
Original Submissions
Current Issue: Volume 15 |  PDF
PDF
Biceps Tenodesis in a 22-year-old Female Softball Pitcher: A Case Report
Reg B. Wilcox, III, P.T., D.P.T., M.S., O.C.S., Justin Jones, P.T., D.P.T., O.C.S., Elana J. Siegel, B.A., Laurence D. Higgins, M.D.
Sports Medicine Service, Department of Orthopaedic Surgery, Brigham and Women’s Hospital, Harvard Medical School, Boston, MA 02114
PDF
Abstract: Injury to the long head of the biceps (LHB) is a common source of pain in the shoulder, typically presenting with rotator cuff involvement. In the case of trauma to the LHB, patients may be indicated for a biceps tenotomy versus tenodesis, with the latter recommended for younger patients. The following case study will present a 22-year-old Division III collegiate softball pitcher who sustained a traumatic, isolated proximal biceps rupture without rotator cuff damage. He was subsequently managed with biceps tenodesis and physical therapy, and was able to make a successful return to fast underhand softball pitching.
Keywords: long head biceps tendon, tenodesis, arthroscopy, shoulder, pitcher
Background
The long head of the biceps tendon (LHB) is an intra-articular structure of the shoulder, running within the bicipital groove and exiting the intra-articular space.24 Its exact role in glenohumeral mechanics is not definitively understood, yet damage to the LHB tendon is a frequent source of pain in the shoulder. LHB pathology is divided into three types: instability, inflammatory and traumatic conditions.34 Isolated, traumatic biceps tendon ruptures are relatively rare, as tears classically co-present with chronic microtrauma within the shoulder.26 A review of the literature reveals that, to date, there are no well-controlled, randomized clinical trials that decisively determine whether tenotomy or tenodesis of the LHB is the superior treatment, although tenodesis is generally preferred for patients under the age of 50.5,27 As patient outcomes display little variability between the two procedures, the role of the tenodesis is primarily considered a cosmetic one, as the Popeye’s sign appears in approximately 43% of patients with ruptured LHBs.3 In the athletic population, however, there is a general consensus that the biceps should be preserved, particularly in overhead athletes. To date, there are few reports of successful management of biceps rupture treated with tenodesis that have resulted in return to competitive overhead sport.
Various methods of arthroscopic or open tenodesis have been reported, which can comprise soft tissue suturing or the use of suture anchors, interference screw, screw and washer, and bone tunnels. LHB fixation is typically performed above the bicipital groove or beneath the pectoralis major muscle.5
Case Report
A 22-year-old right hand dominant female Division III college softball pitcher presented to an outside orthopaedic surgeon with diffuse rotator cuff related overuse symptoms. She was originally prescribed oral corticosteroids to address the pain.
She was advised to begin a general rotator cuff strengthening program and continue pitching. Three weeks into her rotator cuff strengthening program, she sustained a sudden injury while pitching in a game. She reported feeling a pop in her right shoulder during the follow-through phase of her pitch. She was evaluated by her team physician following the injury and told she had a “career-ending injury.” After being seen by a physical therapist one day after her injury she was advised to seek an orthopaedic consult, as she had an obvious deformity of her biceps tendon consistent with the Popeye’s sign.27 The patient displayed nearly full shoulder active range of motion of 150° of forward flexion and 70° of external rotation, and could rotate internally rotate behind her back to her upper lumbar spine bilaterally. Rotator cuff strength testing for the supraspinatus, infraspinatus and subscapularis each scored 5/5 by manual muscle testing. She reported no tenderness at her acromioclavicular joint and had a negative cross-arm adduction exam. She complained of tenderness over her proximal biceps groove and noted pain with Speed’s Test. The patient was neurovascularly intact. Overall, she subjectively rated her right shoulder value as 50%, scoring her contralateral side as 100%.
The patient’s MRI confirmed the presence of a right superior labral tear and ruptured proximal biceps tendon, evident on the sagittal oblique view,near the humeral metaphysis (Figure 1) as well as the coronal view (Figure 2). Her rotator cuff was intact. Given the patient’s age, activity level and the acute nature of the injury, it was recommended that the patient undergo surgery to perform a biceps tenodesis through an arthroscopic approach.
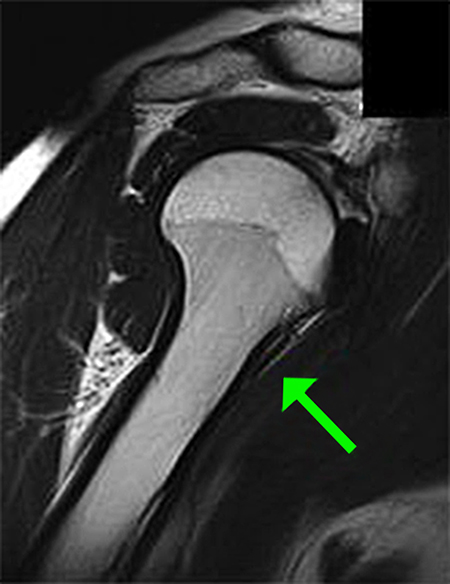
Sagittal oblique view of MRI illustrating torn biceps tendon
All Rights Reserved. Permission For Use Required.

Coronal view of MRI showing torn biceps tendon
All Rights Reserved. Permission For Use Required.
The patient was taken to surgery 13 days post-injury, 2 days after our clinical evaluation. Examination under anaesthesia revealed a stable shoulder with 2+ anterior, 2+ posterior and 1+ inferior laxity with Sulcus sign, which diminished with external rotation. Arthroscopic evaluation demonstrated that the cartilage of the humerus and glenoid was intact, as was the anterior, posterior and inferior labrum. The rotator cuff was pristine, and a visualization of the subacromial space revealed an unharmed bursal side of the subacromial space. The superior labrum presented with an avulsion-type tear, and we confirmed a complete detachment of the biceps tendon, retracted down to the intertubercular groove.
The superior labrum was debrided back to a stable margin, having been avulsed from its superior attachment. There was no tissue amenable to repair. Hemostasis was secured after the torn degenerative labrum was debrided.
The arthroscope was then directed into the subacromial space, where the bursal side of the rotator cuff was inspected and noted to be intact. No bony decompression was performed.
In order to address the biceps tendon, the arm was placed in forward flexion with the scope still in the subacromial space. The biceps was found proximally and traced down to the distal end of the intertubercular groove. The pectoralis major muscle was identified, and the biceps was held in place in the supra-pectoral region while the humerus was prepared. A small incision was placed for percutaneous insertion of an Osteoraptor (Smith and Nephew, Andover MA) anchor. The anchor was inserted in the supra-pectoral region. Using an accessory portal, the biceps was held under tension whilst the sutures were retrograded in a lasso-loop fashion to retrieve the biceps tendon and eliminate the Popeye’s deformity (Figure 3). The patient’s arm was brought through range of motion and the biceps deformity was no longer present. All wounds were irrigated and closed, and the patient was placed in a standard sling (Figure 4).
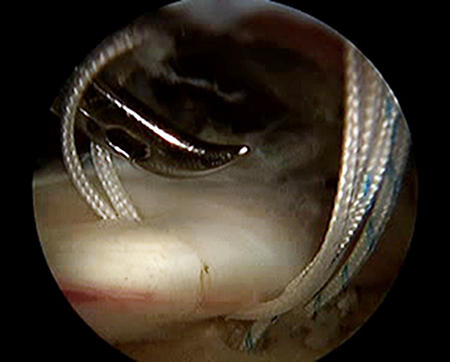
Passing sutures during arthroscopic biceps tenodesis
All Rights Reserved. Permission For Use Required.
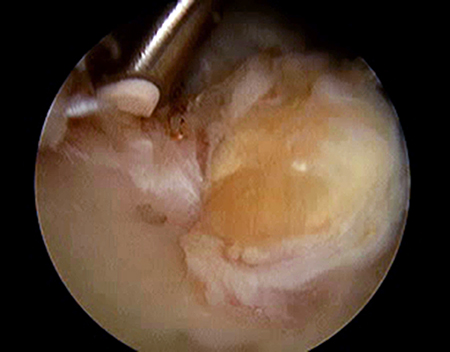
Final appearance after biceps tenodesis
All Rights Reserved. Permission For Use Required.
At 2-week follow-up, the patient reported minimal discomfort and was tolerating the physical therapy regimen well. All of the patient’s neurovascular structures, including axillary, median, radial and ulnar nerve distributions were intact. At 14-week follow-up, she had normal biceps contour and displayed full active range of motion in abduction, forward flexion, and internal and external rotation. Isometeric right rotator cuff strength by hand held dynamometry revealed 7.9 kg in abduction and forward flexion (left 6.3 kg), 7.5 kg in external rotation (left 5.3 kg), 9.5 kg in internal rotation (left 6.9kg) with manual muscle testing revealing 5-/5 in biceps flexion and supination as compared to the contralateral side. Her Shoulder Pain and Disability Index (SPADI) score was 3%.
At 9 months follow-up: she had a SPADI score of 0%, full AROM in all planes, a negative Speed’s test with no pain to palpation of her proximal biceps and normal biceps contour. Isometeric right rotator cuff strength by hand held dynamometry revealed 8.3 kg in abduction and forward flexion (left 7.8 kg), 9.3 kg in external rotation (left 9.0 kg), 10.6 kg in internal rotation (left 10.5kg) with manual muscle testing revealing 5/5 in biceps flexion and supination as compared to the contralateral side.
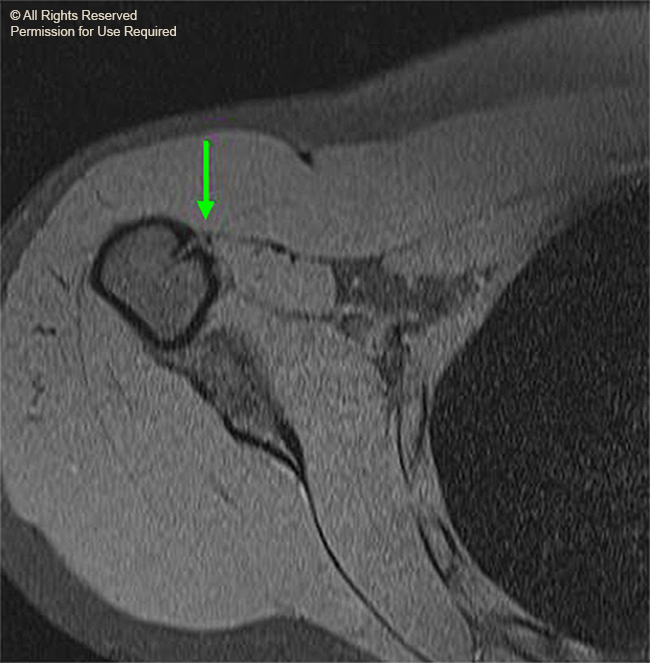
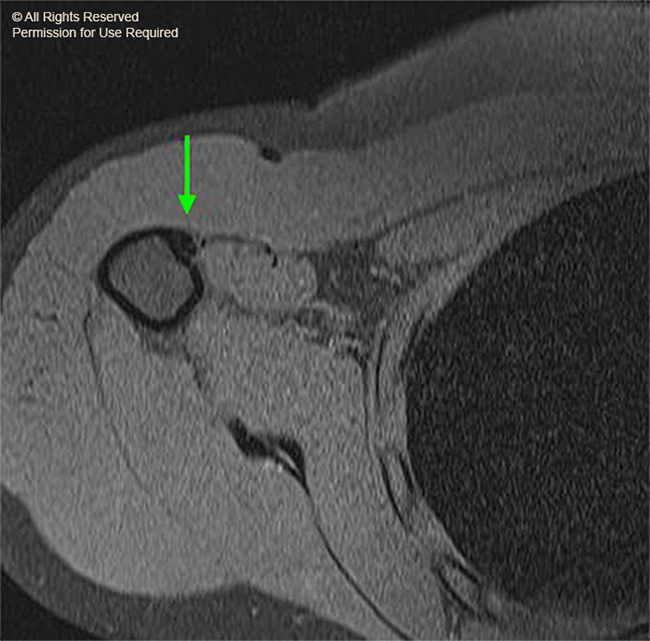
Over the course of this 9-month time period, she had attended 12 physical therapy sessions and had been completely compliant with her progressed home exercise program. Her MRI demonstrated complete healing of the tenodesis (Figure 5, 6). She was advised to begin and progress a throwing program over the next 2-3 months. She stayed in close contact with her physical therapist during this process and had no setbacks. At 11 months after her surgery, the patient had returned to pitching for her collegiate softball team, with minimal discomfort that resolved one or two days after pitching. The patient reported being overall very happy with her outcome and planned to continue with her shoulder strengthening and throwing program. At the 2-year postoperative point she continued to have a SPADI score of 0%, full AROM in all planes, a negative Speed’s test, and a normal biceps contour. Isometeric right rotator cuff strength by hand held dynamometry revealed 8.0 kg in abduction and forward flexion (left 7.8 kg) , 9.0 kg in external rotation (left 9.0 kg), 10.2 kg in internal rotation (left 10.3 kg) with manual muscle testing revealing 5/5 in biceps flexion and supination as compared to the contralateral side. She reported that she had successfully completed her collegiate pitching career without any further shoulder injury.
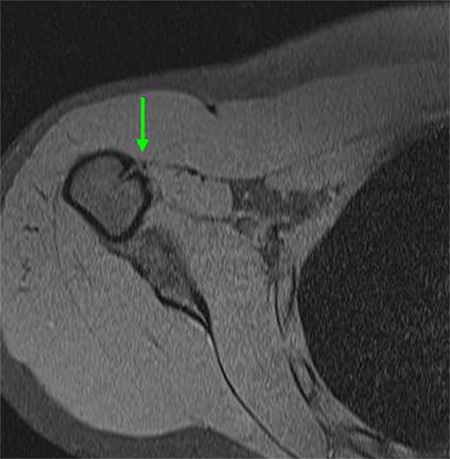
Axial view of MRI depicting anchor from tenodesis
All Rights Reserved. Permission For Use Required.
-View Large-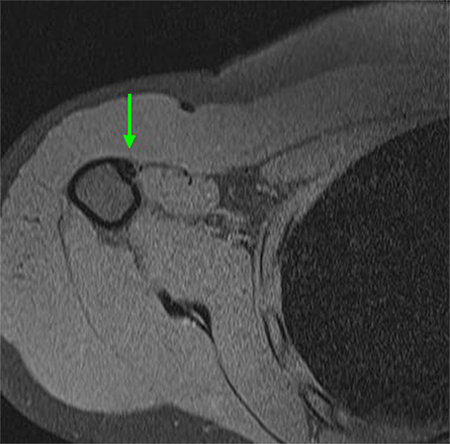
Axial view of MRI illustrating healed biceps tendon
All Rights Reserved. Permission For Use Required.
-View Large-Discussion
The sport of softball has enjoyed increasing popularity over the past several decades and is reported as one of the largest female team sports in the United States from the youth through collegiate ranks.25,17,18 In particular, collegiate fast pitch softball at all three divisions has experienced significant increases in participation over the past decade.2,17,18 According to the NCAA participation report17 there were 13,496 females participating in collegiate softball (Divisions I through III) in the 1996-1997 season and 16,997 total participating collegiate softball players in the 2006-2007 season. As participation in the sport has increased, so too has the need for research contributing to the diagnosis, management and ultimately prevention of common injuries, particularly with regard to the position of pitcher.
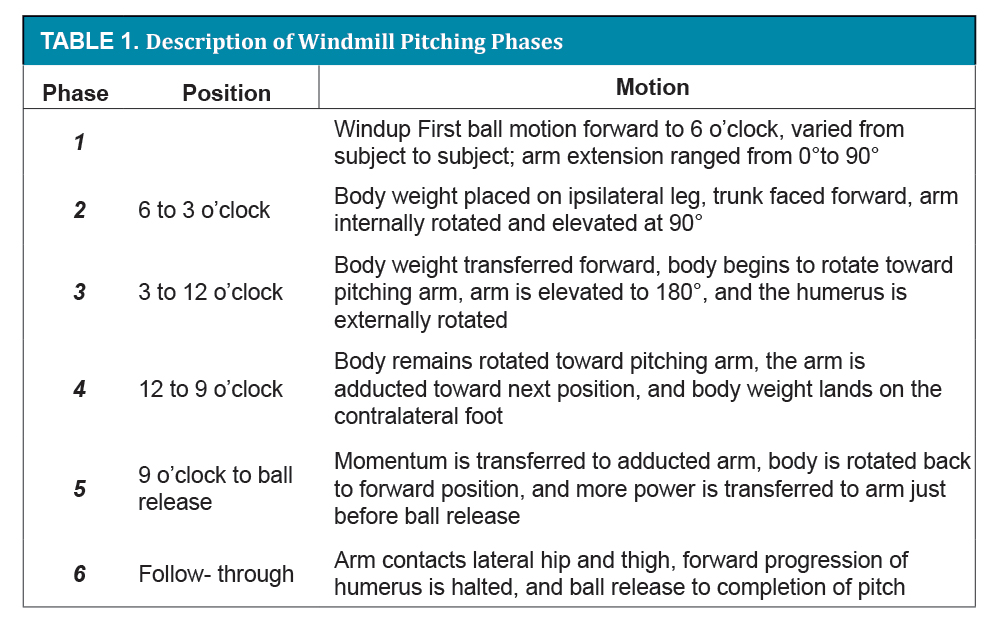
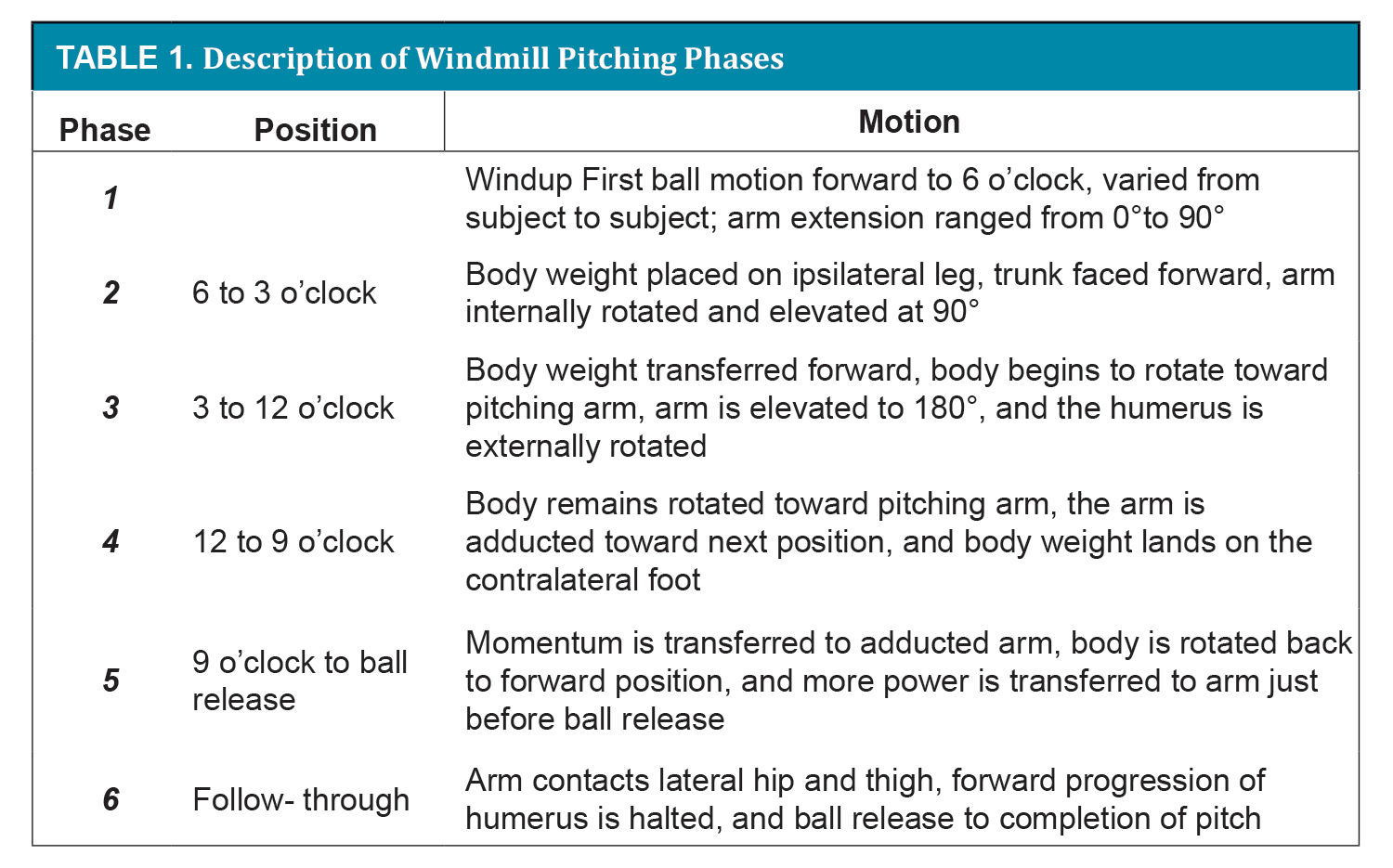
In fast pitch softball, pitchers use an underhand throwing motion that is commonly referred to as the windmill technique and can require up to 485 degrees of total shoulder circumduction to complete.3 It is commonly divided into 6 phases (Table 1). Unlike baseball, there are no regulations on pitches thrown or innings pitched and as a result, pitchers often pitch consecutive games and days with some reports of over 1200-1500 pitches thrown in a weekend.30,31 The biomechanical requirements of this throwing motion have been analyzed in several studies;3,15,20,21,25,30,31 however the amount of research available lacks significantly compared to that for overhand pitching in baseball. This may be due to the historical belief that the windmill style is less stressful on the upper extremity than overhand pitching.3,10 When looking at the literature on injury patterns in softball, however, it appears that windmill pitching may present a greater risk for injury than once thought.9, 25
{kind=link}
{kind=link}
{kind=link}
Hill and colleagues looked at injury incidence in female college pitchers (Division I, II, and III) through a survey which also included demographics, pitching and game data, and information on training programs utilized by the players during the 2001-02 calendar year. Injuries were reported by 131 (72.8%) of the 180 who completed the survey with 57 (31.7%) reporting more than one injury in that time frame. Injuries were further classified into acute (36), chronic/overuse (92), and unspecified (3). 44% of all the injuries were related to pitching and 41% of those pitching injuries were related to the shoulder.10 Kranjik et al reported a rate of 1 shoulder injury per 10,000 activity exposures in high school softball compared to 1.72 shoulder injuries per 10,000 activity exposures in high school baseball players.13 The most common shoulder injuries in both sports were classified as strains/incomplete tears and were more likely to occur in practice than in a game situation in both sports. Marshall et al, using the NCAA injury surveillance data base from 1988-1989 through 2003-2004, found overuse shoulder injuries among the most common conditions in NCAA women’s softball.16
Anecdotally, a common complaint of softball pitchers is anterior shoulder pain and given the demands on the biceps, and repetitive nature of the activity, this may be a potential source of pain in softball pitchers.30,31 Rojas et al. in a study that looked at biceps activity in female fast pitch windmill pitchers found higher biceps activity in all phases compared to baseball pitching.25 In particular, they report significant biceps activity particularly during phase 5, which is the 9 o’clock position to ball release phase. This coincided with the highest demands for reducing elbow velocity and resisting shoulder distraction forces prior to ball release. After ball release the authors suggest that biceps activity may continue as a means of decelerating the arm and reducing distraction during follow through, while others have stated that the deceleration demands may be facilitated by pitchers whose pitching arm strikes the lateral hip which decelerates the arm.2,15 Additionally, given the large range of motion required for windmill pitching the authors theorize that there is a large excursion of the biceps tendon which also could predispose it to injuries.25 The process of long head biceps tendinopathy and risk for spontaneous tear has been analyzed on an anatomical basis and it appears likely that the demands of windmill pitching can predispose an athlete to biceps pathology.19,28
In conclusion, acute rupture of the LHB in young adults is a rare occurrence, with limited reports in the literature. Provided there is no damage to the rotator cuff, a biceps tenodesis may be performed instead of a superior labral repair, and full motion may be regained as in the case of this 22-year-old patient who returned to competitive underhand fast-pitching softball (Figure 7).

Patient returns to pitching 11 months after surgery
All Rights Reserved. Permission For Use Required.
Reg B. Wilcox III, P.T., D.P.T., M.S., O.C.S.: Clinical Supervisor, Department of Rehabilitation Services, Brigham and Women’s Hospital
Adjunct Clinical Assistant Professor, Department of Physical Therapy
School of Health and Rehabilitation Sciences, MGH Institute of Health Professions
Boston, MA
Email: rwilcox@partners.org
Justin Jones P.T., D.P.T., O.C.S.: Assistant Clinical Professor, Simmons College
Physical Therapy Department
300 The Fenway Rm. S-320
Boston, MA
Email: justin.jones@simmons.edu
Elana J. Siegel, BA: Research Assistant
Harvard Shoulder Service, Brigham and Women’s Hospital
Boston, MA
Email: Esiegel1@partners.org
Laurence D. Higgins, M.D.: Chief of Sports Medicine
BWH Chief of the Harvard Shoulder Service
Orthopedic Surgeon, Department of Orthopedics
Brigham and Women’s Hospital
Boston, MA
Email: ldhiggins@partners.org
References
