Original Submissions
Current Issue: Volume 14 |  PDF
PDF
The “Almost Open” Calcaneus Fracture: Tips for Soft Tissue Management
Dept. of Orthopaedic Surgery, Massachusetts General Hospital, Boston, MA
PDF
Background
Open calcaneus fractures are relatively uncommon injuries with a reported incidence of 0.8% to 10% of calcaneus fractures. Most of these open lacerations, excluding injuries sustained from blast or gunshot wounds, are found on the medial hind foot. Given the high energy mechanism from which intra-articular calcaneus fractures are sustained and a relatively thin soft tissue envelope, open calcaneus fractures have significantly worse outcomes as compared to closed calcaneus fractures. The incidence of superficial and deep infection is increased and series in the literature have uniformly demonstrated poor outcomes. Case series have been published detailing management protocols for open calcaneus fractures which include urgent irrigation and debridement and various staged protocols involving temporary external/internal fixation with delayed definitive treatment.
The typical deformity in intra-articular calcaneus fractures is a depressed posterior facet with a shortened, widened tuberosity in varus angulation with comminution and expansion of the lateral wall. With increased severity, fracture lines propagate to the anterior calcaneus and can involve the calcaneal cuboid joint. There is little in the literature describing medial sided bony injury. The sustentaculum has long been believed to maintain anatomic position in these injuries, thus being termed the “constant” fragment. However, there is no evidence to support the notion that heel widening is solely due to lateral wall expansion and that the medial calcaneus, whether it be the sustentaculum or medial wall, maintains an anatomic position. Berberian, et al., in unpublished data, challenged the notion of the constancy of the sustentaculum fragment. They found a high percentage of displacement, angulation and fractures involving the sustentaculum in intra-articular calcaneus fractures. Given their findings and the lack of literature describing medial calcaneal bony injury, it is likely an important aspect of intra-articular calcaneus fractures especially given the observation that most open calcaneus fractures occur medially.
Soft tissue injuries fall along a spectrum and the simplified categorization of closed versus open fractures fails to take into account patients with significant medial soft tissue contusion without a clear open communication. As it regards to calcaneus fractures, studies have looked selectively at either open or closed injuries. Furthermore, much has been described about lateral wall expansion and subsequent issues with nonoperative treatment such as peroneal entrapment, subfibular impingement and shoe wear difficulties but little has been described about the effects of medial calcaneal wall bony expansion. There is no previous examination of the closed calcaneus fracture with significant medial soft tissue injury which we call the “almost open” calcaneus fracture. (Figure 1)

Medial Hindfoot
All Rights Reserved. Permission For Use Required.We report an illustrative case and tips for management of these injuries.
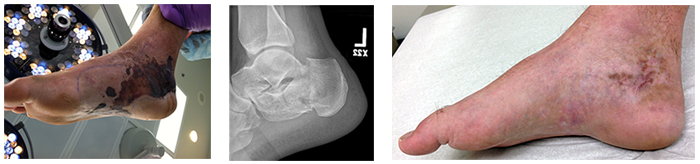
Patient RM is a 17 yo female who sustained bilateral closed calcaneus fractures after a fall from height. The right side was amenable to percutaneous fixation with little soft tissue injury and was fixed acutely. The left side demonstrated a Sanders 3/4 calcaneus fracture and given significant soft tissue injury was treated surgically in a delayed fashion.(Figure 2)
 All Rights Reserved. Permission For Use Required.
All Rights Reserved. Permission For Use Required.
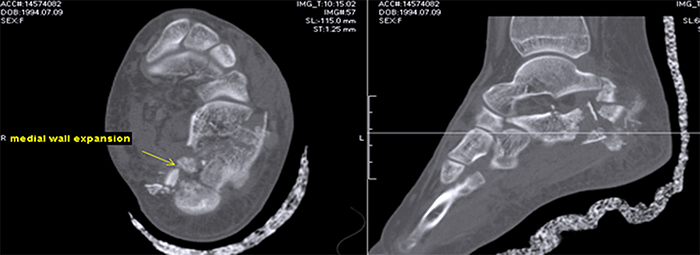
Preoperative CT demonstrated medial bony comminution
All Rights Reserved. Permission For Use Required.Physical examination at the time of surgery revealed a healed fracture blister on the medial hindfoot but not evidence of an open injury or full thickness contusion.
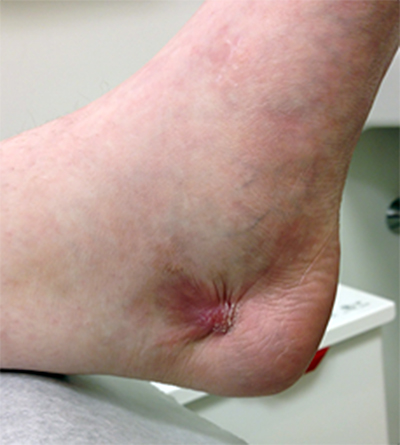
After successful open reduction internal fixation the patient was examined at her first postoperative visit 1 week later and was found to have full thickness ulceration medially. (Figure 4)
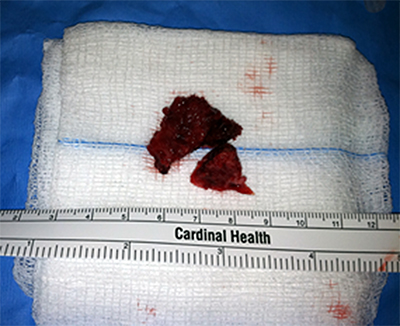
This was treated with urgent irrigation & debridement and removal of medial bony fragments and was successfully treated with prolonged negative pressure dressing therapy. (Figure 5)

Examples of significant medial soft tissue injury in closed calcaneus fractures are presented with resolution with careful soft tissue monitoring and management. (Figure 6A and 6B)
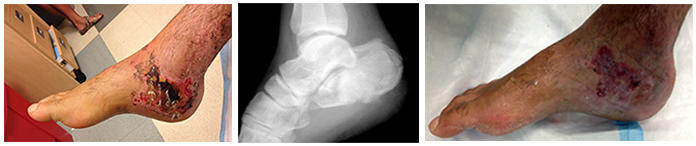 Figure 6B.
Figure 6B.
 All Rights Reserved. Permission For Use Required.
All Rights Reserved. Permission For Use Required.
Discussion
Several works in the published literature describe management protocols for open calcaneus fractures which include urgent irrigation and debridement and staged protocols with initial temporary stabilization and/or reduction of the tuber and delayed open reduction and internal fixation. Management of the “almost open” calcaneus fracture is similarly important to maximize outcomes and warrants special consideration.
Initial management entails careful examination of the hindfoot soft tissue envelope. While focus is often placed on the lateral soft-tissues, the medial hindfoot should be examined carefully as well for evidence of soft-tissue contusions, ecchymosis, skin threatening from displaced bony fragment and the presence of fracture blistering. These clinical signs may indicate a significant medial soft tissue injury. A careful neurovascular examination should be obtained. Given the intimacy of the tibial neurovascular bundle to the medial calcaneal wall, patients may present with plantar paresthesias or dysethesias. However this is not uncommon as the mechanism that produces calcaneus fractures can result in compression neuropraxias or contusion of the medial and lateral plantar nerves. In additional several works have demonstrated the association of tarsal tunnel syndrome in both acute calcaneus fractures as well as secondary to calcaneal malunion. Foot compartment syndrome should be assessed for. Foot compartment syndrome has previously been estimated to occur in 10% of calcaneus fractures although this has been challenged by recent literature which puts the estimate to be much lower.
Radiographic examination may give clues to the potential for evolving medial soft tissue injury not immediately apparent on initial clinical examination. The Harris axial heel view should be assessed for medial bony injury. As computed tomography scanning is often obtained when evaluating patients with intra-articular calcaneus fractures, careful attention should be paid to medial bony injury and displacement.
As operative calcaneus fractures (which are not amenable to percutaneous fixation or minimally invasive approaches) often require delayed definitive treatment, the injured extremity should be placed in a bulky Jones dressing with optional posterior plaster. Unless there is an associated ankle injury, a plaster “U” should not be placed as this may cause increased pressure along the medial and lateral soft tissues and offers no particular benefit. Patients may be similarly placed in a fracture boot which allows for more careful examination of the status of soft tissues but may not afford the compression and edema control that a Jones dressing does and may be poorly tolerated in the acute setting. While Thordarson and others demonstrated the effectiveness of foot pumps to reduce edema and resultant time to operative fixation for calcaneus fractures, this may not be the best management protocol for patients with significant medial soft tissue injury and a significantly contused soft tissue envelope.
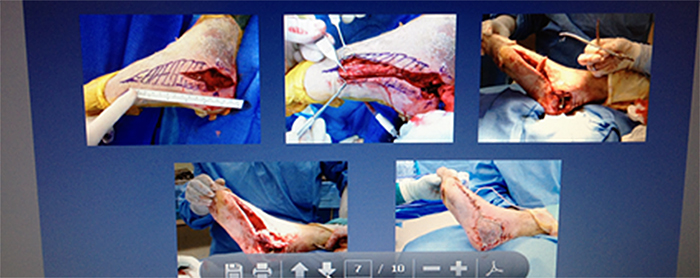
Patients with the “almost open” calcaneus fracture should be followed more closely than patients without significant medial soft-tissue injury both preoperatively and postoperatively. If the patient is discharged from the emergency ward they should be seen within 1 week not only for potential surgical planning but to monitor the soft-tissue envelope. Patients admitted to the hospital should have daily examination of soft tissues to assess not only for timing of definitive fixation but also for evolving medial soft tissue injury. Patients with evolving medial soft tissue injury should be managed accordingly. Full thickness necrosis should be aggressively and urgently debrided. The size of the defect determines whether this can be managed by negative pressure/vacuum assisted closure management or if plastics consultation is warranted for potential flap coverage or other grafting procedures. Recently Romash, et al described a pedicle transfer of the abductor hallucis muscle to address medial sided hindfoot soft tissue defects after calcaneus fracture. (Figure 7)
After calcaneus open reduction internal fixation patients are seen 1 week postoperatively to monitor not only the lateral incision but the medial soft tissues. This short term follow-up allows for early intervention should wound healing problems be noted. Patients are seen again 1 week later for suture removal.
 All Rights Reserved. Permission For Use Required.
All Rights Reserved. Permission For Use Required.
Conclusion
Medial soft tissue contusions in closed intra-articular calcaneus fractures require special consideration and management. A careful physical and radiographic examination at time of injury and careful post-injury follow-up is required to optimize outcomes.