
Original Submissions
Current Issue: Volume 15 |  PDF
PDF
Granular Cell Tumor Presenting as a Pediatric Spinal Deformity
Terrill P. Julien, M.D. and M. Timothy Hresko, M.D.
Department of Orthopaedic Surgery, Boston Children’s Hospital, Harvard Medical School, Boston, MA 02114
PDF
Abstract: Granular cell tumors (GCTs) occur very rarely in the pediatric population. A granular cell tumor arising from the epidural spinal canal itself has never been described in a pediatric patient. We present a case of an epidural-based granular cell tumor that presented with a rapidly progressive scoliotic deformity in a 12 year-old boy. The computed tomography (CT) and magnetic resonance imaging (MRI) studies showed a dumbbell-shaped lesion, consistent with a neurogenic paravertebral tumor. However, the pre-operative needle biopsy showed positive immunohistochemical staining for S-100 and histology was consistent with a granular cell tumor. A single-stage resection of the tumor with posterior segmental instrumentation yielded a successful result.
Keywords: astrocytoma, epidural, granular cell, paravertebral, neurofibromatosis, scoliosis
Background
Granular cell tumors (GCTs) occur infrequently in the spine. Several studies have contributed to our understanding of the histology, origin and clinical course of these tumors. While the tumor was first described by Abrinkossoff in 1926, there is still debate regarding the true cell origin of the tumor. The vast majority of GCTs are benign, with malignant tumors accounting for less than 1%.9 To date, granular cell tumors have been described in the breast, larynx, appendix, palm, eye, peripheral nerves and chest wall.1,6,9,16,19 Granular cell tumors in the spine are extremely rare, with few reported to date. We report a case of a 12 year-old boy with a GCT found on imaging for atypical scoliosis. To our knowledge, the have been no reports in the literature of a GCT occurring this early presenting as neurogenic scoliosis.
Case Report
A 12-year old boy presented to our spine clinic for evaluation of a scoliotic deformity that was initially noticed by his pediatrician approximately one year earlier. He denied any activity-related or night pain. Family history was negative for neurofibromatosis, Marfan’s Syndrome, cardiac or renal abnormalities. His father was diagnosed with scoliosis as a child but required no treatment. His father’s history was also significant for medullary thyroid cancer and a lower extremity soft tissue sarcoma, both treated successfully with surgery, chemotherapy and radiation. Our patient had an unremarkable initial physical examination with no signs of hyperlaxity (0/5 on the Marshall scale) or spinal tenderness. He had no café au lait spots, hairy patches or dimples. He had level shoulders and pelvis. His initial Adam’s forward bending test showed an axial trunk rotation by scoliometer reading of 7 degrees in the midthorax. His neurologic exam was benign.
Given the appearance of a new curve and a clinically suspicious reading on scoliometer testing, standing spinal radiographs were obtained which showed a Lenke 2 double thoracic curve which measured 25 degrees to the left in the upper thorax and 25 degrees to the right in the lower thorax by Cobb measurement. Pelvic films showed a Risser stage zero.
As he was asymptomatic, it was elected to monitor him clinically with repeat examinations and radiographs. He was seen in clinic four months later with a stable exam and radiographs. At the eight-month follow-up, radiographs demonstrated curve progression from 25 to 30 degrees in both curves. An MRI was obtained to rule out intraspinal abnormalities based on his young age of presentation and a new clinical exam finding of 2 beat ankle clonus.
The MRI showed a large, enhancing epidural lesion at T5 which extended out of the left T5-T6 neural foramen into the adjacent soft tissues (Figure 1a, 1cb, 1c). There was impingement on the spinal cord by the mass at that level without any signal changes within the cord. The mass measured 1.8 x2 2.4 cm and was low intensity on T2 (Figure 1b). A CT scan was obtained which showed no destructive elements of the mass or cortical breakthrough, but the diagnosis remained unclear. A percutaneous biopsy was obtained revealing polygonal tumor cells with finely eosinophillc cytoplasma and a moderate degree of nuclear atypia. Immunohistochemical stains revealed an S-100 positive tumor that was also negative for synaptophysisn, chromogranin and epithelial membrane antigen (EMA).

(A) Coronal T2-weighted MRI showing the tumor exiting the neuroforamen into the adjacent soft tissue at T5 (B) Saggital T2 showing the extent of the tumor from T4 to T6 (C) Axial T1-weighted showing the extent of the mass.
All Rights Reserved. Permission For Use Required.
-View Large-{kind=link}
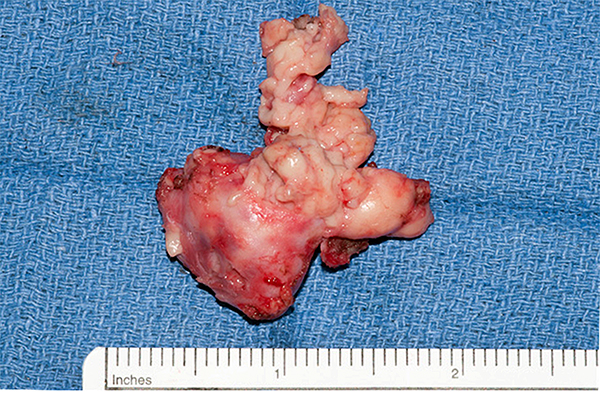
Gross specimen with tan, irregular borders and overlying adipose tissue measuring 3.0 x 2.5 x 1.5cm
All Rights Reserved. Permission For Use Required.
-View Large-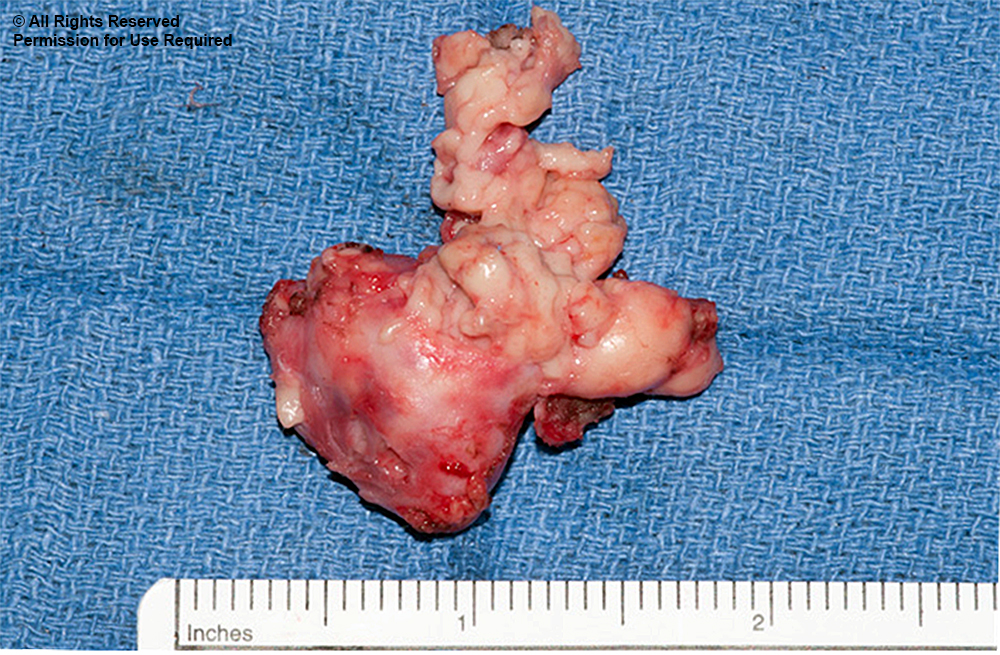{kind=link}
Macroscopic Description
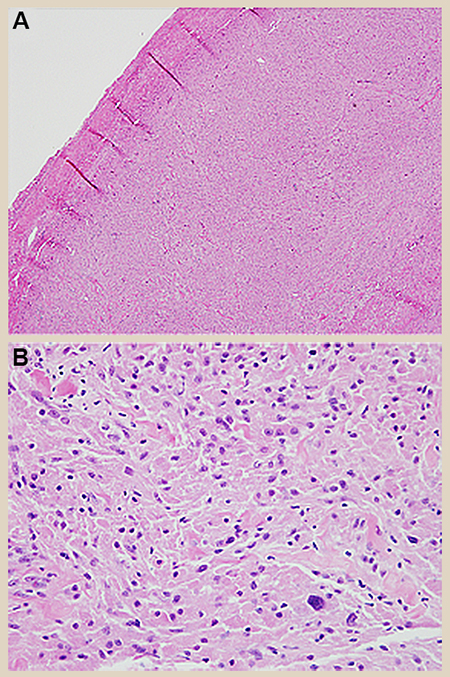
Histologically, sections of the tumor showed a well-circumscribed mass and strands of polygonal cells separated by thin fibrous septa. The cells had characteristic, copious, finely granular, eosinophilic cytoplasm. Despite a moderate degree of nuclear atypia, rare (1/10 HPF) mitoses were seen and no necrosis was present (Figure 3). Immunohistochemical stains were also performed, confirming the findings from the initial biopsy, which were S-100 and inhibin positive and, negative for synaptophysisn, chromogranin and EMA (Figure 4). Additionally, Olig-2 staining was negative and PAS staining showed granular cytoplasmic positivity. The proliferation index by Ki-67 (MIB-1) was estimated at 1-3%.
All Rights Reserved. Permission For Use Required.
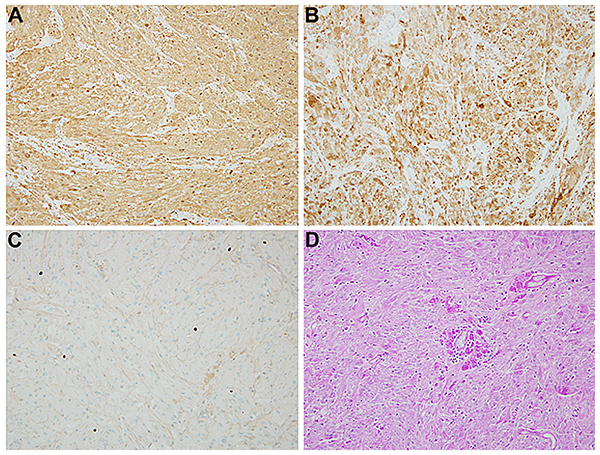
Figure 4. Neoplastic cells are diffusely immunoreactive with S-100 protein (A) and inhibin (B). The proliferation index by Ki-67 (MIB-1) was low (C). In addition, the cytoplasmic granules were periodic acid Schiff (PAS) positive (D).
All Rights Reserved. Permission For Use Required.
-View Large-{kind=link}
Figure 3. Hematoxylin and eosin stain revealed (A) a well-circumscribed mass composed of nests and strands of polygonal cells separated by thin fibrous septa. (B) The cells had abundant, finely granular, eosinophilic cytoplasm and a mild degree of nulcear atypia.
-View Large-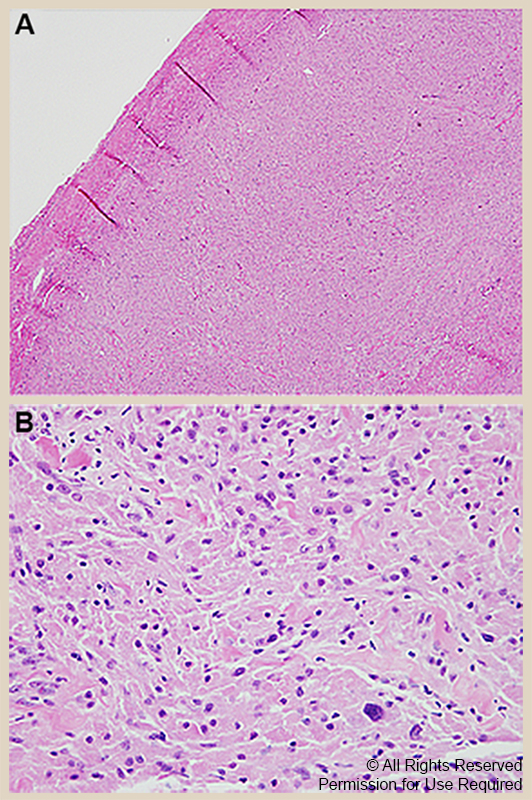{kind=link}
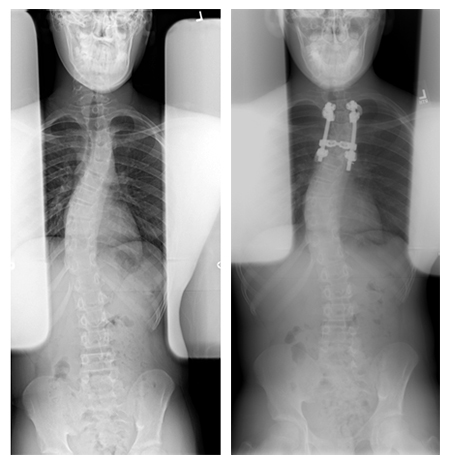
Initial preoperative standing plain films with a high left thoracic curve of 25o and a right thoracic curve of 25o. Post-operative films show a stable curve.
All Rights Reserved. Permission For Use Required.
-View Large-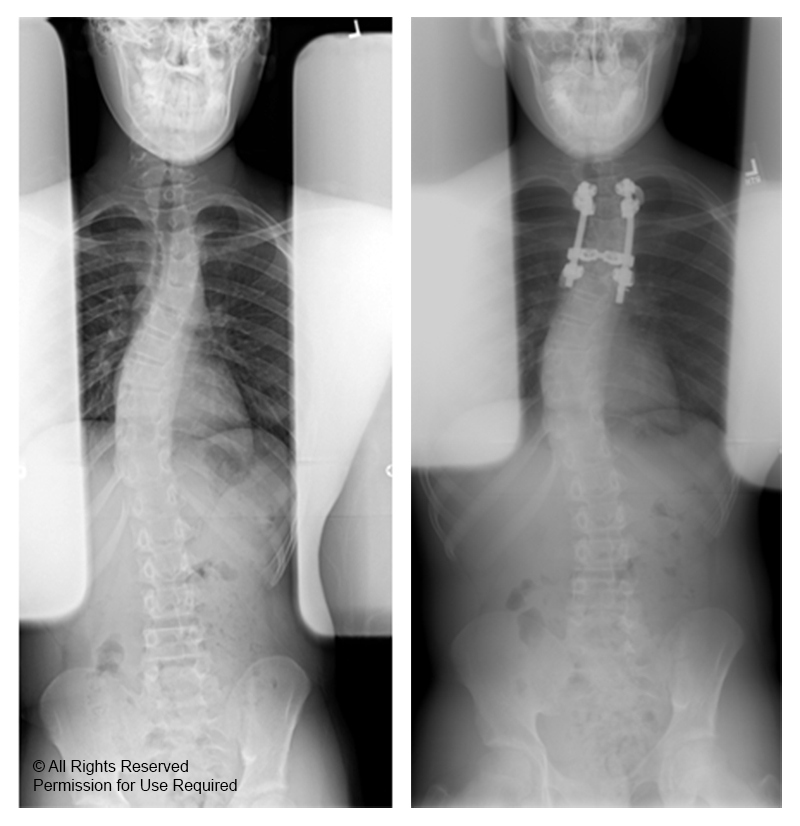{kind=link}
His post-operative course was uncomplicated and he was discharged home on post-op day five. On follow-up clinical evaluations, he is pain free and progressing well. At his one-month visit, his lower right thoracic curve was stable at 30 degrees and he was fitted for a brace (Figure 5). At his four-month follow-up, he had a stable curve and was wearing his brace 18-20 hours daily and tolerating it well.
Discussion
Granular cell tumors (GCTs) occur very rarely in the pediatric population. The typical presentation is between the third and sixth decades with a female to male ratio of 2:1.9,11 Most reports demonstrate their occurrences in epithelial tissue, the GI tract and occasionally in the spine and central nervous system (CNS).1,2,6-9,12,13,16,17,19,20 The most common presentation is in the epithelial tissue where it presents as small, non-tender solitary nodules.12 GCTs associated with spinal cord are exceptionally rare, with only four intradural cases in the literature to our knowledge.4,7,19,20 A granular cell tumour arising from the epidural spinal cord has never been previously described. The distinctive pattern of granular cytoplasmic changes is due to the accumulation of lysosomes, although the histogenesis of the granular cell tumor is still uncertain.5 It was first named “myoblastenmyome’’ in 1926 by Abrikossoff, but the cumulative evidence from many reports incorporating electron microscopy and immunohistochemical studies has ruled out this possibility and support a Schwannian differentiation.14,15
The pathological diagnosis of these tumors can be difficult. The granular appearance can share similar traits as infarcts, inflammatory processes and all manner of neoplasms. Therefore, initial biopsies should not be solely relied on for diagnosis.3,21 For spinal tumors in this location, the differential will include schwannoma, neurofibroma, meningioma, ganglioneuroma, paraganglioma, and granular cell astrocytoma. Schwannoma and neurofibroma are the most important differential diagnostic considerations as they also be positive for S-100 protein, but negative for inhibin and tend to be more spindled and without cytoplasmic granularity. Meningiomas may have a whorled cytologic appearance, psammoma bodies, and are usually EMA positive. Paragangliomas have a zellballen pattern, with chief cells positive for chromogranin and synaptophysin, while sustentacular cells showing S-100 protein reaction. Ganglioneuroma has large, interspersed ganglion cells with prominent nuclei, showing a strong staining for synaptophysin and neurofilament protein. Similarly, the GFAP and OLIG-2 positivity would help to confirm the diagnosis of a granular cell astrocytoma (Table 1).
Table 1.
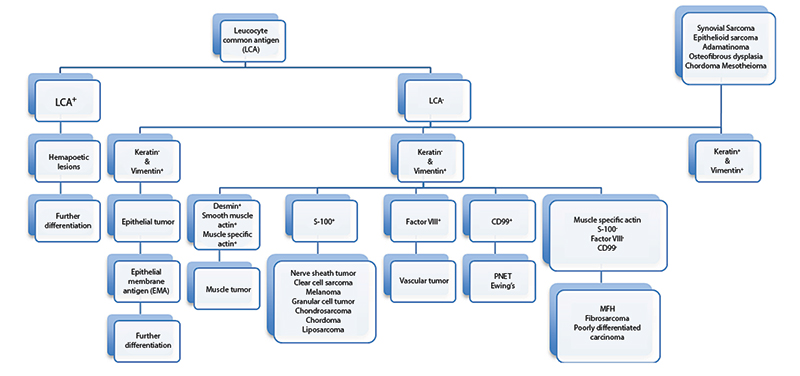
Immunoperoxidase staining flowchart for poorly differentiated tumors.
All Rights Reserved. Permission For Use Required.
-View Large-{kind=link}
MRI is commonly used to aid in the diagnosis of this tumor. On the T1-weighted images, the tumors are well-defined, hypo-intense lesions compared to the spinal cord. T2-weighted images show a hyper-intense lesion which increases uniformly with contrast.7,19
The mainstay of treatment for this tumor is largely surgical excision. When occurring in the lumbar spine in an asymptomatic patient, some authors have recommended close observation for signs of neurologic decline. However, although the majority of GCTs are benign, due to the anatomic constraints in the thoracic spinal canal and the risk of spinal cord compression, surgery should be considered early in the course.18 Although Barrenechea described good results in a series of 13 patients from 1997-2004 who underwent endoscopic removal of paravertebral tumors via a hemilaminectomy followed by a thoracoscopy generally, the treatment is a posterior midline or paraspinal approach followed by excision.2 Reported recurrence rates are approximately 7% in the case of incomplete resection.9,10,14,15 In our patient, the extent of the tumor required spinal destabilization which was addressed with posterior stabilization and the patient has done well over time.
Conclusion
To our knowledge, this is the first report of an intraspinal GCT presenting as with scoliosis in the pediatric literature. The report underscores the importance of a systematic workup of patients who present with an atypical or progressive scoliotic deformity including close clinical follow-up, accurate physical examination, advanced imaging and an interdisciplinary approach to surgical decision-making.
References
