
Original Submissions
Current Issue: Volume 15 |  PDF
PDF
Analysis of Medial Collateral Ligament Injuries of the Knee
Dania M. DeGrace, MD1, Thomas J. Gill IV, MD2, Thomas J. Gill III, MD3
Sports Medicine Service, Department of Orthopaedic Surgery, Massachusetts General Hospital, Harvard Medical School, Boston, MA 02114
PDF
Abstract: The medial collateral ligament (MCL) is the most commonly injured ligament of the knee. The typical mechanism is a valgus force on a flexed knee, but severe MCL injuries may be associated with other forces, particularly in high energy trauma and complex knee injury patterns. MCL injuries may occur as an isolated event or in the setting of multiligamentous, meniscal, and other associated knee pathology. Most MCL injuries are nonoperative and can be managed appropriately by primary care physicians or sports medicine specialists. A reasonable period of bracing and attention to the type of physical therapy utilized are essential for optimizing a rapid recovery and an excellent outcome. Most importantly, it is essential to rule out concomitant intra-articular pathology, particularly for higher grade injuries. An accurate history, a detailed physical exam, and appropriate imaging are necessary in all cases. Cruciate ligament rupture, meniscus tears, and osteochondral defects may require surgical intervention and should be rapidly detected. A literature review and our clinical experience support these basic principles.
Keywords: medial collateral ligament (MCL), medial knee injury, knee ligament injury, multiligament injury
Background
The medial collateral ligament (MCL) provides primary resistance to valgus forces at the knee in flexion. It is the principal static stabilizer of the medial side of the knee, and provides resistance to valgus stress as well as internal and external rotation.1,2 A cadaver study by Haimes et al. showed that sectioning of the superficial MCL caused significant increases in valgus angulation at 15, 30, 60, and 90 degrees of flexion but not in full extension.3 The MCL contributes to dynamic stability via its muscular attachments, including the pes anserinus, semimembranosus, and vastus medialis. The MCL also provides restraint to anterior tibial translation via attachment of the deep fibers of the MCL to the medial meniscus, which appear to stabilize the posterior horn, particularly in the setting of an anterior cruciate ligament (ACL)-deficient knee.2,4
The posteromedial corner consists of the anatomic structures between the posterior border of the MCL and the medial border of the posterior cruciate ligament (PCL). The posteromedial corner is comprised of the posterior oblique ligament (POL), expansions of the semimembranosus, oblique popliteal ligament, and posterior horn of the medial meniscus.5-7 This complex is a primary stabilizer of the extended knee and is the primary restraint to valgus stress and internal rotation in full extension.2,7 Haimes et al. demonstrated that transection of structures within the posteromedial corner in addition to the MCL significantly increased both valgus angulation and external rotation at all flexion angles.3
The MCL is also the most commonly injured ligament of the knee.8 The typical mechanism is a valgus force on a flexed knee, but severe MCL injuries may be associated with other forces, particularly in high energy trauma and in complex knee injury patterns. MCL injuries may occur as an isolated event or in the setting of multiligamentous, meniscal, and other associated knee pathology.
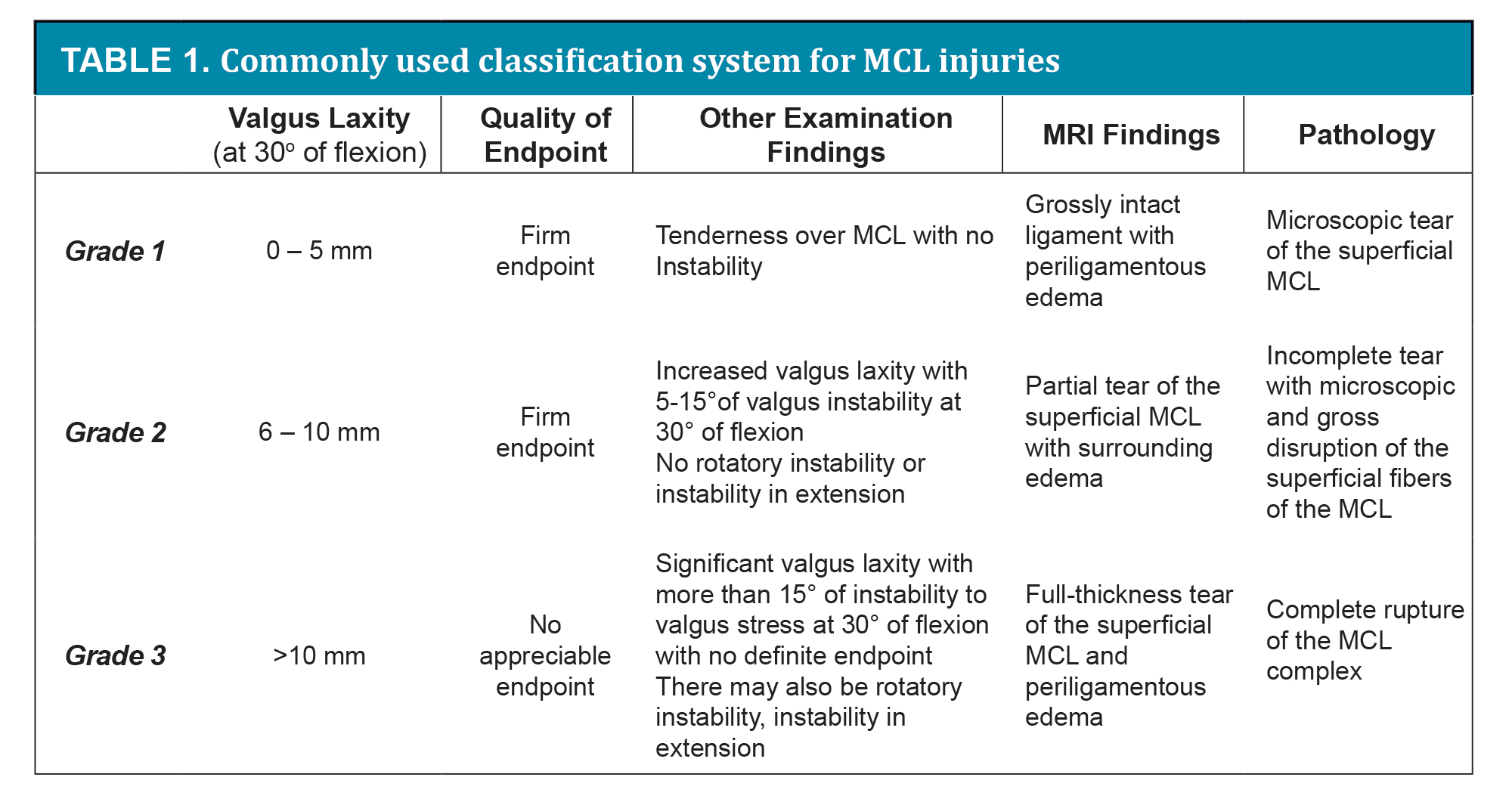
MCL injuries are classified clinically by grade, which refers to the amount of joint line opening with a valgus force, and by degree, which refers to the quality of the endpoint when laxity exists. According to the American Medical Association, clinical grade is evaluated with a valgus force at 30 degrees of flexion.9 A grade 1 sprain is defined as 0-5mm valgus laxity which corresponds to stretching and minor tearing of the MCL. This correlates with the definition of a first-degree sprain, where there is tenderness over the MCL but no instability. A grade 2 sprain is defined as 6-10mm valgus laxity on exam which corresponds to a significant partial tear of the MCL. This correlates with the definition of a second-degree sprain where there is increased valgus laxity with a firm endpoint. A grade 3 injury is defined as greater than 10mm of joint line opening which corresponds to a complete rupture of the MCL. This correlates with the definition of a third-degree injury where there is significant laxity with no appreciable endpoint.9,10 (Table 1)
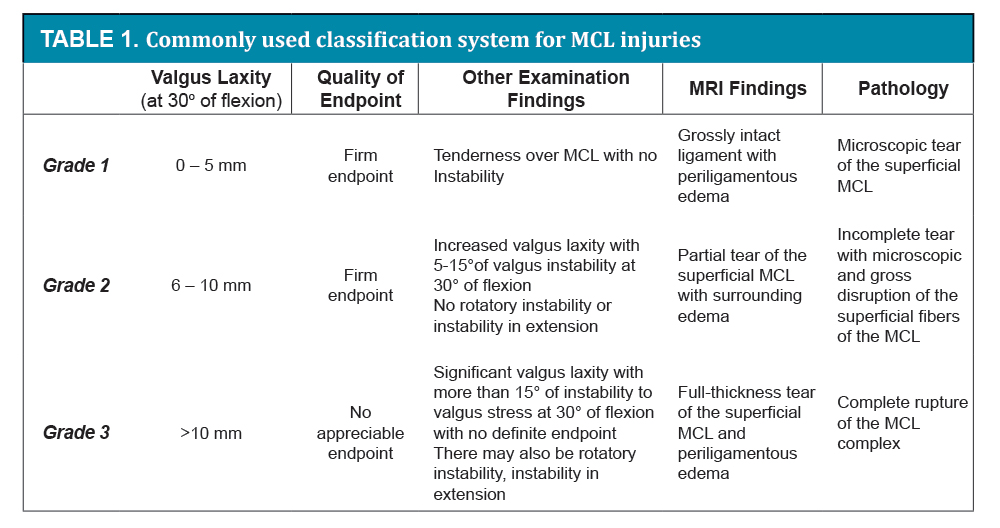
There are several classification systems for MCL injuries which use a combination of clinical valgus laxity, quality of endpoint, and MRI findings to describe the severity of injury. There is no standardized method of classification but most surgeons use a system that combines these elements to describe the injury. The most commonly used system defines a grade 1 injury as a microscopic tear of the superficial MCL, with no instability or laxity to valgus stress, and a grossly intact ligament on MRI scan with periligamentous edema.2,10,11 A grade 2 injury is an incomplete tear with both microscopic and gross disruption of the superficial fibers of the MCL. This causes 5-15 degrees of valgus instability at 30 degrees of flexion, but no rotatory instability or instability in extension. A grade 2 injury is characterized by a firm endpoint, and MRI scan demonstrates a partial tear of the superficial MCL with surrounding edema. A grade 3 injury refers to a complete tear of the MCL complex with more than 15 degrees of instability to valgus stress at 30 degrees of flexion with no definite endpoint. There may also be rotatory instability and instability in extension. MRI scan demonstrates a full-thickness tear of the superficial MCL and periligamentous edema.2,10,11 (Table 1).
With a severe MCL injury, damage to other anatomic structures must be considered. The likelihood of damage to other ligaments increases with the grade of the MCL injury. According to Fetto and Marshall, in a study of 265 patients, the risk of having a concomitant ligament injury was 20% with a grade 1 MCL injury, 53% with a grade 2 MCL injury, and 78% with a grade 3 MCL injury.8 The most common pattern of combined injury involves the MCL and ACL, comprising 7-8% of all ligamentous knee injuries5,12 and 70% of all multiligamentous knee injuries.13 Most studies agree that the second most common combination involves the MCL and PCL, comprising approximately 1% of all ligamentous knee injuries5,12 though a large study by Kaeding et al.13 found this pattern to be the least common, comprising 0.4% of all multiligamentous injuries.
The most worrisome is a multiligamentous injury involving the MCL plus two or three additional ligaments (ACL, PCL, and LCL in any combination), often associated with a history of knee dislocation. In general, traumatic knee dislocations are uncommon, accounting for <0.02% of all orthopaedic injuries, but since they often spontaneously reduce before initial evaluation, the true incidence is unknown.14 According to Kaeding et al.,13 the ACL/PCL/MCL combination comprises 4.2% and the ACL/PCL/LCL/MCL combination comprises 1.1% of all multiligamentous knee injuries. Dislocation commonly involves injury to multiple ligaments of the knee, resulting in multidirectional instability. Associated meniscal, osteochondral, and neurovascular injuries are often present and can complicate management.14-16
Rotatory instability, a positive dial test or a positive Swain test, and valgus laxity in full extension are indicative of injury to the posteromedial corner and should increase suspicion of injury to the cruciate ligaments as well.3,6 Combined MCL and posteromedial corner injuries may be more prevalent than previously thought. Sims et al.6 performed a retrospective cohort study evaluating operative isolated and combined medial-sided knee injuries in 93 patients. They found that 99% of patients had an injury to the posterior oblique ligament, 70% had an injury of the semimembranosus capsular attachment, and 30% had complete peripheral detachment of the meniscus.
Halinen et al.17 demonstrated that in multiligamentous knee injuries involving ACL rupture and grade 3 MCL injury, nonoperative and early operative treatment of the MCL injury with early ACL reconstruction yielded similar results at two year followup. Postoperative management included utilization of a brace at all times for 6 weeks followed by an additional 2 weeks during the day. Nonoperative management of the MCL with concomitant reconstruction of the ACL has demonstrated good results in the short term, but there is continued concern that an incompetent MCL can reduce the mechanical strength of the ACL graft leading to premature rupture.17-20
Acute reconstruction of the ACL (within 3 weeks of injury) initially appeared to have a greater risk of arthrofibrosis and decreased postoperative range of motion, particularly if the MCL was also reconstructed at the same time.21,22 Petersen et al.23 studied patients with combined ACL and MCL injuries where the MCL was treated nonoperatively. Early ACL reconstruction (within three weeks of injury) was followed by postoperative brace treatment for 6 weeks. Late ACL reconstruction (after a minimum of 10 weeks) was preceded by 6 weeks of brace treatment followed by a period of accelerated rehabilitation. Patients with late ACL reconstruction had better postoperative range of motion resulting in a lower rate of repeat arthroscopy for loss of extension: 4/27 patients or 15% of the early reconstructions and 1/37 patients or 3% of the late reconstructions required arthroscopy for stiffness. More recently Halinen et al.24 studied a group of 47 patients with complete ACL and MCL ruptures. Subjects were randomized to early ACL reconstruction with MCL repair or early ACL reconstruction and nonoperative management of the MCL. They found that all patients achieved full knee extension. Nonoperative treatment of the torn MCL allowed faster restoration of flexion and quadriceps muscle power, but at 52 weeks there was no significant difference in outcomes between patients treated operatively and nonoperatively for the MCL.
For patients requiring surgery it is also essential to address meniscal tears, osteochondral defects, and other intra-articular pathology, particularly in multiligamentous knee injuries. Associated intra-articular injuries have an increasing prevalence in multiligamentous knee injuries, high grade MCL lesions, and chronic MCL injuries. A persistent effusion in the setting of a suspected isolated MCL injury should raise concern for intra-articular injury.25 Miller et al.11 reported that the prevalence of trabecular microfractures was 45% in a cohort of 65 patients with isolated grade 2 or grade 3 MCL injuries. These were primarily located on the lateral femoral condyle or lateral tibial plateau, and completely resolved within two to four months after injury in all cases.
A large study by Kaeding et al.13 analyzed the pattern of intra-articular chondral and meniscal damage in subjects with multiligament knee injuries undergoing surgery. Data from 2,265 subjects showed that the ACL/MCL injury pattern was the most common, comprising 70% of all multiligament injuries. Lateral meniscal damage was significantly greater and medial meniscal damage was significantly less in this group as compared to the group with ACL injury only. There was no significant difference in medial or lateral meniscal damage in the ACL/PCL/MCL or ACL/PCL/LCL/MCL groups as compared to the group with ACL injury only. Taken together, multiligament knee injuries had a 30% incidence of medial meniscus injury for patients who underwent surgery less than 12 months after injury, and 64% for patients who underwent surgery more than 12 months after injury. The incidence of lateral meniscus injury was similar between groups. These findings paralleled the findings in the group with ACL injury only. Articular damage to the medial tibial plateau was significantly lower in the ACL/MCL group, and all other multiligament injury patterns showed chondral damage similar to the group with ACL injury only. Taken together, multiligament knee injuries that underwent knee reconstruction before 12 months had significantly less chondral damage on all surfaces compared with those who underwent knee reconstruction after 12 months. Overall, ligament injuries repaired acutely had significantly less articular and medial meniscal damage than repairs performed in a delayed fashion.
The correlation between knee ligament insufficiency, timing of reconstruction, and degenerative changes has been clearly shown in studies with isolated ACL injuries.26-29 A study by Kennedy et al.30 evaluated a series of 300 athletic patients under 40 years old with isolated ACL injuries. The researchers divided them into groups based on time from initial injury to ACL reconstruction. They found that the incidence of articular cartilage degeneration was significantly higher in patients who had surgery more than 6 months after injury (odds ratio = 4). In addition, the greatest severity of articular cartilage degeneration was found in the group that had the longest delay to surgery (>18 months). Likewise, there was a significantly higher incidence of medial meniscal tears in patients who underwent ACL reconstruction more than 12 months after injury (odds ratio = 8), but the odds of having a lateral meniscus tear did not change significantly with increasing time to surgery. Overall, acute ACL reconstruction with meniscal preservation has been shown to achieve the lowest incidence of degenerative change.26,27
The literature suggests that low grade MCL injuries are common, and that relatively few high grade isolated and combined multiligamentous MCL injuries ultimately require surgery. Evidence-based guidelines indicate that isolated MCL grade 1 and grade 2 injuries can be treated nonoperatively. Isolated grade 3 (complete disruption) MCL injuries have also been successfully treated nonoperatively in many series, including in elite athletes.31,32 Most MCL injuries are managed conservatively with bracing, physical therapy, and guarded return to activities. These are often appropriately treated by primary care physicians or sports medicine specialists. However, consideration may be given to operative management of grade 3 injuries in certain situations:
- • Multiligamentous knee injury
- • Chronic symptomatic valgus instability
- • Pellegrini-Stieda lesion where ossification of the femoral attachment of the MCL with associated pain and restricted movements may require excision of the bony lesion and reconstruction of the MCL.33,34
- • Stener-type lesion where the distal MCL is torn and the pes anserinus tendons become interposed between the MCL and the tibia, interfering with healing
In the setting of a multiligamentous knee injury, controversy exists with respect to operative stabilization or conservative management of the concomitant MCL injury. Patients likely prefer a knee that is mildly lax but functional with full range of motion as opposed to a stiff, painful, stable knee.12 In the multiligament-injured knee, a well-accepted approach based on that described by Indelicato for ACL/MCL injuries is often utilized.2,25 This protocol involves physical therapy for several weeks, which provides time for the MCL to heal and allows the patient to regain full knee range of motion. Once the preoperative rehabilitation is complete, the patient undergoes operative reconstruction of the cruciate ligaments. After cruciate reconstruction, the MCL is tested at 0 and 30 degrees of flexion intraoperatively. If significant laxity to valgus stress is observed as compared to the contralateral side, the MCL is surgically addressed. Indications for choosing either repair or reconstruction of the MCL and options for surgical technique are variables which seem to affect outcome but for which there is no consensus.
Physical therapy is another area of high importance for optimum outcome of both nonoperative and operative MCL injuries.14 Early mobilization is an important principle of both operative and nonoperative treatment. In a study performed on dogs, transection of the superficial MCL was performed and subjects were separated into three treatment groups including early motion, immobilization for 3 weeks, or immobilization for 6 weeks. Early motion resulted in enhanced healing and improved biomechanical properties of the superficial MCL.35 Mobilization after ligament injury improves the longitudinal alignment and concentration of cells and collagen and increases the ultimate load of the healing tissue.2,36,37 In addition, early knee motion appears to be protective against damage to articular cartilage and degenerative changes of the joint.38
For postoperative rehabilitation of multiligamentous knee injuries, physical therapy is tailored towards optimizing healing of the cruciate ligaments. A hinged knee brace that provides stability in the coronal plane but allows full knee range of motion is often used to protect the MCL without immobilizing the knee.
Giannotti et al.39 published guidelines for a functional rehabilitation program after isolated grade 3 MCL injuries. They state that “good to excellent results can be expected with a return to full preinjury activity level being the norm.” A simple hinged knee brace is used initially to protect the knee from valgus stress. Depending on the activity, bracing may be continued until the patient feels stable and safe playing without it. The protocol outlines four phases covering a time span of 10-12 weeks. During phase 1 (0-4 weeks), goals are to decrease swelling, restore knee range of motion from 0-100 degrees, gain 4/5 quadriceps and hamstring strength, restore a normal gait pattern, and restore full-weight-bearing status. Treatment during phase 1 includes cryotherapy, electrical muscle stimulation, stretching, range of motion exercises, and quadriceps and hamstring strengthening. During phase 2 (4-6 weeks), goals are to continue to control swelling, restore full knee range of motion from 0-140 degrees, and gain 5/5 quadriceps and hamstring strength. Treatment during phase 2 includes cryotherapy, closed chain exercises, and static proprioceptive exercises. During phase 3 (6-10 weeks) goals are to regain the ability to perform squats, return to light jogging and agility skills, and possibly progress to sport-specific skills and competition. Treatment during phase 3 includes treadmill jogging, dynamic proprioceptive exercises, slide board training and rebounder training. During phase 4 (8-12 weeks) goals are to attain 95% quadriceps index and 90% single leg hop index, return to full running and sport-specific drills, and resume competition. Treatment during phase 4 includes plyometric training, full agility and sport-specific drills, continued dynamic proprioceptive exercises and rebounder training, and road running. In general, return to competition is allowed after the following are achieved: there are no signs or symptoms of instability and there is a normal ligament exam; quadriceps strength is at least 90% when compared to the contralateral extremity; and sport-specific skills, agility testing, and athletic activities do not cause any pain.39
Methods
We evaluated our own data and performed an analysis of the patterns of MCL injuries and the management of these injuries by a single surgeon at the Sports Medicine Center at the Massachusetts General Hospital between July 2001 and August 2011. After IRB approval was obtained, patients with MCL-injured knees were identified in the electronic medical records system. The database was queried using the diagnosis codes 844.1 (sprain or strain of the MCL in the knee) and 717.82 (old disruption of MCL in the knee). In addition the database was queried using the procedure codes 27405 (primary repair of collateral ligament and/or capsule of the knee) and 27599 (unlisted procedure, femur or knee). Injuries included any type of isolated MCL or multiligamentous knee injury where the MCL was repaired or reconstructed. Medical records were reviewed in order to determine demographic information, mechanism of injury, anatomical structures involved, pattern of injury, time from injury to surgical intervention, operative indications, method of surgical repair or reconstruction, whether additional surgeries were required, and clinical and functional outcome.
Results
Each year, approximately 4000 patients were seen and approximately 800 surgeries were performed. Over the ten year period, 385 patients were evaluated with MCL injuries of all grades, accounting for less than 1% of the total clinic volume. Of these, only 19 patients had operative repair or reconstruction of the MCL for a total of 20 surgeries (one required revision). Thus, only 5% of MCL injuries evaluated underwent surgery, which reflects approximately 0.25% of the total surgical volume the clinic. Clearly MCL repair and reconstruction were rarely performed.
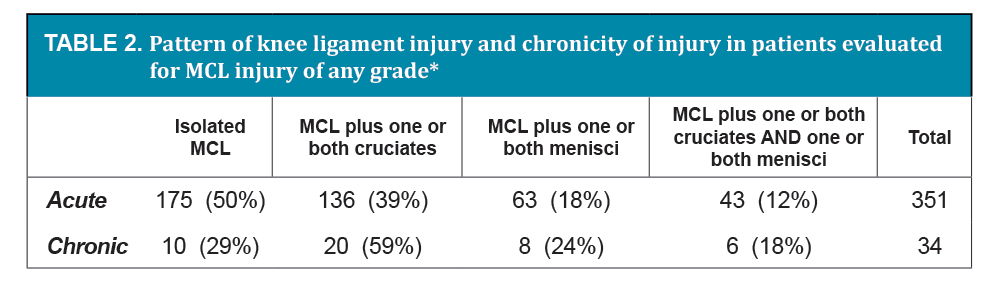
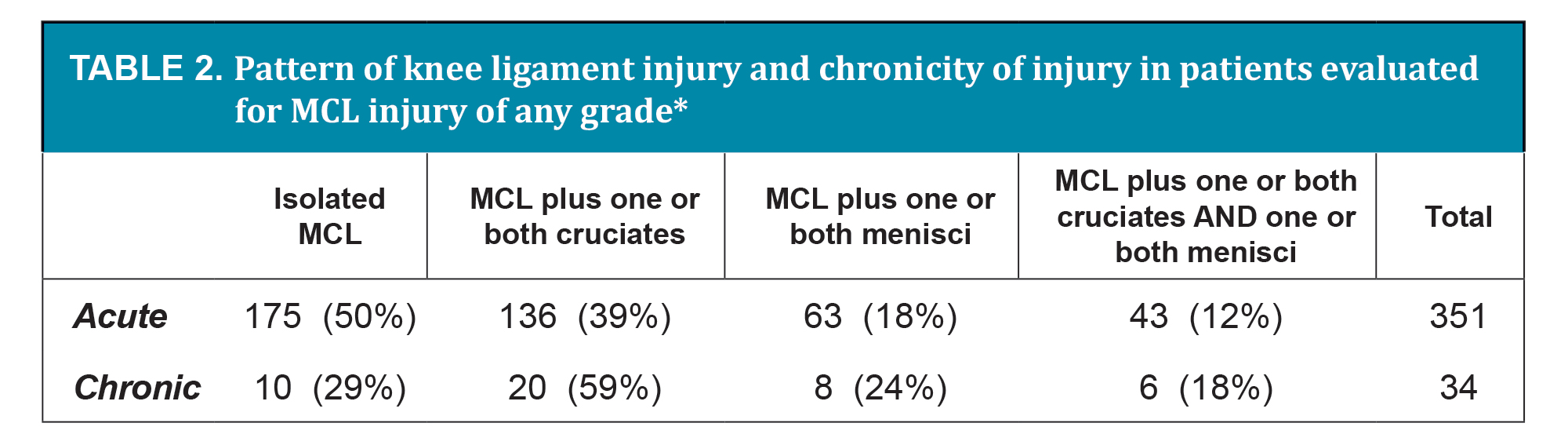
Of the population of patients evaluated with MCL injuries, 351 were acute injuries and 34 were chronic injuries at the time of presentation. Of the 351 acute injuries, 175 (50%) were isolated MCL injuries; 136 (39%) involved the MCL and one or both cruciate ligaments; 63 (18%) involved the MCL and one or both menisci; and 43 (12%) involved the MCL, one or both cruciate ligaments, and one or both menisci. Of the 34 chronic injuries, 10 (29%) were isolated MCL injuries; 20 (59%) involved the MCL and one or both cruciate ligaments; 8 (24%) involved the MCL and one or both menisci; and 6 (18%) involved the MCL, one or both cruciate ligaments, and one or both menisci. (Table 2)
{kind=link}
{kind=link}
The demographics and mechanism of injury of the 19 operative cases showed the following: men outnumbered women by 17 to 2 (90% men); the average age at the time of surgery was 33 (range 16 to 64); two patients were professional athletes and were injured playing their sport; and there were 13 sports injuries, 6 high energy trauma injuries, and 2 injuries at work. There were 4 chronic injuries, defined as presenting more than 6 months after injury. There were 4 patients with prior surgery in the ipsilateral knee. There were 7 left and 12 right knees, and all MCL injuries were classified as either grade 2 or grade 3.
Almost all operative cases had more than one incompetent ligament at the time of injury.
- • Isolated MCL injury: 2 out of 19 (10%)
- - Both patients with isolated MCL injuries had undergone a prior remote ACL reconstruction and had no history of previous MCL injury.
- - Injury to the posteromedial corner was also diagnosed in both cases.
- • ACL + MCL combination: 7 out of 19 (37%)
- - One patient in this group had a remote ACL reconstruction and MCL repair. He sustained a new injury and ruptured both the ACL graft and MCL repair. He underwent repeat ACL reconstruction and MCL repair, but the revision MCL repair failed and he required MCL reconstruction.
- • PCL + MCL combination: 2 out of 19 (10%)
- - Both patients had chronic injuries (time from injury to surgery was more than 9 months in both cases).
- • ACL/PCL/MCL combination (all were documented dislocations): 5 out of 19 (26%)
- • ACL/PCL/MCL/LCL combination (all were documented dislocations): 3 out of 19 (16%)
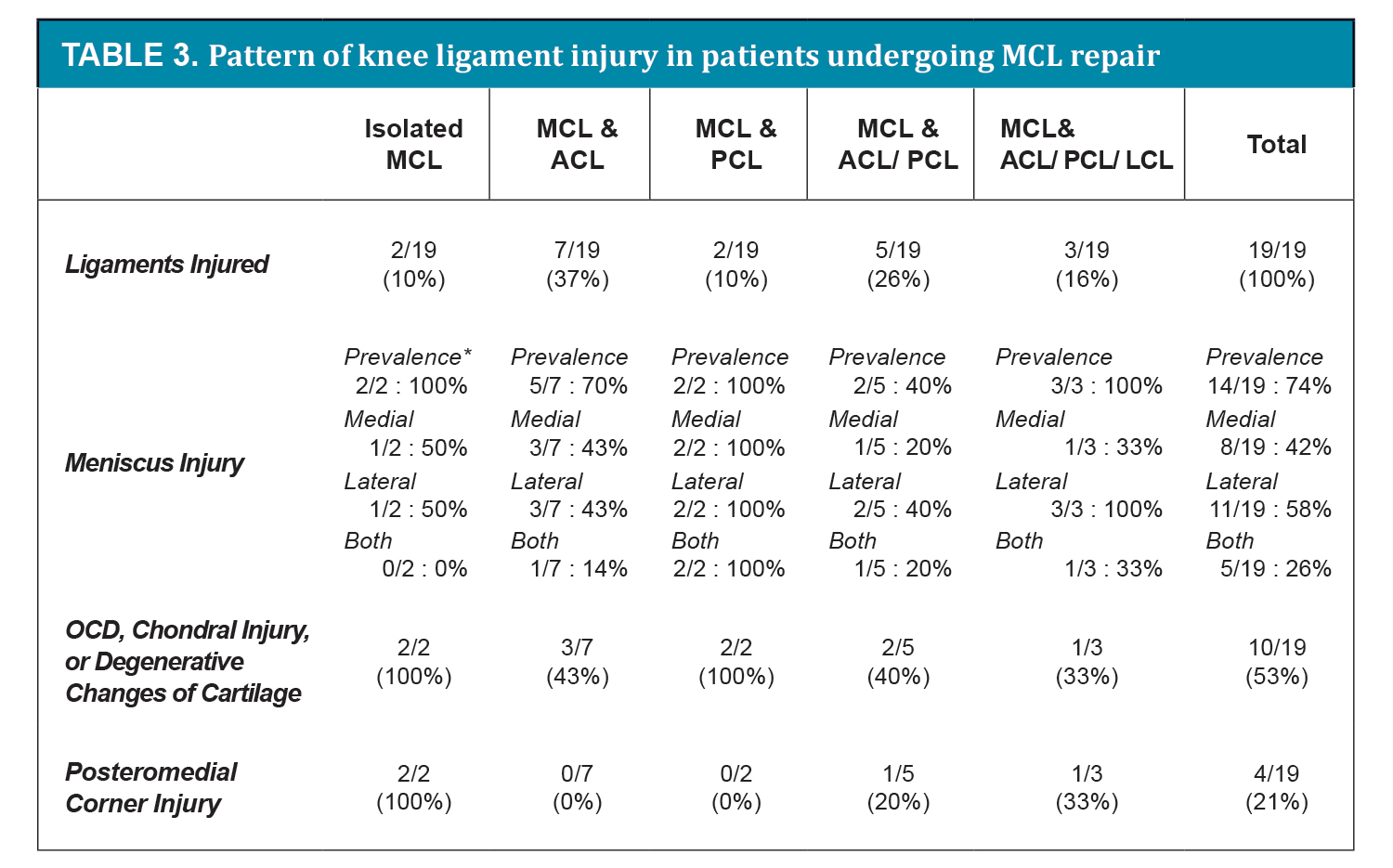
Most patients had concomitant injuries in the same knee. As indicated above, 9/19 patients (47%) had one cruciate ligament ruptured and 8/19 patients (42%) had knee dislocations with both cruciate ligaments ruptured. In addition, 14/19 patients (74%) had meniscal pathology requiring partial resection or repair. Osteochondral defects, chondral injury, or significant degenerative changes of the cartilage were found in 10/19 patients (53%)(Table 3).
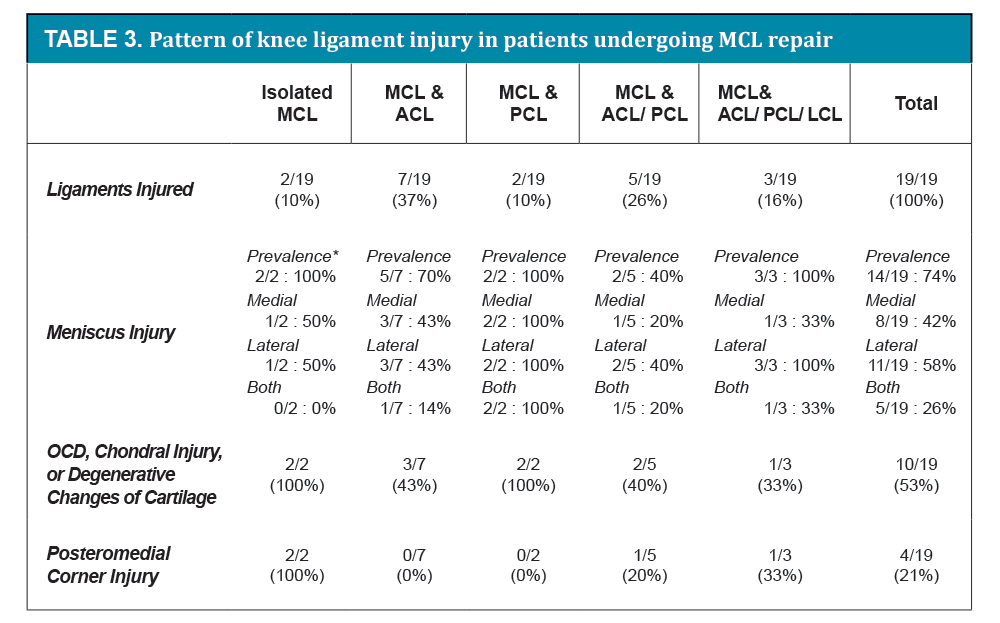
*Prevalence refers to the total number of patients having any meniscal injury
MCL = medial collateral ligament, ACL = anterior cruciate ligament, PCL = posterior cruciate ligament, LCL = lateral collateral ligament, OCD = osteochondral defect
{kind=link}
Overall, our experience was similar to that of previously published studies in terms of the following parameters: demographics; mechanism of injury; time from injury to surgical intervention; pattern of ligamentous injury deemed appropriate for surgery; prevalence of concomitant intra-articular injuries; and the direct relationship between chronicity and prevalence of both meniscal injury and articular cartilage defects.
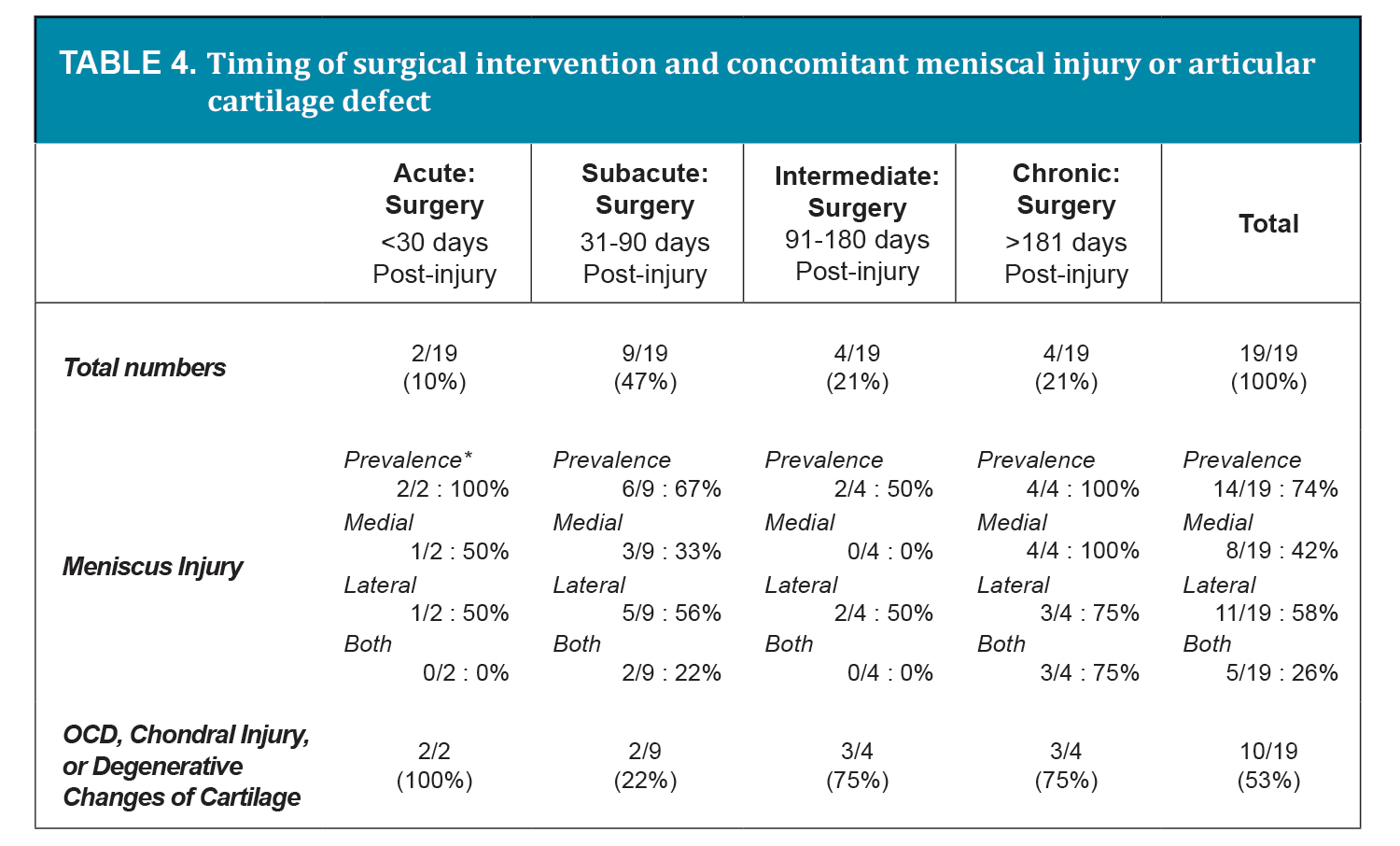
There are two apparent exceptions which deserve further explanation. First, our results suggest that the risks for meniscal injury and cartilage defects were highest in the MCL/PCL group where 2/2 patients (100%) had defects in articular cartilage as well as both medial and lateral menisci (Table 3). However, both of the MCL/PCL patients in our series had chronic injuries. Prior studies have demonstrated that the prevalence of degenerative changes, including meniscal tear and articular cartilage defects, is higher in chronic injury groups.<sup>13, 26-29</ Our results also suggest that the risk for meniscal injury was highest in the chronic injury group, in which 4/4 patients (100%) had a meniscal injury and 3/4 patients (75%) had defects in both medial and lateral menisci (Table 4). Our results also suggest that the risk for articular cartilage defects was high in both the intermediate and chronic injury groups, where 3/4 patients (75%) had evidence of chondral damage at the time of surgery (Table 4). It is possible that that the meniscal injuries and cartilage defects noted in the MCL/PCL group were primarily related to chronicity rather than ligament injury pattern.
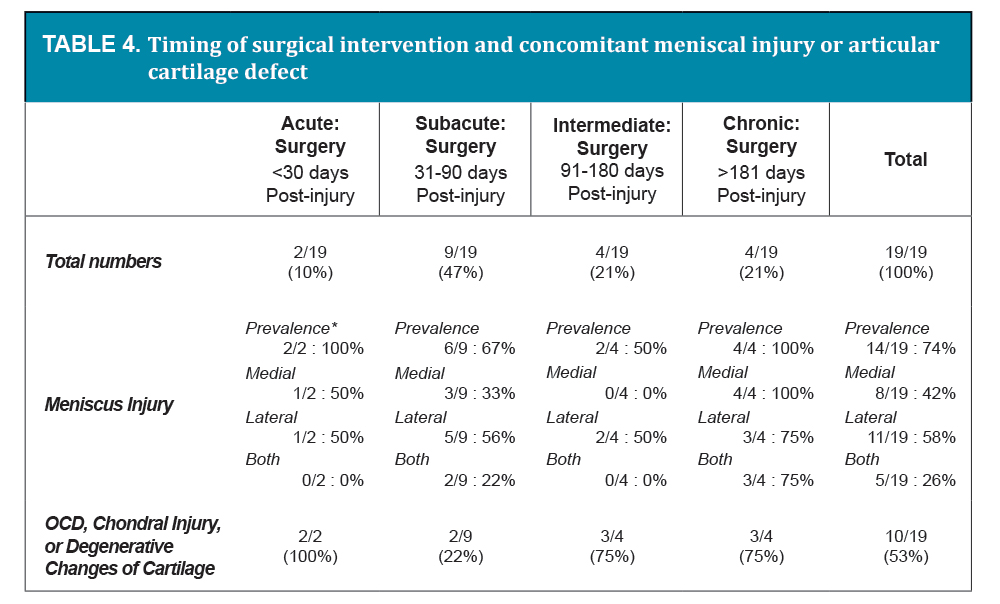
*Prevalence refers to the total number of patients having any meniscal injury
OCD = osteochondral defect
{kind=link}
The second apparent exception is related to the unanticipated finding that both patients with isolated MCL injuries had concomitant meniscal, articular cartilage, and posteromedial corner injuries. All of these injuries were observed in 2/2 patients (100%) (Table 3). However, both of these patients had prior trauma to the same knee and had required ACL reconstruction in the past. This history suggests that there may be a cumulative effect of multiple traumas or a component of mild chronic ligamentous insufficiency contributing to the observed pathology.
Surgery was most frequently performed between 30 and 90 days after injury. This delay was intended to allow the acute knee effusion to resolve, give the MCL time to heal independently, and allow the patient to regain full range of motion with physical therapy. In the case of severe trauma, however, repair was often delayed for more than a year. Only 2/19 cases (10%) underwent staged surgery, and these were for knee dislocations in the setting of high energy trauma. Acute surgical repair (<30 days post-injury) was performed in another 2/19 cases (10%); both were professional athletes. The majority, 9/19 cases (47%), underwent subacute repair (31-90 days post-injury); 4/19 cases (21%) underwent intermediate repair (91-180 days post-injury); and 4/19 cases (21%) underwent delayed repair (Table 4). The surgical patients with higher energy trauma, knee dislocations, other concomitant injuries in the same knee, and chronic injuries had generally poorer outcomes with respect to stability, pain, and development of degenerative changes in the knee.
In our series there were 18 MCL repairs and 2 reconstructions in 19 patients (one was a revision). We follow a specific protocol when considering surgery for the MCL. For acute knee injuries, we recommend physical therapy for four to six weeks with a short period of bracing. This provides time for the MCL to heal and allows the patient to regain full knee range of motion. Once this period of rehabilitation is complete, isolated MCL injuries are examined for persistent valgus laxity, quality of endpoint, and pain. Depending on the findings surgery may be considered. If there is a concomitant injury to one or both cruciate ligaments, they are reconstructed, and immediately afterward an intraoperative examination of the MCL at 0 and 30 degrees of flexion is performed. If there is significant valgus laxity compared to the contralateral knee, the MCL is repaired, with or without repair of the posteromedial corner as indicated at the time of surgery. In our practice MCL repairs are performed using a pants-over-vest imbrication technique. MCL reconstructions are reserved for failed repairs or cases with severely attenuated tissues.
Conclusions
Evidence from the literature and our experience supports several conclusions:
- • Most MCL injuries are nonoperative and can be managed appropriately by their primary care physicians or sports medicine specialists. This is likely the reason that such a common injury comprises such a small proportion of a surgeon’s practice.
- • An appropriate period of bracing and attention to the type of physical therapy utilized is essential for optimizing rapid recovery and an excellent outcome.
- • Most importantly, it is essential to rule out concomitant intra-articular pathology, particularly for higher grade injuries. An accurate history, a detailed physical exam, and appropriate imaging are necessary in all cases. Cruciate ligament rupture, meniscus tears, and osteochondral defects may require surgical intervention and should be rapidly detected.
Acknowledgements
Thanks to the entire staff of the Sports Medicine Center for all their help and support.
None of the authors have any conflicts of interest that pertain to this research.
1Dania Magri, MD: Harvard Combined Orthopaedic Surgery Residency Program
55 Fruit Street WHT 535
Massachusetts General Hospital, Boston, MA 02114
2Thomas J. Gill IV, MD: Sports Medicine Service, Massachusetts General Hospital
Medical Director: New England Patriots
Associate Professor of Orthopaedic Surgery, Harvard Medical School
3Thomas J. Gill III, MD: Director of Research, Sports Medicine Service, Massachusetts General Hospital
Lecturer in Orthopaedic Surgery, Harvard Medical School
Email: tjgill3@partners.org
References
