| HOJ HOME | Chiefs Reports | Osgood Day | Scientific Articles | Alumni Association |
|
| Click here to visit our web site |
| |||||||
|
The emergence of improved
computer databases and mature outcome assessment instruments have allowed
us to address a long-standing need -- the development of a registry that
prospectively collects both clinical and radiographic data from multiple
institutions. Such a registry can perform at least two essential functions.
First, it can enable the prospective evaluation of clinical and radiographic
results and match them to the patients' assessments of specific procedures.
Second, it can serve as a resource for post-market surveillance of implants,
and by so doing, act as an early warning system for possible implant failures.
The first task for
the acceptance of such a registry is to demonstrate that data collection,
analysis, and presentation can be performed efficiently and at a reasonable
cost. The Hip Society is taking the first steps toward the implementation
of a North American Hip Registry. This endeavor is being funded by the
Council on Research of the American Academy of Orthopaedic Surgeons, the
Hip Society, and the Orthopaedic Research and Education Foundation. Its
specific aim is to establish the efficacy of a registry by performing
two initial studies that yield publishable results in one year. In this
paper, we discuss the two studies that comprise the first phase of implementation
and discuss the methodological, technological, administrative, and confidentiality
issues regarding the project.
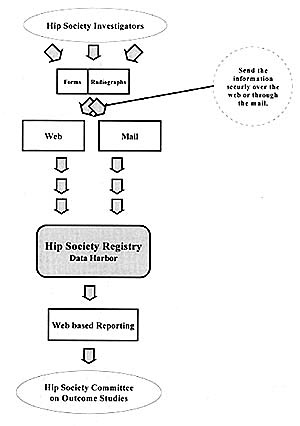
Structure of the Registry Participating Hip Society members submit data on scannable paper forms or securely over the Internet to an independent data management center, Data Harbor, Inc. (Figure 1). Members also transmit digital radiographs securely over the Internet or send plain films to the center. The Hip Society Committee on Outcome Studies determines the data elements, time points, radiographic views, reporting requirements, and specific studies for the Hip Society Registry. Because an independent data manage-ment company manages the hard-ware, software, and data at a central location, a personal computer and web browser are all the orthopaedic surgeon needs to enter and access his/her data. This arrangement provides potential cost savings as well as professionals with specific expertise to do the work while allow-ing orthopaedic surgeons and their staff the time to focus on their core competencies. Study of the incidence and outcome of dislocation after total hip arthroplasty (THA) in ten North American teaching centers. For our initial pilot study, we chose to study the problem of dislocation following total hip arthroplasty (THA) for the following reasons. (1) The complication is unambiguous and easily identified. (2) Most dislocations occur within the first three months following arthroplasty. (3) By collecting data for six months on consecutive THAs performed at the contribut-ing centers, analysis of those data will be sufficient to deter-mine trends and stimulate hypothesis-driven research ques-tions regarding dislocation. While there is abundant literature on the causes and treatment of dislocation following THA, there has not been a systematic inquiry into the combined effects of variables such as surgical technique, patient risk factors, radiographic analysis, and surgeon volume. Furthermore, there have been no reports regarding of the impact of this complication on patient perception of outcome and satisfaction. In this study, we will determine how accurately the operating surgeon can predict subsequent dislocation at the time of surgery, and how accurately we can predict dislocation after reviewing the radiographs. We hope to determine what patient and surgical fac-tors are most likely to lead to dislocation. Most importantly, we hope to determine the impact of dislocation on patients' lives, and the impact of any subsequent procedure(s) performed as a result of dislocation. Centers will collect data from patients preoperatively and from operating surgeons at the time of surgery. Each center will also provide three radiographs for the study: a preoperative AP Pelvis, a postoperative AP Pelvis, and a postoperative Cross-Table Lateral. Centers will send the two forms (including the implant stickers) and three radiographs to the independent data management center. The data management center will enter the forms and radiographs in to the database and collect follow-up data from patients via mail. In January 2000, data collection began in ten centers for this study. Recruitment will continue for six months; we expect a minimum of one hundred consecutive patients from each center, providing a study cohort of at least one thousand patients. Study of the incidence of revision THA in ten North American teaching centers. There are no current post-market surveillance mechanisms in place in North America to evaluate survival following THA. We plan to identify the types and longevity of implants revised during one year. These data should provide a rich source of hypothesis-driven research questions. Data collection began in ten centers in January 2000. Recruitment will continue for one year; we expect each center to contribute one hundred consecutive patients, providing a study cohort of one thousand failed arthroplasties. Centers collect data from operating surgeons at surgery and send this form to the independent data management cen-ter for entry into the database. Upon completion of this study, we expect to learn the inci-dence of revision surgery in these ten centers. We will learn the reasons for revision, the length of time from implantation to revision, and the specific components removed. By tracking the removed components, we hope to determine if there areany component-specific design or surgical issues that lead these components to fail either earlier or more frequently than expected.
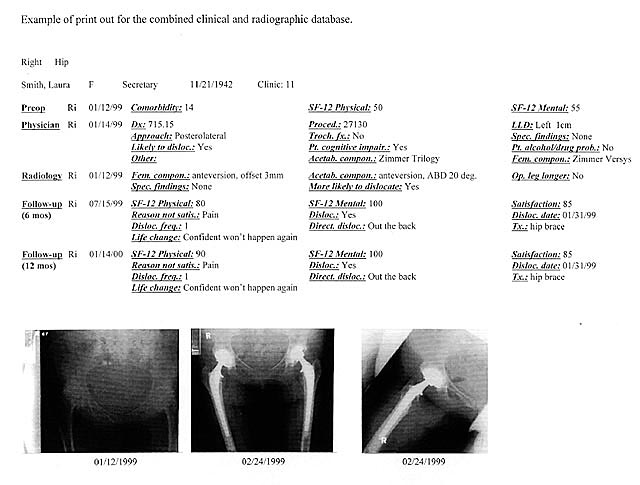
Administrative Issues Minimizing the length of data collection forms, particu-larly those forms completed by surgeons and staff, is a critical factor in the success of this project. The Hip Society Registry has created single-page physician forms that can be completed in a minimal amount of time (less than two minutes). Still, each center must make its own individual assessment of how to integrate data collection into its daily routine. The follow-ing questions must be addressed. When will the physician complete this form? How will it be delivered to him/her? How will the staff person retrieve it? When will the patient be given a form? Who will give it to him/her? Who will retrieve it from him/her? Who will answer his/her questions? There are also other administrative issues relating to ongoing physician acceptance. What can the Hip Society Registry provide to the practitioner so he/she will continue to participate? By presenting combined clinical and radiographic data in a useful format, such as the x-ray card (Figure 2), and by providing benchmarking comparisons, the Registry will provide physicians with ongoing value. We hope and expect these features will lead to continuing participation beyond a single study of interest. Confidentiality Issues Patient confidentiality is a critical concern when storing data and radiographs at a location outside of the hospital. Patient consent must also be acquired before contributing data for research and releasing data and radiographs to a central database. Institutional Review Board (IRB) approval is likely required when participating in a multi-center registry such as the Hip Society Registry. Conclusion These first studies evaluating the problems of dislocation and revision following THA will provide the Hip Society Registry with a foundation of two thousand patients and three thousand radiographs. If successful in the longer term, this registry will provide a wealth of information for collaborative research in the years to come. It will provide another impor-tant function, by its ongoing tracking of revisions, as an early warning system of implant failures. It will also provide an opportunity for cost savings through the outsourcing of indi-vidual center's joint registries. Acknowledgments We gratefully acknowledge the support of the Maurice E. Müller Foundations of North America and Switzerland. We thank Ben Albert of Data Harbor for his contributions to this manuscript. |
|||||||
|
|||||||
| HOJ HOME | Chiefs Reports | Osgood Day | Scientific Articles | Alumni Association |
| References | |
| 1. | Ware J Jr; Kosinski M; Keller SD. A 12-Item Short-Form Health Survey: Construction of Scales and Preliminary Tests of Reliability and Validity. Med Care 1996 Mar; 34(3): 220-33 |
| 2. | Katz JN; Phillips CB; Poss R; Harrast JJ; Fossel AH; Liang MH; Sledge CB. The Validity and Reliability of a Total Hip Arthroplasty Outcome Evaluation Questionnaire. J Bone Joint Surg Am 1995 Oct; 77(10): 1528-34 |
| 3. | Harrast JJ; Hong G; Greenaway L; Eggli S; Poss R; Sledge CB. A Comparison of the SF-36 and SF-12 General Health Status Measures: The Cases of Total Hip and Total Knee Replacement. American Academy of Orthopaedic Surgeons Annual Meeting 1997 Feb. |
|
TOP OF PAGE | HOJ HOME |
| HOJ HOME | Chiefs Reports | Osgood Day | Scientific Articles | Alumni Association |