| HOJ HOME | Chiefs Reports | Osgood Day | Scientific Articles | Alumni Association |
|
| |||||||||||||||||||||||
|
The Hand Surgery Service at Massachusetts General Hospital has treated a relatively large number of patients with ununited fractures of the humerus (7, 11, 15-18) . In treating these patients, we have learned how difficult it can be to obtain fixation that is stable enough to allow healing in the presence of poor bone quality. A number of specific techniques and implants have been developed to facilitate skeletal fixation of poor quality bone (15, 17). Background The Problem Fractures are more common in the elderly, due to loss of bone mineral density and the normal hormonal changes associated with menopause (6) . Metaphyseal fractures, such as those of the proximal and distal humerus are often associated with osteoporosis. In addition, many older persons are undernourished (4). Others have diminished bone density from limited activity. Older patients with ununited fractures may exhibit many of these factors and also lose bone from disuse, because their ununited limb is often painful and unstable (6). Fracture healing requires a good vascular supply, stability, and bone apposition (23). Nonunions occur when the blood supply is insufficient, when there is excess motion, or when there is soft tissue interposition or a bony gap. When a fracture of the humerus that has been treated non-operatively fails to heal, it is usually due to excess motion. Often a false joint, or synovial psuedoarthrosis develops at the fracture site and all attempts at healing are arrested (23).
To obtain healing, the surgeon must gain adequate fixation while preserving the vascular supply to the bone and surrounding soft tissue envelope. Any defects must be filled with autogenous cancellous bone graft. None of the currently available bone graft substitutes have been proven to be reliable for the treatment of ununited fractures. The Need to Address the Problem Achieving stable fixation in the presence of diminished bone quality, loose implants, and bony defects represents a substantial challenge (17, 19, 20) . In fact, some surgeons consider it risky to consider operative treatment in older patients with complex ununited fractures of the humerus. On the other hand, an unstable, ununited fracture can be extremely dis-abling and painful. The disability associated with an ununited fracture may be greater in an older person who is less capable of adapting to adversity. We have measured the disability associated with an ununited fracture of the humeral diaphysis in an older patient using the Disabilities of the Arm, Shoulder, and Hand (DASH) instrument and the Enforced Social Dependency Scale (ESDS) (17) . The DASH instrument consists of 21 questions about difficulty performing specific activities, 5 questions about symptoms, and 4 general health status questions. A higher score indictates greater dysfunction. The DASH scores for patients with ununited fractures of the humerus averaged 77 points, with the poorest score being 94 out of 100 points. These poor pre-operative scores were improved to an average of 24 points after operative treatment (17) . The Enforced Social Dependency Scale is an interview-based scale that was developed by nurses for the evaluation of patients who become dependent upon others for activities of daily living due to illness (1) . Although initially applied to med-ical illnesses such as heart failure and cancer, the ESDS is also appropriate in the evaluation of musculoskeletal problems. The scale has the ability to stratify among patients with very limited dependence upon others to those in a vegetative state. Pre-operatively, patients scored an average of 39 out of 100 points on a standardized scale. Scores improved to an average of 9 points after operative treatment, indicating substantial restoration of independent functioning (17) . These outcome instruments helped to quantify the impact that an ununited fracture of the distal humerus can have on a patients quality of life and ability to function independently. The dramatic improvement in scores for patients with unstable ununited fractures demonstrates the importance of devel-oping reliable means to gain stable fixation of the osteoporotic skeleton. Fixation Techniques
The use of orthogonal plates in the treatment of diaphy-seal fractures was unsuccessful in earlier applications (21) . However, those earlier studies were performed when subpe-riosteal dissection and plates with a large surface area in contact with the bone were used. It is likely that these techniques disrupted the blood supply to the bone and limited the biological capacity of the bone to heal (13) . With newer exposures which limit the elevation of muscle from bone and leave the perios-teum in place, and modern low-contact implants, such as the limited contact dynamic compression plate (LC-DCP; Synthes, Ltd., Paoli, PA) (13) , the PC-Fix (Synthes, Ltd.; Paoli, PA), and the so-called wave plate (2, 3, 14, 16) , it may be possible to take advantage of the biomechanical advantages of orthogonal plates without compromising the biological aspects of bone healing. Fixed-Angle Fixation Devices
Schuhli Nuts Nuts are occasionally applied to screws in an attempt to improve fixation. (Fig. 5B) The drawbacks of standard nuts include the need for an extensive, devascularizing exposure to apply the nut on the opposite cortex. In addition, the screw will still loosen and toggle, particularly with cyclic loading, if its threads do not engage the bone.
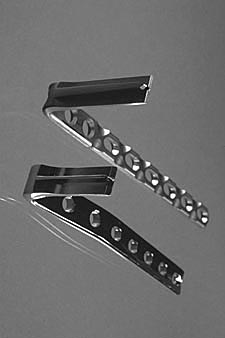
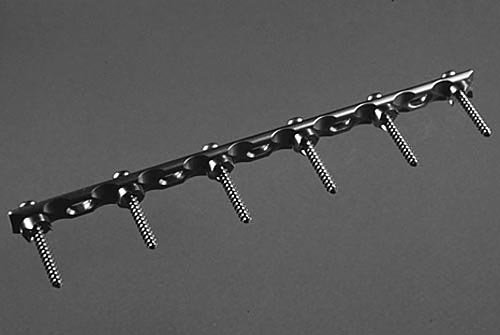
A new type of nutthe Schuhli nut 8-10 has been developed as a means to enhance the fixation of osteopenic bone. The Schuhli nut is applied underneath a plate, between the plate and bone on the near cortex.(Fig. 6) It locks into the plate so that when a screw is fully threaded in to the plate it becomes a fixed-angle device. Even if the screw has limited engagement or purchase in the bone, it still provides stability just as the blade of a blade plate does. In addition, the nut has spikes that increase the friction between the plate and the bone. The nuts raise the plate off of the bone, thereby decreas-ing its contact area and making it a more limited contact implant.
Results We have used these principals, techniques, and implants in the treatment of ununited fractures of the humerus at various levels and for various types of fractures. Ununited Fractures of the Distal Humerus The senior author (JBJ) has treated over 40 patients with an ununited fracture of the distal humerus. A large percentage of these patients were women over 60 years of age. Many of them had synovial nonunions, and some had intra-articular nonunions. Older patients with ununited fractures of the distal humerus are treated with a combination of three plates( 7) : the medial plate wraps around the medial epicondyle, providing for an increased number of screws in the medial fragment with the most distal screw oriented orthogonal to the more proximal screws; the lateral column is secured with two orthogonal platesone directly posterior and the other directly lateral on the lateral column. The elbow capsule is released through the fracture site, the fracture site is debrided to bleeding bone, and autogenous bone graft is applied (7, 11) . Post-operatively, patients are splinted in extension, and active, gravity-assisted elbow mobilization is initiated the day after surgery. Healing was achieved in each case with an average of 95 degrees of ulno-humeral motion ultimately obtained, in some cases after a secondary elbow capsular release. Ununited Fractures of the Humeral Diaphysis We recently published the results of the operative treatment of 22 older-aged patients with unstable ununited fractures of the humeral diaphysis (17) . Plate length averaged 76% of the length of the humerus. Modifications of standard plating technique included the use of a blade plate in 13 patients, Schuhli nuts in 6 patients, replacement of a loose 4.5 millimeter cortical screw with a 6.5 millimeter cancellous screw in 12 patients, augmentation of a loose 4.5 millimeter cortical screw with cement in 2 patients, and use of an allograft strut to enhance screw fixation in 2 patients. In addition, 5 patients had bony defects addressed with a second intramedullary plate in 2 patients, and a wave plate in 3 patients. Healing was achieved in all but two patients. The fixation remains stable in the two patients with persistent fracture lines, suggesting fibrous union. The functional improvements were dramatic both objectively and subjectively with 77% of patients achiev-ing good or excellent results and the improvements based on the outcome measures documented above (17) . Ununited Fractures of the Proximal Humerus In a combined series with Michael McKee, MD in Toronto, we have reviewed the treatment of 25 patients with ununited fractures of the proximal humerus using blade plate fixation (18) . About two-thirds of these patients were older than 60. Only two fractures failed to unite, but the fixation remained stable in each case. Again, marked functional improvements were recorded both subjectively and objectively. Fractures of the Humerus Associated with a Bony Defect In a combined series with Dr. Rene Marti in Amsterdam, Dr. Richard Sanders in Birmingham, and Dr. Jaime Quintero in Columbia, we have studied the results of treatment of 15 patients with ununited fractures of the humerus associated with a bony defect at the fracture site (16) . When a defect is present as a result of debridement of an originally open fracture, a subsequently infected one, a synovial nonunion, or loose implants with devascularized bone, we have used the so-called wave plate (2, 3, 14, 16) . Wave plate osteosynthesis consists of a plate contoured to stand away from the bone about _ to 1 centimeter at the fracture site. Bone graft is applied both beneath the plate and in the fracture site. The wave contour improves the access of the blood supply from the surrounding musculature to the underlying bone grafts. It also distributes bending stresses over a greater area of the plate, thus limiting the potential for fatigue failure under cyclic loading. Finally, itfacilitates restoration of a tension band function of the plate, since the lateral translation of the bending moment that results from the contour of the plate distributes compressive forces to the near cortex. Restoration of this cortex by incorporation of the bone grafts placed underneath the plate leads the plate to act as a tension band, thereby improving the mechanics of the plate-bone construct. All but one of the patients treated with wave plate osteosynthesis healed. Conclusions The operative treatment of ununited fractures of the humerus presents a formidable task as a result of the poor bone quality that is often encountered in this patient popula-tion. However, the extreme disability associated with a painful, unstable nonunion mandates that we address this challenge. A number of recent developments in the implants and techniques for the fixation of poor quality bone have proven useful in the treatment of our patients with ununited fractures of the humerus at all levels, including those with bony defects. We continue to address the need for stable fixation of poor quality bone both in the care of our patients, as well as in the biomechanics laboratory. |
|||||||||||||||||||||||
|
|||||||||||||||||||||||
| HOJ HOME | Chiefs Reports | Osgood Day | Scientific Articles | Alumni Association |
| References | |
| 1. | Benoliel JQ, McCorkle R, Young K.Development of a social dependency scale. Res Nurs Health 1980; 3:3-10. |
| 2. | Blatter G, Weber BG.Reosteosynthesis in delayed fracture healing of the femoral shaft using a waved-plate. AO Bulletin 1986; 1:3-5. |
| 3. | Blatter G, Weber BG.Wave plate osteosynthesis as a salvage procedure. Arch Orthop Trauma Surg 1990; 109:330-333. |
| 4. | Glowacki J.Advances in skeletal biology. Havard Orthopaedic Journal 1999; 1:63-66. |
| 5. | Helfet DL, Hotchkiss RN. Internal fixation of the distal humerus: a biomechanical comparison of methods. J Orthop Trauma 1990; 4:260-264. |
| 6. | Järvinen M, Kannus P. Injury of an extremity as a risk factor for the development of osteoporosis. J Bone Joint Surg 1997; 79A:263-276. |
| 7. | Jupiter JB, Goodman LJ. The management of complex distal humerus nonunion in the elderly by elbow capsulectomy, triple plating, and ulnar nerve neurolysis. J Should Elbow Surg 1992; 1:37-46. |
| 8. | Kassab SS, Mast JW, Mayo KA. Patients treated for nonunions with plate and screw fixation and adjunctive locking nuts. Clin Orthop Rel Res 1998; 347:86-92. |
| 9. | Kolodziej P, Lee FS, Patel A, et al. Biomechanical evaluation of the Schuhli nut. Clin Orthop Rel Res 1998; 347:79-85. |
| 10. | Matelic TM, Monroe MT, Mast JW. The use of endosteal substitution in the treatment of recalcitrant nonunions of the femur: report of seven cases. J Orthop Trauma 1996; 10:1-6. |
| 11. | McKee MD, Jupiter JB, Toh CL, Wilson L, Colton C, Karras KK. Reconstruction after malunion and nonunion of intra-articular fractures of the distal humerus. J Bone Joint Surg 1994; 76B:614-621. |
| 12. | McKee MD, Miranda MA, Reimer BL, et al. Management of humeral nonunion after the failure of locking intramedullary nails. J Orthop Trauma 1996; 10:492-499. |
| 13. | Perren SM. The concept of biological plating using the limited contact dynamic compression plate (LC-DCP): Scientific background, design and application. Injury 1991; 22:1-41. |
| 14. | Ring D, JB JB.Wave plate osteosynthesis in the upper extremity. Tech Hand Upper Ext Surg 1997; 1:168-174. |
| 15. | Ring D, JB JB. Fixation techniques for osteopenic bone: the experience with ununited fractures of the humerus. Scientific exhibit presented at the 66th annual meeting of the American Academy of Orthopaedic Surgeons., Anaheim, California, 1999. |
| 16. | Ring D, Jupiter JB, Quintero J, Marti R. Wave plate osteosynthesis in the upper extremity., Poster presented at the 10th annual meeting of the English speaking orthopaedic associations of the world., Auckland, New Zealand, 1998. |
| 17. | Ring D, Perry B, Jupiter JB. The functional outcome of the operative treatment of ununited fractures of the humeral diaphysis in elderly patients. J Bone Joint Surg 1999; 81A:177-189. |
| 18. | Ring RD, B BP, Jupiter JB. The use of a blade plate to treat ununited fractures of the proximal humerus., American Shoulder and Elbow Surgeons Specialty Day, New Orleans, Louisiana, 1998. |
| 19. | Rosen H. The management of non unions and malunions in long bone fractures in the elderly. In: Zuckerman JD, ed. Comprehensive care of orthopaedic injuries in the elderly. Baltimore: Urban and Scwartzenberg, 1990:489-512. |
| 20. | Rosen H. The treatment of nonunions and pseudarthroses of the humeral shaft. Orthop Clin N Amer 1990; 21:725-742. |
| 21. | Teipner WA, Mast JW. Internal fixation of forearm fractures: double plating versus single compression (tension band) plating A comparative study. Orthop Clin N Amer 1980; 11:381-391. |
| 22. | Törnkvist H. The strength of plate fixation in relation to the number and spacing of bone screws. J Orthop Trauma 1996; 10:204-208. |
| 23. | Weber BG, Cech O. Pseudarthrosis. New York: Grune and Stratton, 1976. |
|
TOP OF PAGE | HOJ HOME |
| HOJ HOME | Chiefs Reports | Osgood Day | Scientific Articles | Alumni Association |