| HOJ HOME | Chiefs Reports | Osgood Day | Scientific Articles | Alumni Association |
|
| Click here to visit our web site |
| |||||||||
|
Introduction The health care industry is changing rapidly in response to managed care and cost containment pressures. Health care networks are increasingly turning to information technology to help them survive and thrive in this challenging marketplace. In particular, a growing number of pioneering organizations are implementing Electronic Medical Record (EMR) systems. In last year's Healthcare Information and Management Systems Society leadership survey (1) of healthcare executives and managers, 57% of the 993 respondents indicat-ed that they have already begun to install an EMR system or have plans to do so, while 11% of the respondents said they already have fully operational EMR systems. Physicians are increasingly
realizing the significant positive impact that an EMR can have on their
practice. Studies are being published every year that demonstrate the
value of using healthcare information systems. Benefits include streamlined
office workflows, more complete documentation, better compliance with
regulations, improved patient care, reduced errors, increased patient
and provider satisfaction, and significant cost savings from reduced chart
pulls and transcription use. Additionally, insurers and government regulators
are requiring physicians to provide more extensive documentation regarding
patient care. These events are encouraging physicians to turn to computer
systems to assist them with their daily clinic workflow.
EMR Benefits One of the most fundamental benefits of an EMR is the ability to access legible and complete patient charts quickly from any location within the network. This substantially reduces the need for chart pulls in many cases, resulting in a substantial cost savings, and eliminates the need for retrieval of paper charts. In addition, EMR systems can be designed to permit secure offline access and editing, for example, to download selected patient charts to a laptop for completion at home. Much of my residency and early practice was devoted to the management of the sequelae of poliomyelitis. It is difficult to describe the anxiety and precautions taken in communities in the years of polio epidemics, and the number of children left with permanent disabilities. The disappearance of this scourge has to be one of the defining events of this period. Much the same can be said about tuberculosis as evidenced by the absence of the dedicated sanitoria, which were so prevalent at mid-century. Whether either of these diseases could reappear will depend on compliance with immunization programs on the one hand and development of resistant strains and poor public health measures on the other. Using an EMR can reduce transcription-related expenses, but more importantly, it eliminates the turnaround time required for transcription. Notes entered directly into the system are immediately available and can be viewed by others on the system, or they can be printed and sent to other providers outside of the system. The ability to produce a referral note immediately after the patient's visit is also of great importance to the referring doctor, and can allow for more immediate feedback on the utility of certain care protocols. Documentation for follow-up visits can be completed quickly using an EMR that has a "copy forward" feature. This feature allows you to start with a copy of your last visit note written for this patient and complete the current visit note by simply making edits to the prior note. This can be a tremen-dous timesaver in cases where there has been little change since the previous visit, and allows the physician to complete his documentation faster than by using traditional dictation. A large component of any clinic practice is patient education. There is now a large, growing library of patient-oriented health education material available in software form for all specialties. Having the material in an online computer database makes it much easier to locate specific handouts and elimi-nates stocking or storage issues. The online database can be easily searched for a specific topic, and the materials often can be customized or annotated specifically for your patient. Each orthopedist can have their own branded educational materials, which ensures that the patients are provided with physician-specific materials that are current and accurate. Clinical data in electronic form obtained from using an EMR in clinic practice can be invaluable for the academic practitioner who is interested in doing retrospective clinical research. Research queries can now be performed by computer in seconds using data collected by the EMR. For example, with online patient data collected from an EMR, it would be easy to obtain answers to queries such as, What percentage of patients in my practice present with a meniscal tear that is refractory to all non-operative modalities and requires opera-tive intervention? Orthopedic-specific EMR needs The majority of EMR systems available today have been designed for ambulatory-based primary care practices. Orthopedic surgeons have different information needs that present unique challenges to the implementation of an EMR system. Several of these orthopedic-specific needs are described below. Orthopedic practices tend to have a higher volume and more rapid pace of appointments when compared to other clinical departments. A portable computing platform is prefer-able in this environment to allow the orthopedist maximum mobility so he can quickly move in and out of exam rooms while completing his documentation. Using portable devices also makes it easier for fellows and clinic staff to help con-tribute to portions of the visit documentation, as the device can be shared among staff. Primary care providers see patients with a wide range of clinical problems, so they must have a large array of templates that can cover any possible presenting complaint. On the other hand, orthopedists tend to have quick appointments with a smaller set of highly structured problems, so they need a smaller number of templates, but with more specialty-specif-ic details. For example, a knee physical exam performed by an orthopedist includes more specialized tests and maneuvers than that of a primary care physician. In addition, Evaluation and Management (E/M) coding requirements for single-organ system exams are different than for the general multi-organ system exam typically performed by a primary care provider, and it is important to be sure that the EMR software can cor-rectly code these orthopedic specialty exams. Orthopedists also tend to have a large amount of "routine" documentation, such as operative reports, post-operative fol-low- up notes, office procedure notes, and referral letters. With a properly set-up collection of pre-written templates, this type of routine documentation can actually be done faster with an EMR than with dictation. Arthroscopy, total joint arthroplasty, and many other procedures lend themselves well to the pro-duction of a templated operative report. Doing this requires an initial time investment to set up custom templates for each purpose, but a small initial time investment can save hours of time in the future. A structured operative note also provides an appropriate base of data to assist in the development of out-come metrics. Although orthopedists tend to write fewer medication orders than primary care physicians do, they do write a signif-icant number of other types of orders, such as imaging orders, requests for durable medical equipment, and referrals to ancil-lary services such as physical therapy. An orthopedic-specialty EMR implementation should be able to automate these com-mon tasks as an additional timesaving feature for the surgeon. Evaluation and Management Coding Partners Department of Orthopaedic Surgery initially began this project as a method to help staff surgeons with E/M coding compliance. The financial stakes with E/M coding are high since there have recently been several highly publicized cases where the Office of the Inspector General (OIG) from the Department of Health and Human Services has conducted audits of healthcare institutions and uncovered violations resulting in millions of dollars in fines and penalties. The Health Care Financing Administration (HCFA), which has responsibility for administration of Medicare, publishes the official Evaluation and Management Documentation Guidelines. The latest version of the HCFA Documentation Guidelines is a 48-page manual published in 1997 which con-tains a comprehensive set of rules detailing exactly what ele-ments are required to be documented in order to bill at a given Level of Service. These very onerous guidelines are difficult to comply with using traditional non-computerized systems, but it can be done relatively easily using a computer-based system. By per-forming office visit documentation online using templates, accurate coding levels can be obtained using an automated E/M "coding wizard" that analyzes the note and automatically generates an appropriate E/M code. The current version of the HCFA Documentation Guidelines are currently under-going review amidst concerns from practicing physicians about the complexity of the guidelines, and a new version of the Documentation Guidelines is expected to be released some time later this year. Although there will be some adjustments to the coding rules, HCFA is still insisting upon some form of point scoring system, so it is likely that software tools will still be needed for the foreseeable future to help physicians comply with these documentation guidelines. Implementation Last year, Dr. James
Herndon, chairman of Partners Department of Orthopaedic Surgery, asked
us to begin investigating options of software systems that could help
surgeons comply with E/M coding guidelines. Using information from various
sources, we compiled a comprehensive vendor matrix analysis comparing
the features and functions of EMR products from over 30 different commercial
vendors. Our key requirements included an E/M coding wizard that would
accommodate an orthopedics specialty, support for wireless portable client
devices, and the ability to easily create custom templates for orthopedic-specific
problems. After extensive analysis, we chose the Compendia EMR system
from Data Critical (Houston, TX, www.physix.com). We felt that this product
would adequately meet our needs at a reasonable cost per provider. The
Compendia EMR is a fully functional EMR system with the ability to interface
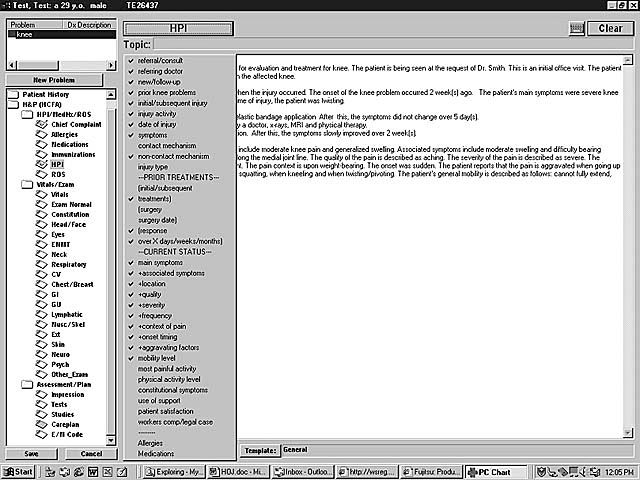
to scheduling and billing systems. Compendia uses a template-driven system
for con-structing chart notes. Users are presented with a series of cas-cading
drop-down menus with choices that generate sentences when selected (Figure
1). The templates are customizable by the end user and allow notes to
be written in a range of styles. The Compendia system includes an advanced
E/M Coding Wizard that automatically computes the appropriate Level Of
Service code based on the note you have written, which then requires confirmation
by the individual orthopedist.
We also performed an extensive review of hardware client devices for this project. We required a Windows 9x platform with both a pen-based touch screen and a keyboard. We even-tually chose the Fujitsu B2130 Lifebook (Fujitsu, San Jose, CA), which is an Intel Celeron 400MHz ultra-light laptop with 64MB of RAM, a 6.4GB hard drive, a 10.4" touch screen, and a nearly full-sized keyboard (Figure 2). For wireless connectivi-ty, we use the Aironet 4800 series product (Aironet, Akron,OH), which uses direct sequence spread spectrum and oper-ates on the 2400MHz-frequency spectrum. It has a data throughput rate of 11 Mbps, which gives us response times that are comparable to wired Ethernet speeds. The Aironet wireless system was Partners Information Systems' preferred vendor for wireless networking, and we felt that it was important to use the same wireless system as the rest of the organization so that our providers will eventually be able to roam seamlessly throughout the hospital while remaining connected to the wireless network.
Challenges Implementing an EMR system involves a fundamental change in the way an orthopedist runs his or her clinic, interacts with patients, and communicates with clinic staff. It is important to set the proper expectations up front. As with any new workflow, there is a learning curve and it will take some time and effort to master the system. Initially, physicians will not be as efficient using the computer system, but over time they can become faster using the EMR than using traditional dictation. Experience from others has shown that it can take several months to achieve a critical mass of user acceptance of any new EMR system. It is important to identify a number of physician champions for the project. The physician champion should be a practicing physician from each subspecialty area within the department who will remain closely involved with all phases of the project. The champion should be someone who is well respected among other physicians in the department. The physician champions play an important role in leading tem-plate development groups and in demonstrating the use of the EMR system. A good EMR training plan is critical to the success of an EMR implementation. For physicians, one-on-one training is preferred so that training can be individualized and specific questions and concerns can be addressed. Although this approach requires more training personnel, it is much more effective than group sessions. Training should be scheduled shortly before go-live since new users tend to forget things eas-ily if they don't use the information right away. It is also impor-tant to realize that the most important learning occurs during the first few weeks of actual usage of the application with real patients, so this underscores the importance of having trainers on site full time during the first few weeks of go-live. One of the big challenges to our implementation at Partners was the multiple locations involved. Even for our small pilot of about 6 orthopedists, the clinics were spread out among 5 physical locations across metropolitan Boston, with several clinics at Massachusetts General Hospital, and some at Brigham & Women's Hospital. This necessitated special con-siderations for the wireless network and printer setup. This factor also made it more challenging to assemble the pilot physicians for user meetings. Future Directions In the next phase of this project, we will begin work on interfaces between Compendia and our scheduling and billing systems. This will allow patient information to flow seamlessly between computer systems. After the pilot with the knee specialists has been implemented, we plan to focus on template development for other body systems. The eventual goal is to develop a base set of templates that covers each orthopedic specialty area, including the hip, spine, pediatric orthopedics, shoulder, hand/wrist, and foot/ankle. As we develop these templates, we will bring orthopedists on board who specialize in these areas. We also plan to solicit user feedback so we can make rec-ommendations to our vendor for enhancements to improve the system for orthopedics practices. Our vendor has indica-ed a willingness to work with us to enhance the software and adapt it for our needs. Conclusion Adoption of Electronic Medical Record systems is likely to continue to increase rapidly in the future. Physicians in all specialties are beginning to understand and appreciate thebenefits of using computers in their clinic practice. Implementation of an EMR in an orthopedic practice is partic-ularly challenging and requires considerations to orthopedic-specific needs. Our initial experiences have been positive. As we continue to refine and customize the system, we are hope-ful that we will be able to demonstrate significant improve-ments in patient care and cost savings with the usage of an EMR system in the Partners Department of Orthopaedic Surgery. |
|||||||||
|
|||||||||
| HOJ HOME | Chiefs Reports | Osgood Day | Scientific Articles | Alumni Association |
| References | |
| 1. | The 10th Annual HIMSS Leadership Survey, Healthcare Information and Management Systems Society, http://www.himss.org/survey, accessed 3-30-2000 |
|
TOP OF PAGE | HOJ HOME |
| HOJ HOME | Chiefs Reports | Osgood Day | Scientific Articles | Alumni Association |