, MA
Keywords: allograft, malunion, olecranon, osteochondral, osteotomy
PDF
Abstract
Comminuted olecranon fractures require careful restoration of the anatomic relationship of the ulnohumeral joint. Inadequate fixation results in malunion with painful and stiff elbow that can result in early osteoarthritis. Treatment options for olecranon malunions are limited with often-poor results. We present a case of olecranon malunion with both shortening of the coronoid-to-olecranon distance and a large depressed central articular surface that was reconstructed with corrective osteotomy and interposition of an osteochondral allograft.
Introduction
The anatomic relationship of the sigmoid notch of the olecranon to the humeral trochlea is fundamental to the stability and the motion of the elbow joint. Fixation of displaced olecranon fractures should take into account both the anatomic restoration of the articular surface as well as the restoration of the length between the coronoid to the olecranon. Inability to restore the length of the sigmoid notch has been cited as a factor leading to limitation of elbow function and increased joint contact pressures with early osteoarthritis.1-4 Small articular step-offs at the base of the olecranon are well tolerated, but failure to restore the large depressions in the articular surface and shortening of the sigmoid notch results in malunited fractures with poor outcomes.
When patients present with malunited fractures, surgical options include revision surgery, olecranon excision with triceps advancement, massive allograft reconstruction or a total elbow replacement. In a young patient, revision surgery is the only suitable initial option. Revision surgery with autologous and allografts are commonly advocated but literature on such methods is limited.5 Use of massive osteochondral allografts in the elbow has been used only as salvage procedures for reconstruction of the elbow published in limited cases.6-8 However, specific use of small osteochondral allograft contoured to restore the articular congruity and the length between the olecranon tip to the coronoid process has not been previously published.
We report a case of comminuted olecranon fracture that was initially treated with tension band wires. This fixation construct failed, and the patient developed a malunion with both shortening of the coronoid-olecranon interval and a large depressed central articular surface that led to a painful and stiff elbow. Revision surgery involved osteotomy of the olecranon and interposition of small fragment of fresh osteochondral allograft. Although use of osteochondral allografts have been previously reported for many different fracture types including the talus, tibial plateau, femoral head and humeral head and its use in elbow is not unique, use of small osteochondral allograft contoured specifically to restore articular congruity and length of the coronoid-olecranon interval has not been previously addressed in literature.
Case
A 30 year-old right-hand-dominant male truck driver fell off a trailer and sustained a comminuted right olecranon fracture. It was initially treated at an outside hospital with a tension band technique. The patient presented to our institution 8 months later with a complaint of motion block with inability to fully flex or extend the elbow. Examination of his left elbow revealed limited active and passive elbow motion with less than 100 degrees of functional arc of motion. He had painless full supination and pronation of his forearm. Radiographs of the elbow revealed a malunited olecranon with a large defect in the articular surface of the olecranon with a narrowed coronoid-to-olecranon interval (Figure 1). Examination under anesthesia revealed that the elbow was stable to varus and valgus stress but the elbow was catching prior to full flexion and extension at the humeroulnar articular contacts of the coronoid and the olecranon. Diagnostic elbow arthroscopy revealed grade II chondromalacia of the radial head and grade I to II chondromalacia of the capitellum. The trochlea showed grade I chondromalacia while the olecranon had a significant defect in the articular surface with interposed fibrous tissue.
Given the significant osteochondral defect and proximal ulna shortening, the patient underwent a transolecranon osteotomy. Using the posterior incision from the previous surgery, a chevron osteotomy was created distal to the previous fracture site to reflect the proximal ulna along with the articular step off. Fresh medial tibial osteochondral allograft was carefully selected and contoured to the shape of the articular defect of the greater sigmoid notch to restore the articular congruity. The appropriate length of the graft was determined by comparing the coronoid-to-olecranon distance of the unaffected elbow. Allograft trials were provisionally fixed with K-wires and the sigmoid notch was reduced to determine restoration of smooth arc of motion in flexion and extension. Once the appropriate osteochondral allograft was appropriately contoured, it was inserted and internally fixed with 3 Herbert screws to the proximal ulna applied from inside the joint to outside (Figure 2). The proximal ulna osteotomy was reduced and internally fixed using tension band technique. Intraoperatively, full smooth arc of elbow motion was achieved.
The fixation of osteochondral allograft 6 months later went into fibrous-type nonunion, so the tension band wires were replaced with a compression plate which provided a more stable construct with union noted in 1 year follow-up (Figure 3). Patient also regained 105° arc of motion from 10-115°.
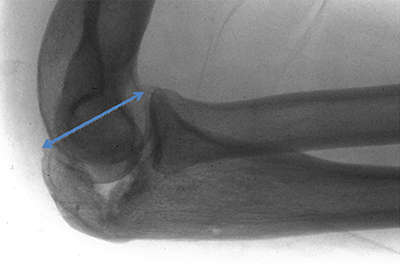 Lateral xray of the patient showing the olecranon malunion with a large osteochondral defect and shortened coronoid-to-olecranon interval (blue arrow)
Lateral xray of the patient showing the olecranon malunion with a large osteochondral defect and shortened coronoid-to-olecranon interval (blue arrow)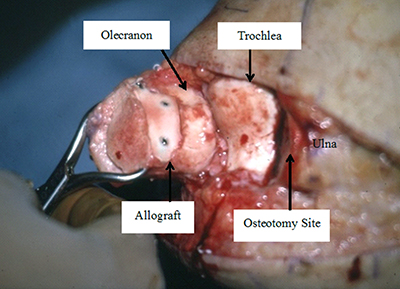 Intraoperative photograph: Proximal part of the sigmoid notch at the osteotomy site flipped 180-degrees showing the articular surface with tibial osteochondral allograft fixed with herbert screws
Intraoperative photograph: Proximal part of the sigmoid notch at the osteotomy site flipped 180-degrees showing the articular surface with tibial osteochondral allograft fixed with herbert screwsAll Rights Reserved. Permission For Use Required.
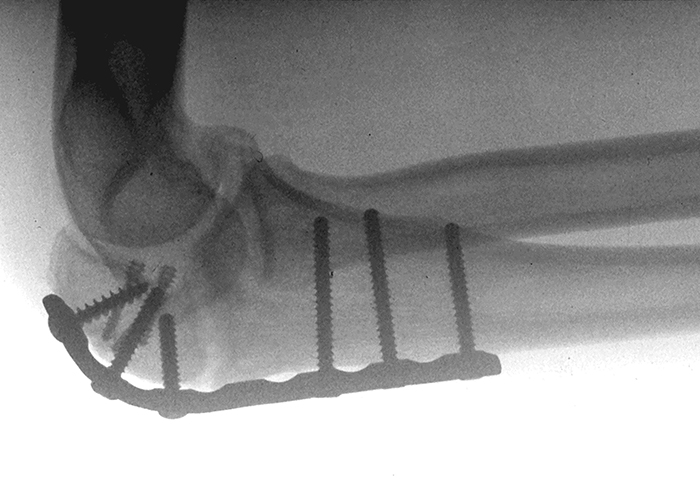
Postoperative lateral xray of the elbow revealing reconstruction construct with the osteochondral allograft
All Rights Reserved. Permission For Use Required.Discussion
Principles of intra-articular fracture fixation rely on restoration of the articular surface and stable fixation for early range of motion. Unique to the proximal ulna, the articular surface is a semilunar notch. The facets of the coronoid and proximal olecranon not only provide anterior and posterior elbow stability but they also serve as mechanical blocks at extremes of elbow flexion and extension.9 Hence, for comminuted olecranon fractures, the contour of the articular surface as well as the length of the greater sigmoid notch must be restored to provide smooth arc of motion and to prevent early osteoarthritis.2,3,10
Contemporary interests lie with attempts at restoration of the articular surface of the sigmoid notch with a variety of internal fixation techniques.11-15 Tension band fixation converts the distraction force of the triceps on the cortical surface of the olecranon to generate compression forces on the articular surface of the trochlear notch. If the articular surface opposite tension band fixation is comminuted, it will not resist the compression forces generated by this technique and collapse, resulting in shortened coronoid to olecranon interval as was the case with this patient.16 More stable fixation of comminuted olecranon fractures can be achieved with compression plate and screws supporting the cortical surface of the olecranon to maintain the sulcus distance of the greater sigmoid notch at the expense of small gaps in the articular surface. If the fractures are very comminuted, however, bone graft is necessary. The use of bone grafts to restore the articular surface of the greater sigmoid notch has been reported for olecranon fractures and nonunions.11-14,17,18 Schatzker advocated elevation of the joint depression much like tibial plateau fractures and bone-grafting the resultant defect.19 Bone grafts made of corticocancellous “bone plates” or bone plugs has also been used but these grafts are used to supplement as biology for healing and are not necessarily used as a structural graft for the purpose of interposition.
When malunion develops from inadequate initial fixation, reconstruction presents a major surgical challenge and literature on restoring these malunions are limited.5,7,8 Some papers support that a large portion of the greater sigmoid notch can be removed without sacrificing elbow motion and stability.20,21 Due to elevated joint pressures and humeroulnar joint constraints, current indications for olecranon excision have been limited to low-demand patients of 60 years or older with osteopenia and stable fractures requiring less than 50% olecranon excision.3,9,12 Excision of the comminuted portion of the olecranon and re-approximating a shortened trochlear notch have also been described.10,16 This method, however, causes further narrowing of the greater sigmoid notch and loss of motion.2 Alternatively, if the malunion results in enlargement of the coronoid-to-olecranon distance, computer-assisted CT modeling has been described to preoperatively determine the amount of bone excision required to restore normal anatomy of the sigmoid notch.22
Doornberg and Marti presented a case report utilizing iliac crest autograft as interpositional graft for an olecranon malunion.5 Because the base of the sigmoid notch is void of any articular cartilage this is a good option if the articular defect is small. If the initial fracture was severely comminuted, use of an osteochondral allograft may be a more suitable option with the possibility of fibrocartilage ingrowth and potential to avoid donor site morbidity with autograft harvesting.
In summary, we provide a technique for revising an olecranon malunion with large articular defect and shortening of the coronoid-to-olecranon interval. Use of an osteochondral allograft contoured to restore the articular step-off and re-establish appropriate length between the coronoid and the olecranon is a viable option for osteochondral defects that span beyond the bare area of the sigmoid notch and avoids the donor site morbidity associated with harvesting autografts. Careful preoperative planning is needed to identify the precise location of the osteotomy as well as the size and shape of the interposition bone graft.
References