| HOJ HOME | Chiefs Reports | Osgood Day | Scientific Articles | Alumni Association |
|
| Click here to visit our web site |
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
The main goals of the surgical treatment of idiopathic sco-liosis are the prevention of deformity progression through arthrodesis and correction of deformity sufficient to balance the spine in both the frontal and sagittal planes. Ideally these goals are accomplished while maintaining as much lumbar spinal flexibility as possible. Under the influence of Dr. John Hall, the group at the Children's Hospital developed such a motion sparing method using anterior spinal fusion and instrumentation. HISTORY Anterior spinal instrumentation
for the treatment of idio-pathic scoliosis was introduced in the 1960's
by Dr. Anthony Dwyer and colleagues 1 . His method offered a number of
advantages over existing posterior instrumentation systems, but the construct
composed of screws, staples, and a flexi-ble cable lacked rigidity and
often produced kyphosis. Unacceptable rates of pseudoarthrosis, implant
failure, and loss of lumbar lordosis have led to the abandonement of the
system when used alone for the surgical treatment of idiopathic scol-iosis
2,3,4,5. It has remained part of the armamentarium for the treatment of
neuromuscular curvatures, however, when used in concert with posterior
instrumentation. The Zielke system, which uses a flexible solid rod, had
similar problems 6-13 .
PATIENT SELECTION The ideal candidate
for short segment anterior instru-mentation is an adolescent or young
adult with a flexible idio-pathic thoracolumbar scoliosis and truncal
decompensation. For this type of deformity, traditional posterior instrumenta-tion
systems would necessitate fusion to the lower lumbar spine; anterior over-correction,
in contrast, may save two lum-bar motion segments. To produce a balanced
spine, both the lumbar curvature caudad and thoracic curvature cephalad
to the segments to be instrumented must be flexible enough to realign
following structural curve correction. The structural deformity must be
supple enough to be reversed by 10 degrees; in general this requires a
lumbar or thoracolumbar curvature of no greater than 60and a thoracic
curvature that corrects to 20 or less on the supine bending film. As anterior
instru-mentation has a tendency to produce kyphosis, thoracic hyper-kyphosis
is a relative contraindication to this procedure. SELECTION OF FUSION LEVELS Selection of proper fusion levels is essential for the suc-cess of the procedure. A set of guidelines based on the radi-ographic scoliosis series has been established specifically for the anterior apex overcorrection technique (Table 1) 15 . The instrumented segments include either three or four vertebra. When the levels of instrumentation as determined by the standing and supine methods differ, the longer of the two con-structs is chosen. TECHNIQUE Overcorrection of
the structural scoliosis, which is essen-tial to the success of the short
segment technique, places sig-nificant stresses on the instrumented portion
of the spine. Care is required to minimize these stresses by proper patient
positioning, destabilization through soft tissue resection, accurate hardware
placement, and controlled reduction maneuvers. The patient is placed in
the lateral decubitus posi-tion, the kidney rest is elevated, and the
operating table is flexed to improve the exposure. A transpleural, retroperitoneal
approach is made to the spine and the proper level is confirmed with intraoperative
radiographs. The segmental vessels over the vertebral bodies to be instrumented
are ligated and divided, and a subperiosteal exposure is performed. The
intervertebral discs are completely excised and the cartilaginous endplates
are resected. Currently, ISOLA anterior instrumentation is used. The screw
entry site is the mid-lateral aspect of the vertebral body. A staple is
placed, taking care to avoid penetration of the end discs, and the screw
tract is tapped through the far cortex. The appropriate length screw is
placed. It must be oriented par-allel to the end plates with one thread
engaging the opposite cortex. Each disc space is distracted with a laminar
spreader and a properly sized structural graft, currently a Harms cage,
is placed in the anterior aspect of the body slightly toward the concavity.
The disc space is the packed with morecelized auto-genous bone graft harvested
from the rib. The operating table is then straightened to allow spontaneous
correction.
A 1/4 inch rigid rod
is then cut to the correct length and contoured to provide the appropriate
lordosis and scoliosis over-correction, usually 20. The rod is placed
in the screws and rotated anteriorly toward a lordotic position, then
further rotat-ed until the desired degree of lordosis and reverse scoliosis
is obtained. The structural grafts are checked for position, and gentle
compression is applied toward the central screws to sta-bilize the construct.
Bone graft is added beneath the periosteal sleeve and over the disc spaces.
All screws are revisited and tightened. A chest tube is placed and the
wound is closed.
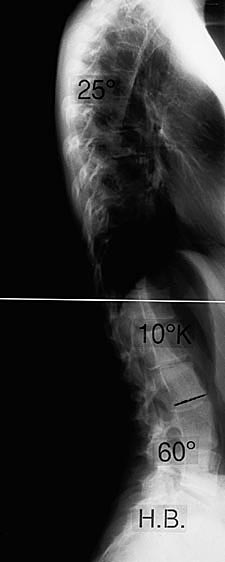
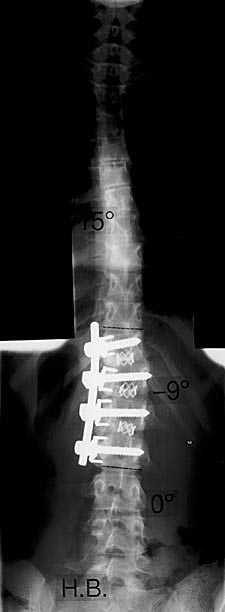
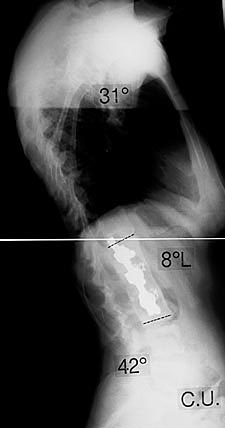
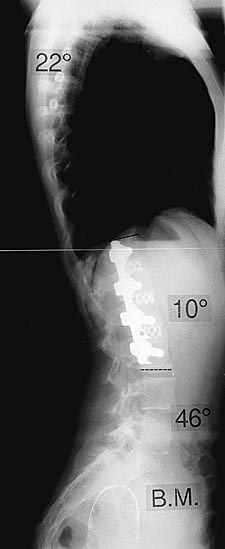
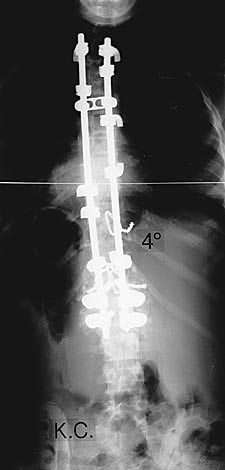
The patients are mobilized as tolerated postoperatively. Patients were instructed to wear a semi-flexible anterior open-ing Boston overlap brace when out of bed for the first three months post-operatively, though this is no longer a routine practice. Physical education is prohibited for six months and contact sports for one year. Follow up radiographs are taken at three, six, 12, and 24 months postoperatively. PATIENT REVIEW We have used the technique of short segment anterior instrumentation with Harms cages for over 3 years. Twenty-five patients have been followed for at least two years. All had adolescent idiopathic thoracolumbar or lumbar scoliosis. The average curvatures were approximately 50pre-operatively and were corrected 70%-80% on average. Over-correction of the instrumented segment was maintained at two years. The over-all lumbar lordosis was essentially unaltered and, most impor-tantly, the lordosis through the instrumented segment was maintained or improved. In general, most patients showed no loss of correction over time, though several had a deterioration due to an increase in the compensatory thoracic and subse-quent increased lumbar deformity. To date there have been no pseudoarthroses or other major complications. DISCUSSION The fate of the unfused portion of the lumbar spine below an instrumented segment is always a concern. Long-term studies that document increased low back pain following pos-terior instrumentation and fusion have involved the use of a straight Harrington rod with resultant loss of the normal lum-bar lordosis 19 . The newer segmental systems have not been in use long enough for comparison. We believe that increasing the number of spared lumbar motion segments distributes the stress across more levels and minimizes the risk of degenera-tive disc disease. Previous problems of high pseudarthrosis rates, instrumentation failure, and relative kyphosis through the instrumented segments seem to have been solved with the latest generation construct. While anterior spinal
fusion and instrumentation for tho-racolumbar and lumbar scoliosis has
been reported in the past, the short segment technique, which requires
overcorrection of the structural curvature, is nearly unique to Children's
Hospital 15,16,17,20 . This method, we believe, obtains excellent truncal
balance while preserving an additional lumbar motion segment. One criticism
of the technique has been the wedged disc space that sometimes occurs
beneath the instrumented segments 21 . Degenerative changes have been
reported to be associated with this finding by Kohler et al 16 . In that
series, however, Dwyer instrumentation was used, the short segment overcorrection
method was not performed, and the constructs extended into the lower lumbar
spine. Furthermore, the exam-ples cited by Kohler et al. showed staple
penetration of the disc spaces caudal to the fusion. To date we have not
seen wedg-ing associated with discomfort or degenerative changes 15,16
.
CONCLUSION We believe that preserving motion segments in the lumbar spine when performing surgical correction of lumbar and tho-racolumbar curvatures is critical, and thus we consider short segment anterior spinal instrumentation to be the treatment of choice for idiopathic scoliosis in properly selected patients. The method requires overcorrection or reversal of the structural curvature. The present technique, which utilizes a rigid rod, segmental screws, and anterior structural support in the form of mesh cages seems to have solved many of the problems that have been previously reported with this technique. |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| HOJ HOME | Chiefs Reports | Osgood Day | Scientific Articles | Alumni Association |
| References | |
| 1. | Dwyer AF, Newton NC, Sherwood AF. An anterior approach to scoliosis. Clin Orthop 1969:62:192-202. |
| 2. | Bridwell KH. Spinal instrumentation in the management of adolescent scoliosis. Clin Orthop 1997; 335:64-72. |
| 3. | Hsu LS, Zucherman J, Tang SC, Leong JCY. Dwyer instrumentation in the treatment of adolescent idiopathic scoliosis. J Bone Joint Surg Br 1982:64:536-41. |
| 4. | Kohler R, Galland O, Mechin H. et al. The Dwyer procedure in the treatment of idiopathic scoliosis. Spine 1990:15:75-80. |
| 5. | Luk KD, Leong JC, Reyes L, Hsu LC. The comparative results of treatment in idiopathic thoracolumbar and lumbar scoliosis using the Harrington, Dwyer, and Zielke instrumentations. Spine 1989:14:275-80. |
| 6. | Hammersby KW, Rodts MF, DeWald RL. Zielke instrumentation . Orthopedics 1988:11:1365-71. |
| 7. | Horton WC, Leatherman KD, Holt RT, Johnson JR. Results of Zielke instrumentation in the treatment of idiopathic thoracolumbar scoliosis. Orthop Trans 1966:10:33 |
| 8. | Kaneda K, Fujiya N, Satoli S. Results with Zielke instrunentation for idiopathic thoracolumbar and lumbar scoliosis. Clin Orthop 1986:205:195-203. |
| 9. | Kostuik JP, Carl A, Ferron S. Anterior Zielke instrumentation for spinal deformity in adults. J Bone Joint Surg Am 1989:71:898-912. |
| 10. | Lowe TG, Peters JD, Anterior spinal fusion with Zielke instrumentation for idiopathic scoliosis. Spine 1993:18:423-6. |
| 11. | Moe JH, Purcell GA, Bradford DS. Zielke instrumentation (VDS) for the correction of spinal curvature. Clin Orthop 1983:180:133-53. |
| 12. | Puno RM, Johnson JR, Ostermann PA, Holt RT. Analysis of the primary and compensatory curvatures following Zielke instrumentation for idiopathic scoliosis. Spine 1989:14:738-43. |
| 13. | Wojcik AS, Webb JK, Burwell RG, An analysis of the effect of the Zielke operation on s-shaped curves in idiopathic scoliosis. Spine 1989:14:625-31. |
| 14. | Hall JE. Current concepts review: Dwyer instrumentation in anterior fusion of the spine. J Bone Joint Surg Am 1981:63:1188-90. |
| 15. | Hall JE, Millis MB, Snyder BD. Short segment anterior instrumentation for thoracolumbar scoliosis. In: Bridwell KH, DeWald RL, eds. The textbook of spinal surgery. 2nd ed. Philadelphia:Lippincott-Raven, 1997:665-74. |
| 16. | Millis MB, Hey LA, Diminick MJ, Hall JE. Long-term follow up of patients with short-segment anterior instrumentation in the treatment of adolescent idiopathic thora-columbar scoliosis. Orthop Trans 1995-1996:19: 610. |
| 17. | Bernstein RM, Hall JE. Solid rod short segment anterior fusion in thoracolumbar scoliosis. J Pediatr Orthop Part B 1998:7:124-31. |
| 18. | Micheli LJ, Hall JE. The use of modified Dwyer instrumentation in anterior stabilization of the spine. Orthop Trans 1978:2:270. |
| 19. | Cochran T, Irstam L, Nachemson A. Long term anatomic and functional changes in patients with adolescent idiopathic scoliosis treated by Harrington rod fusion. Spine 1983:8:576-84. |
| 20. | Asher MA. Anterior surgery for thoracolumbar and lumbar idiopathic scoliosis. Spine:State of the art review 1998;12:701-11. |
| 21. | Johnston CE. Anterior correction of thoracolumbar and lumbar idiopathic scoliosis. Semin Spine Surg 9:150-163, 1997. |
|
TOP OF PAGE | HOJ HOME |
| HOJ HOME | Chiefs Reports | Osgood Day | Scientific Articles | Alumni Association |