| HOJ HOME | Chiefs Reports | Osgood Day | Scientific Articles | Alumni Association |
|
|
||||
|
Introduction Aseptic loosening and osteolysis are presently two of the most common causes of failure of total joint replacements. In the United States, it is estimated that approximately 38,000 joint replacements are revised each year due to osteolysis and aseptic loosening alone. (1) Studies have shown that the cellular mechanisms involved in periprosthetic bone loss involve the interactions between particulate wear debris from materials used in the prosthesis and the surrounding macrophages. (2) Wear debris, primarily ultra-high molecular weight polyethylene (UHMWPE), tends to accumulate in the peri-implant tissues. Macrophages phagocytize the debris and are stimulated to release lysosomal enzymes as well as pro-inflammatory mediators, such as interleukin-1 beta (IL-1 ), interleukin-6 (IL-6), prostaglandin E 2 (PGE 2 ), and tumor necrosis factor-alpha (TNF-á ). These cytokines and mediators stimulate osteoclasts to resorb the surrounding bone, resulting in a painfully loose implant and the need for revision surgery. (3) Bisphosphonates are a class of drugs that inhibit osteoclastic bone resorption. Several bisphosphonate formulations have been approved by the FDA for clinical use to treat osteoporosis and Pagets disease. We have previously demonstrated that an oral bisphosphonate (alendronate) inhibited wear debris mediated osteolysis in a canine total hip replacement model. In this same study, we noted a marked increase in the amount of mineralized bone within the implant porosities in animals treated with alendronate. (4) This increase in bone mass (>100%) was in excess of that which would be normally expected if the osteoclastic bone resorption was inhibited and normal osteoblast bone formation continued. It is uncertain whether bisphosphonates affect osteoclasts only, or if bisphos-phonates also interact with osteoblasts. There are limited references regarding the bisphosphonate effect on osteoblast bone formation. Thus, the purpose of this study was to systematically investigate the potential anabolic effect of bisphosphonates on osteoblasts in an in-vitro model. |
||||
|
||||
|
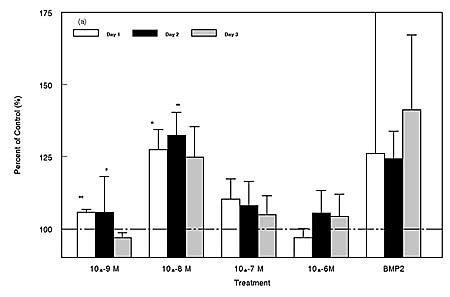
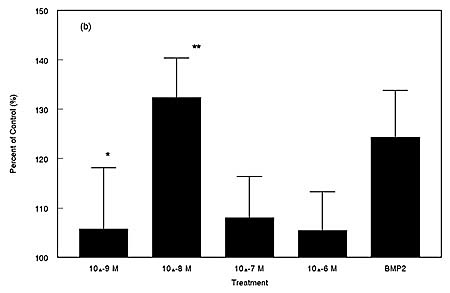
We studied both primary cell cultures of human trabecular bone cells (HTB cells); as well as a murine transformed osteoblast cell line, MC3T3-E1. (5) Following treatment with alendronate at varying concentrations and time periods, cells were assayed for proliferation and maturation by assessment of increased alkaline phosphatase release and osteocalcin. Autocrine effects, such as the upregulation of a bone mor-phogenic protein-2, (BMP-2) were also examined. Materials and Methods Human trabecular bone cells were obtained from femoral heads obtained during primary total hip arthroplasty. Bone fragments from the femoral head were digested with Collagenase P (1.2mg/ml,Boehringer Mannheim) and cultured in Dulbeccos modified Eagles medium: F12 (Biowhittaker) supplemented with 10% FBS and antibiotics/antimycotics (50U penicillin, 50ug streptomycin, Fungizone .; Gibco, NY). MC-3T3E1 clones are murine transformed osteoblast-like cells that have the potential to be stimulated to full osteoblast char-acteristics. MC-3T3E1 cells were cultured in alpha MEM (Biowhittaker) supplemented with 10% FBS, antibiotics (50U penicillin, 50ug streptomycin), and L-glutamine (200mM). Cell cultures were performed at 25 x 10 4 cells/ml with 95% humidity, 5% CO 2 , and 37 degrees C. After an overnight culture, alendronate was added at concentrations ranging from 10 -4 to 10 -13 M, and the cells were examined at 1, 2, 3, 5, 7, 9, and 21 days after treatment. All experiments were done in triplicate and repeated. We have used several techniques to measure the effect of bisphosphonates on osteoblasts. Cell proliferation was assessed by direct cell count as well as MTT ([3-(4,5- dimethylthiazol-2-yl)-2,5-diphenyltetrazolium bromide]) colorimetric assay. Osteocalcin, BMP-2, as well as osteoblast stimulatory factor/core binding factor a1 (cbfa1) was analyzed by RT-PCR, and alkaline phosphatase production evaluated by a bioassay (Sigma). Cell Proliferation - MTT Colorimetric Assay The conditioned medium was discarded and tetrazolium salt (MTT, Sigma, M-2128), was added to the cell layers (50mg/ml in 50 ul) and incubated for two hours at 37C. This time period permitted the intracellular conversion of MTT to formazan. The cells were then lysed, and the formazan was solubilized with acidic isopropanol at room temperature for 20 minutes. Color development was determined in a microtiter plate reader at a wavelength of 560nm. Cell Counting After an overnight culture, cells were treated with alendronate at various concentrations 10 -6 M to 10 -9 . This range of bisphosphonate dosage was previously determined to be effec-tive using the MTT colorimetric assay. Treated cells were cul-tured for 1, 2, and 3 days. Cells were trypsinized and counted with a hemacytometer using Trypan blue dye exclusion. Cell counts were done in duplicate and repeated in five cultures. Alkaline Phosphatase - Bio Assay The production of alkaline phosphatase by the osteoblas-tic cells after experimental treatments or controls was measured at 1,2, and 3 days. Osteoblastic cells were cultured in 12 well plates and grown to confluency. Alkaline phosphatase activity in the conditioned media was measured by its conver-sion of a colorless p-nitrophenylphosphate to a colored p-nitrophenol. The color change was measured at 405nm and the amount of enzyme determined by comparison with a standard curve. All experiments were conducted in duplicate. Data was analyzed using one-factor analysis of variance (ANOVA). Post-hoc "t-tests" were performed between groups of interest. Autocrine Effects Reverse transcriptase poly-merase chain reaction (RT-PCR) RT-PCR was used to identify any upregulation in BMP-2 and cbfa-1. At the end of the culture periods, media was discarded, cells washed with PBS, and 300ul Trizol(Gibco, NY) was added to each well and mixed well by hand agitation to ensure complete coverage of cell layer and lysis. RNA was extracted following established procedures and reverse tran-scribed to produce cDNA (1 st Strand cDNA Synthesis Kit, Boehringer Mannheim, Indianapolis, IN). The PCR [94C denaturing, 68C annealing, 72C extension; 35 cycles; one round; 250nM per 50ul MgCl 2 ] was carried out in a PTC-200 thermocycler(MJ Research; Worcester, MA). Results Cell Proliferation: Using the direct cell counting technique and the MTT colorimetric assay, we observed that alendronate was most effective on human trabecular bone cells at a concentration of 10 -8 M, and the effect was strongest at 48h after treatment.(Fig 2) At this concentration, the alen-dronate treatment resulted in a 32% increase in cell number over controls (p<0.01), comparable to BMP-2 treatment. In the transformed cell in-vitro model, alendronate was also most effective at 10 -8 M and the effect was noted at 72h after treatment. |
||||
|
||||
|
||||
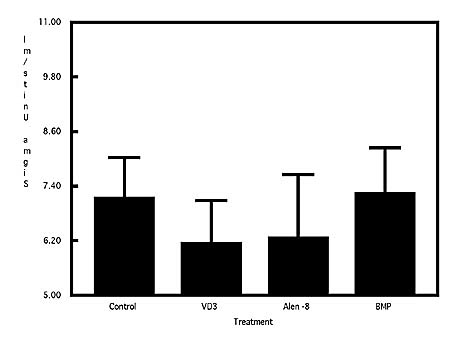
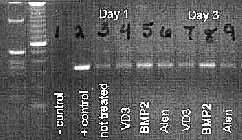
| Alkaline Phosphatase: The alkaline phosphatase production assay supported the cell proliferation data. During cell proliferation, the primary metabolic effort is the propagation of cells, whereas enzyme production would be secondary. Subsequently, the lowest levels of alkaline phosphatase in the conditioned media were detected 48 hours after bisphospho-nate treatment during which the highest cell proliferation occurred. The greatest increase in alkaline phosphatase was measured at seven days post-treatment. (Fig3) Preliminary studies using RT-PCR demonstrated that osteoblasts treated with alendronate stimulated gene expression of BMP-2 (Fig 4) as well as cbfa1 (data not shown). | ||||
|
||||
|
||||
|
Discussion While the ability of bisphosphonates to inhibit osteoclastic bone resorption has been well documented, their effect on osteoblasts is still under investigation. The findings in this study suggest that bisphosphonates can stimulate proliferation of osteoblastic cells and increase alkaline phosphatase levels. The cell proliferation data suggest that alendronate has an ana-bolic effect on osteoblastic cells. The bioassay for alkaline phosphatase supports the cell proliferation findings in that enzyme production is hindered and then upregulated depend ing on the phase of cell propagation. Furthermore, BMP-2 is a well-known osteogenic factor and can play a vital role in the upregulation of net bone formation. In this study, BMP-2 gene expression was noted after treatment with alendronate. Our preliminary findings suggest bisphosphonates may have an anabolic effect on osteoblasts by stimulating the differentiation and propagation of osteoblasts. In a clinical setting, oral therapy to enhance bone ingrowth into porous coated implants provides a convenient and flexible therapeutic approach. The results of this study suggest potential for the clinical use of bisphosphonates in the treatment of osteolysis. Additionally, enhanced bone ingrowth around the femoral component can improve implant stability, and retard the migration of debris to the bone-implant inter-face. Further research will help to clarify the two primary functions of bisphosphonates: inhibition of osteoclastic bone resorption and enhancement of bone formation. Acknowledgements We would like to thank Dr. Harris, Dr. Burke, Dr. Jasty, and Charlie Carter for generously providing the femoral head sam-ples. We would also like to thank David Cho for his assistance throughout this study. Jennifer Kenney was supported by the William H. Harris foundation. |
||||
|
||||
| HOJ HOME | Chiefs Reports | Osgood Day | Scientific Articles | Alumni Association |
| References | |
| 1. | Shanbhag AS, Rubash HE. Bisphosphonate therapy for the prevention of osteolysis in total joint replacements. Cur Opin Ortho 1998; 9:VI:81-7. |
| 2. | Wright TM, Goodman SB. Implant Wear: The future of total joint replacement, Rosemont, IL: American Academy of Orthopaedic Surgeons; 1996. |
| 3. | Chiba J, Rubash HE, Kim KH, Iwaki Y.The characterization of cytokines in the interface tissue obtained from failed cementless total hip arthroplasty with and without femoral osteolysis. Clin Orthop 1994, 300:304-12. |
| 4. | Shanbhag AS, May D, Cha C, Kovach C, Hasselman CT, Rubash H. Enhancing net bone formation in canine total hip components with bisphosphonates. Orthopaedic Research Society, abstract presented, 1999 |
| 5. | Shanbhag AS, Kenney J, Manning C, Flannery M, Rubash H, Harris W, Goldring S. Mitogenic effects of bisphosphonates on osteoblastic cells. Orthopaedic Research Society, abstract presented, 2000. |
|
TOP OF PAGE | HOJ HOME |
| HOJ HOME | Chiefs Reports | Osgood Day | Scientific Articles | Alumni Association |