| HOJ HOME | Chiefs Reports | Osgood Day | Scientific Articles | Alumni Association |
|
| Click here to visit our web site |
| ||||||||
|
INTRODUCTION Osteoarthrosis (OA) is thought to result from a failure of chondrocytes within the hyaline cartilage to maintain a balance between the synthesis and degradation of the cartilage matrix. The cause of this imbalance could be abnormal matrix, as seen in certain hereditary connective tissue disorders (e.g. type II procollagen gene COL2A1 mutation), or abnormal mechanics, as seen in slipped capital femoral epiphysis, developmental hip dysplasia (DDH), or Legg-Calve-Perthes disease, as well as post-traumatic conditions. In the hip, OA is most often caused by an anatomic deformity that leads to cartilage loading beyond what is tolerated by an intrinsically normal cartilage matrix (1, 2) . Specifically, acetabular dysplasia may account for a substantial proportion of hip OA in women (3) . In patients with DDH, partially dislocated or subluxed hips (where the femoral head is laterally displaced and articulates with the anterolateral margin of acetabulum) predictably lead to rapid onset OA (4, 5) . Murphy, et al. (6) retrospectively reviewed the development of OA in the contralateral hip of patients who underwent total hip arthroplasty for dysplasia. In this study, all patients with normal hip function who were followed to age of 65 had a center-edge angle of greater than 16°. Therefore, it appears that hip dysplasia of a certain magnitude may be a sufficient condition for development of OA by age 65. However, when hip subluxation and true acetabular dysplasia are separated. (4) , the rate of onset of OA has been difficult to predict using plain radiographic indices of dysplasia.
Currently, femoral and acetabular osteotomies are being performed with the goal of normalizing the stress distribution in the dysplastic hip and thus delaying or preventing the onset of OA. Retrospective studies looking at the end results of osteotomy have shown success rates ranging from 60-95% (7-12) . However, no long term follow up data beyond the fifth and sixth decades of life are available. Although symptomatic patients are substantially improved following osteotomy, the true efficacy of joint preservation surgery in preventing OA in the long term is unclear. It is difficult to obtain the 30-40 year follow-up data necessary to detect end-stage OA. Previously, there were no noninvasive methods to assess the amount of early degenerative changes in articular cartilage. Conventional radiography provides an indirect measure of cartilage integrity by showing the secondary bony changes. Only advanced OA will show changes detectable by radiographs. Similarly, computerized tomography (CT) scanning would provide three-dimensional anatomic detail, but only an indirect measure of articular cartilage integrity. Conventional magnetic resonance imaging (MRI) has fair to good correlation with arthroscopic surgery findings in detecting and assessing focal ulceration or full thickness cartilage loss. The earlier abnormalities of cartilage glycosaminoglycan (GAG) loss, edema, fibrillation, and fissur-ing, however, have not been reliably detected. Recently, MRI techniques for measuring GAG concentration in cartilage have been developed that have the potential to detect early degenerative changes. Our goal is to improve the management of hip dysplasia by determining preoperative factors, based on CT and/or MRI analysis, that would better predict successful outcomes after periacetabular osteotomy. CT or MRI analysis of the joint contact area and stress distribution would provide us with anatomic information that is thought to be important in the pathomechanics of osteoarthrosis. The gadopentetate dimeglumine (Gd-DTPA 2- ) enhanced MRI technique could provide the ability to detect early changes of osteoarthrosis in dysplastic hips before osteotomy, and determine whether these osteoarthritic changes can be reversed with normalization of hip mechanics. Given that the symptoms of dysplasia typically present in the third and fourth decades of life, the ability to detect early changes of OA in vivo would enhance the evaluation and development of new therapies. Furthermore, the combined analysis of clinical outcome measures as well as noninvasive measures of joint mechanics and matrix integrity could serve as a model to assess future therapies for OA such as cartilage transplantation, protease inhibitor treatment, and gene therapy. METHODS Patient selection and surgical indications All patients were skeletally mature. Patients with skeletal dysplasia, cerebral palsy, and known connective tissue disorders were excluded based on history and physical exam. Surgical indications include symptoms secondary to subluxation and osteoarthritic changes unresponsive to non-operative treatment for six months. Non-operative treatment includes any therapeutic intervention that does not correct the underlying abnormal joint mechanics. Clinical outcome measures Functional outcome was assessed using the modified Harris hip and Western Ontario and McMaster Universities Osteoarthrosis Index (WOMAC) scores. General health status was assessed using Medical Outcomes Study Short Form 36 (SF-36) questionnaire. In addition to a physical exam assess-ing hip range of motion, Cybex (Cybex International, Inc., Medway, MA) testing was used to quantify hip abductor function. Plain radiographic measures of dysplasia As outlined by Murphy, et al. (6) , center edge angle of Wiberg, acetabular index of depth to width, femoral head extrusion index, acetabular index of the weight bearing zone, and other parameters were measured using the anterior-posterior (AP) radiograph of the pelvis. Femoral head subluxation was assessed by determining whether Shenton's line was discontinuous by more than 5 mm 4 . For comparison with historical data, the acetabular angle of Sharp was also measured. In addition, the acetabular ventral inclination was measured from the faux profile view of the acetabulum (10) . Plain radiographic assessment of osteoarthrosis Various measures of osteoarthrosis severity have been used in the past. Most grading schemes are based on qualitative assessment of joint space and extraarticular features such as osteophyte formation, subchondral sclerosis, and subchondral cysts. Recent studies have suggested that grading of OA based on joint space narrowing and subchondral sclerosis may be the most sensitive measure of disease progression and clinical symptoms. Therefore, we measured the weight bearing joint space (11) , minimum joint space, and maximum thickness of subchondral sclerosis. Other features such as cyst formation or femoral head deformity were also noted. CT scan analysis to assess joint congruency and contact pressure CT scan was used to identify the acetabular rim and acetabular notch. These points were used to calculate the radius and center of a sphere that best represented the acetabulum. Three-dimensional iso-surface reconstructions of the acetabulum were created using the computerized modeling program AVS 5.0 (Advanced Visualization Systems, Waltham, MA). The lunate surface was discretized and moved 1.5 mm toward the center of the acetabulum to simulate a uniform 1.5 mm thick layer of cartilage. Load vectors representing three phases of gait, stair ascent, and three variations of stair ascent loads (adduction of the abducted hip, flexion of the extended hip, and external rotation of the neutral hip) were used to represent a wide range of activities of daily living (13) . At each surface patch, the contact pressure was calculated by dividing the load vector normal to each point by its surface area (14) . MRI analysis to assess GAG content of articular cartilage All MRI scans were performed using a 1.5 Tesla clinical scanner by General Electric or Siemens Medical System. A double dose (0.4 cc/kg of body weight) of Gd-DTPA 2- (Magnevist, Berlex Laboratories, Wayne, NJ) was infused and the patient made to walk _ hr prior to the scan. The gadolinium diffuses into the articular cartilage during this time and partitions according to the cartilage charge density, due to the negative charge of Gd-DTPA 2- . The gadolinium concentration in articular cartilage was then measured using MRI by measuring the enhancement of the cartilage T1 value. In-plane resolution of approximately 400-600 microns and slice thickness of 2-4 mm can be achieved. Four T1 maps using 5 7 T1 weighted images were obtained in approximately ten minutes of scanning time. PRELIMINARY RESULTS CT scan analysis of dysplastic hips and predicted stress distri-bution before and after osteotomy The predicted stress distribution was verified against measured pressure distribution in cadaveric and plastic pelves using Fuji pressure sensitive film (14) . The computer model can also be used to predict the relative magnitude of pressure in non-dysplastic cadaveric acetabula at prescribed locations. It is presumed that the computer model can predict maximum pressure relative magnitude and location in dysplastic hips, based on studies using plastic models of normal and dysplastic hips.
Preliminary MRI scan results illustrating the ability to detect degenerative changes in cartilage matrix in vivo In order to demonstrate that Gd-DTPA 2- enhanced images will detect variations in GAG concentration, sections of human femoral head, femoral condyle, and patella were obtained after total joint arthroplasty and imaged using Gd-DTPA 2- enhanced MRI. Histological sections of these samples were then stained with toluidine blue and correlated with the MRI images. As shown in Figure 2, there was a close correlation with the MR and histological images. Notably, there were anatomically intact regions that were depleted of GAG (as assessed by MR or histology) but showed no defects in non-contrast or proton density images, illustrating the improved sensitivity of Gd-DPTA 2- enhanced MRI (19) . The feasibility of
imaging in vivo has been demonstrated using intra-articular and/or intravenous
contrast administration of Gd-DTPA 2- 20 . The unenhanced images did not
show any evidence of an anatomic defect or substantial signal variation.
Images with non-ionic contrast agent did not show the image variations
present with the ionic contrast, lending further evidence to the interpretation
that the variations in image intensity (Gd-DTPA concentration) were due
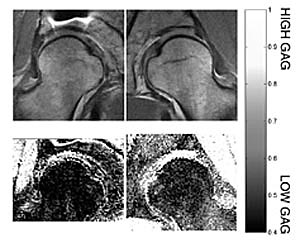
to the cartilage charge, or the GAG content. The images from a 33-year-old
woman with a symptomatic right hip are presented in Figure 3. X-ray and
proton density MRI scan (top panel) do not show any evidence of arthrosis.
However, charge density mapping of the articular cartilage (bottom panel)
do show a decrease in T1 value (~30%) in the symptomatic right hip, suggesting
early OA. These data suggest that this patient had an area of mor-phologically
intact cartilage with low GAG concentration, an area not seen with the
conventional MR imaging method.
Of note, the arthrogram effect of the intravenous Gd-DTPA- 2 - was sufficient to detect labral tears CONCLUSIONS This is a study in progress. We currently are obtaining clinical and radiographic data prior to periacetabular osteotomy. The same clinical and radiographic data will be obtained at one and two years after surgery. Our goal is to determine anatomic and cartilage biochemical factors that are predictive of surgical outcome. We believe that plain radiographic analysis is insufficient to estimate the joint contact pressures in dysplastic hips, and that three-dimensional assessment of the dysplastic hip morphology using CT or MRI is necessary. In vitro and in vivo work to date suggest that the Gd-DTPA-2 -enhanced MRI technique to measure charge density in articular cartilage is feasible and can be used as a clinical tool to detect early osteoarthrosis in the hip joint. |
||||||||
|
||||||||
| HOJ HOME | Chiefs Reports | Osgood Day | Scientific Articles | Alumni Association |
| References | |
| 1. | Aronson, J., Osteoarthritis of the young adult hip. Etiology and treatment. Instructional Course Lectures, The American Academy of Orthopaedic Surgeons., 1986. 35: p. 119-128. |
| 2. | Harris, W.H., Etiology of Osteoarthritis of the Hip. Clinical Orthopaedics and Related Research, 1986. 213: p. 20-33. |
| 3. | Solomon, L., Patterns of osteoarthritis of the hip. Journal of Bone and Joint Disease, 1976. 58B: p. 176-183 |
| 4. | Cooperman, D.R., R. Wallensten, and S.D. Stulberg, Acetabular Dysplasia in the Adult. Clinical Orthopaedics and Related Research, 1983. 175: p. 79-85. |
| 5. | Wedge, J.H. and M.J. Wasylenko,The Natural History of Congenital Disease of the Hip. Journal of Bone and Joint Surgery, 1979. 61B(3): p. 334-338. |
| 6. | Murphy, S.B., R. Ganz, and M.E. Muller, The Prognosis in Untreated Dysplasia of the Hip. Journal of Bone and Joint Surgery, 1995. 77A: p. 985-989. |
| 7. | Salter, R.B., G. Hansson, and G.H. Thompson, Innominate Osteotomy in the Management of Residual Congenital Subluxation of the Hip in Young Adults. Clinical Orthopaedics and Related Research, 1984. 182: p. 53-68. |
| 8. | Guille, J.T., et al., Triple Osteotomy of the Innominate Bone in Treatment of Developmental Dysplasia of the Hip. Journal of Pediatric Orthopaedics, 1992. 12: p. 718-721. |
| 9. | Faciszewski, T., S.S. Coleman, and G. Biddulph, Triple Innominate Osteotomy for Acetabular Dysplasia. Journal of Pediatric Orthopaedics, 1993. 13: p. 426-430. |
| 10. | Trousdale, R.T., et al., Periacetabular and Intertrochanteric Osteotomy for the Treatment of Osteoarthrosis in Dysplastic Hips. Journal of Bone and Joint Surgery, 1995. 77A(1): p. 73-85. |
| 11. | McCarthy, J.J., J.S. Fox, and A.R. Gurd, Gurd, Innominate Osteotomy in Adolescents and Adults Who have Acetabular Dysplasia. Journal of Bone and Joint Surgery, 1996. 78A: p. 1455-1461. |
| 12. | Kleuver, M., et al., Triple Osteotomy of the Pelvis for Acetabular Dysplasia. Journal of Bone and Joint Surgery, 1997. 79B(2): p. 225-229. |
| 13. | Cheal, E.J., M. Spector, and W.C. Hayes, Hayes, Role of Loads and Prosthesis Material Properties on the Mechanics of the Proximal Femur after Total Hip Arthroplasty. Journal of Orthopaedic Research, 1992. 10: p. 405-422. |
| 14. | Michaeli, D.A., S.B. Murphy, and J.A. Hipp, Comparison of Predicted and Measured Contact Pressures in Normal and Dysplastic Hips. Medical Engineering and Physics, 1997. 19: p. 180-186. |
| 15. | Hipp, J.A., et al. Relationships between Peak Pressures, Mean Pressures, Contact Areas and Loading in the Hip Joint. in 44th Annual Meeting of the Orthopaedic Research Society. 1998. New Orleans, LA. |
| 16. | Bashir, A., M.L. Gray, and D. Burstein, Gd-(DTPA) 2- as a Measure of Cartilage Degredation. Magnetic Resonance Medicine, 1996. 36: p. 665-673. |
| 17. | Bashir, A., et al. MRI of Glycosaminoglycan distribution in Cartilage Using Gd(DTPA)2- in vivo. in Fifth Annual Meeting of the International Society for Magnetic Resonance in Medicine. 1997. Berkeley, CA. |
| 18. | Boutin, R.D., et al., MR Imaging of Early Cartilage Degeneration in the Knee. American Journal of Radiology, 1997. 168(suppl): p. 58-59. |
| 19. | Bashir, A., M.L. Gray, and D. Burstein. Validation of Proteoglycan Measurements in Human Cartilage by MRI. in 44th Annual Meeting of the Orthopaedic Research Society. 1998. New Orleans. |
| 20. | Bashir, A., et al. Glycosaminoglycan in Articular Cartilage: In Vivo Assessment with Delayed Gd(DTPA)2--enhanced MR Imaging. Radiology, 1997. 205(2): p. 551-558. |
|
TOP OF PAGE | HOJ HOME |
| HOJ HOME | Chiefs Reports | Osgood Day | Scientific Articles | Alumni Association |