| HOJ HOME | Chiefs Reports | Osgood Day | Scientific Articles | Alumni Association |
|
| Click here to visit our web site |
| |||||||||||||||||||||||||||||
|
Introduction Since its introduction in Sweden more than 10 years ago, autologous chondrocyte implantation (ACI) has generated substantial interest in the orthopaedic community (1) . The high level of interest in ACI is likely due to the troublesome nature of the articular cartilage lesions that it is designed to treat. Once destroyed, articular cartilage will not regenerate, and lesions may progress to osteoarthritis. Furthermore, these lesions frequently result in pain, swelling, and mechanical symptoms such as locking and catching, dramatically reducing a patient's quality-of-life. The basic science investigation of the mechanisms of healing and repair started at our institution in 1992, and the first patients were treated in March 1995. To date, the author has treated 160 patients. This article reviews data on 101 patients who underwent treatment between March 1995 and November 1998, with 59 patients having greater than 6 months follow-up. Science Background and Time Course of Healing Several basic science
investigations have elucidated the mechanisms and time course of healing
of autologous chon-drocyte implantation. In a rabbit study evaluating
autologous chondrocytes labeled with tritiated thymidine, the in-vitro
cultured chondrocytes were noted to be responsible for a large portion
of the repair tissue in-vivo 2 . Further studies deter-mined that the
repair tissue from ACI was superior to periosteum alone. Canine studies
from our institution have demon-strated that there are several stages
to the healing process (4-6) . These stages include (1) the proliferative
stage (0-6 weeks), which is characterized by a primitive cell response
with tissue fill of the defect; (2) the stage of transition during which
a type II collagen framework is produced along with the proteogly-cans
that form the matrix. The tissue is not firm nor well inte-grated, and
is "milkable" when probed with an arthroscopic nerve hook; and (3) a remodeling
and maturation phase that occurs over time, lasting as long as two years,
as matrix proteins crosslink and stabilize in large aggregates, and the
colla-gen framework reorganizes to integrate into the subchondral bone
and form arcades of Benninghoff. By 4-6 months, the tis-sue has usually
firmed up, is no longer "milkable" but has a "putty-like" consistency.
It is well integrated to underlying bone and adjacent cartilage. Patients
will start to experience good symptom relief during this period. However,
the process of tissue maturation that begins during the remodeling stage
continues long after this point. Excessive activity during this remodeling
stage may cause repair tissue degeneration. Hence, the concept of a time
course of healing is critical dur-ing ACI rehabilitation.
Practical Algorithm for Cartilage Repair The author's approach is to use arthroscopic debridement of unstable cartilage flaps for lesions less than 1 cm 2 in low demand patients and a gentle abrasion technique in high demand patients. For lesions of 1-2 cm squared , a marrow stimulation technique (abrasion, drilling or microfracture) or an osteochon-dral grafting technique (Mosaicplasty TM ,OATS TM , or CORR TM ) may be used in high demand patients. For lesions that are larger than 2 cm squaredor have failed alternative treatment options, ACI would be used as a primary treatment. For lesions greater than 10 cm squared where the articular cartilage loss and morphology of the condyle is distorted, fresh osteoarticular allograft is most likely to succeed. The rationale for this algorithm is discussed elsewhere (7-10) . Indications for ACI Autologous chondrocyte implantation has been approved by the FDA for the treatment of a symptomatic full thickness chondral injury of the weight-bearing femoral articular surface in a physiologically young patient who is compliant with the rehabilitation protocol. (11) The results of ACI for the treatment of chondral injuries of the patella and tibia have not been as good as those of the femoral weight bearing condyles and trochlea. Results of ACI for treatment of osteochondritis dis-secans (OCD) have also been successful . (12) The author has also used ACI successfully as a revision chondral surgery for chronic, symptomatic lesions unresponsive to alternative treat-ments, and as a first line treatment for symptomatic defects greater than 2cm squared . ACI is not FDA approved as a treatment for osteoarthritis, that is bipolar chondral injuries with radiographic evidence of joint space narrowing with weight bearing. Therefore, preoperative weight bearing radiographic evidence of joint space narrowing of >50%, osteophyte formation, subchondral bony sclerosis or cyst formation are all considered contraindications to ACI. Rosenberg 45° bent PA views are helpful to assess tibia-femoral loss of cartilage in flexion .(13) Axial alignment weight bearing and merchant views are necessary to assess tibiofemoral or patellofemoral malalignment. MRI does not have high sensitivity (14) in determining the extent of a chondral injury or subtle chondromalacia changes. Normal radiographs with arthroscopic assessment are the gold standard for determining whether a symptomatic patient is a candidate for ACI.
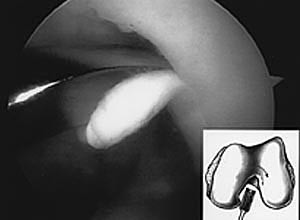
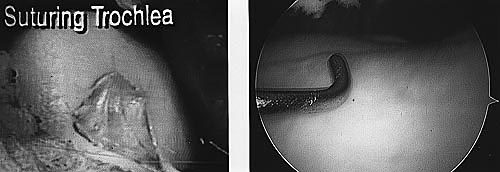
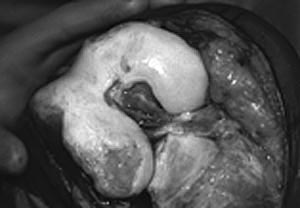
If a lesion is considered appropriate for ACI, then a biopsy site for cartilage procurement must be determined. The lateral intercondylar notch may be biopsied, (author's preferred site, see Figure 1). Approximately 200-300mg of articular cartilage is required for enzymatic digestion and cell culturing. This is roughly a cartilage surface 5mm wide by 1cm in length containing 200,000-300,000 cells. These cells will be enzymatical-ly digested and grown to approximately 12 million cells per 0.4cc of culture media per implantation vial. Following in vitro expansion of cells some 3-5 weeks later, a suitable number and volume of cells will be grown to accommodate the defect size required. At this time, second stage open implantation may occur. Surgical Implantation of Autologous Chondrocytes The steps in open implantation include arthrotomy, radical lesion debridement, (leaving subchondral bone intact) periosteum procurement, periosteum fixation, periosteum watertight integrity testing, autologous or allogeneic fibrin glue sealant, chondrocyte implantation, wound closure, and rehabilitation. The technique has been described in detail previously (1,15,16) . Surgical Correction of Factors Predisposing to Chondral Injury Several predisposing factors to chondral injuries must be assessed so that they may be either corrected in a staged or concomitant fashion with ACI. Tibiofemoral malalignment, patellofemoral malalignment, and ligamentous or bone insufficiency must be assessed prior to definitive cartilage cell reimplantation. When varus or valgus malalignment is associated with a medial or lateral condyle injury respectively, then a corrective osteotomy is paramount to the success of chondral implantation. This can be done either in a staged or concomitant fashion. If corrective osteotomy is done concomitantly, stable fixation must be obtained at the time of osteotomy so that continuous passive motion (CPM) and early active range of motion may be pursued immediately postoperatively. Otherwise, a staged reconstruction should be performed. Patello-femoral mal-tracking combined with a trochlear or patellar chondral injury requires careful pre-operative assessment with physical examination and CT or MRI imaging tech-niques. Tibial tubercle osteotomy combined with soft tissue realignment to ensure proper tracking is key to successful graft healing. Congenital trochlea dysplasia is an uncommon factor contributing to patello-femoral maltracking. Preoperative CT scan demonstrating flattening of the convex superior trochlear capturing entry point best assesses this problem. Treatment is by surgical trochleoplasty combined with patellar realignment as necessary .(16) Cartilage repair in the face of anterior cruciate ligament (ACL) insufficiency may jeopardize a newly regenerating cartilage graft. Staged or concomitant ACL reconstructive surgery should be performed with the goal of preventing shear forces and instability episodes from damaging a healing graft. ACL rehabilitation is modified to exclude closed chain resisted strengthening exercises (leg presses or squats) until 9 months after combined surgery to prevent excessive compressive load to the chondral repair site. When bony deficiency is present such as after an osteochondral fracture or osteochondritis dissecans, the depth of the bony lesion should be assessed preoperatively through conventional radiography, tomography and/or arthroscopy. Osteochondritis dissecans defects, on average, are 6-8mm deep including cartilage and bone. These often do well using ACI alone without bone grafting. However, defects greater than 1- 2cm deep require preliminary bone grafting and healing prior to cartilage resurfacing. This may be performed arthroscopically or by open technique. An interval of 6-9 months is required before second stage articular resurfacing to allow the cancellous bone graft to incorporate. In this way, a new subchondral bone plate' is formed, and minimal (if any) bleeding occurs prior to chondrocyte implantation. In addition, a patient occasionally becomes asymptomatic after bone grafting secondary to fibrocartilage repair of the overlying chondral defect, thus obviating the need for further surgery. Clinical Series Following approval
by the human ethics committee, a prospective evaluation of ACI-treated
patients was undertaken in March 1995. Patients were implanted in the
manner described above with ex-vivo cultured chondrocytes injected beneath
a periosteal patch secured with re-absorbable sutures and fibrin sealant
(1, 15). Post-operative rehabilitation included non-weight bearing and
use of continuous passive motion for 6-8 hours/day for 6 weeks, followed
by progression to full weight bearing at 4 months. Patients were restricted
from in-line impact activities (e.g., running) for 9-12 months, and cut-ting
sports for at least 14-18 months.
Demographic data, prior surgical history, defect characteristics, and baseline evaluation including completion of 4 validated rating scales was collected. Follow-up evaluation was completed using these same 4 metrics at 6, 12, 18, and 24 months, and at yearly intervals thereafter. Standardized rating scales included the SF-36 (Short Form 36 item quality-of-life questionnaire), WOMAC (Western Ontario and MacMaster Universities Osteoarthritis Index), KSS (Knee Society Score), and the modified Cincinnati Knee Rating System. Data were collected by a research assistant independent of the operating surgeon using standardized case report forms, and statistical analysis was conducted by an unbiased third party (AACT-Abt Associates Clinical Trials, Cambridge, MA.
Results SF-36 overall physical health scores improved at each follow- up visit, reaching significance at 24 months (p <0.001). Mental health overall scores improved at each visit, reaching significance at 36 months (p=0.024), with vitality and social functioning components demonstrating the greatest improve-ment. The overall WOMAC score, as well as physical function and pain subscores, showed significant improvement at 24 months (p <0.01 in each case). Similarly, outcomes at 24 months evaluated by the Knee Society Knee Score demonstrated improvement (p<0.001).Changes in the Knee Society Function Score did not reach sig-nificance (p = 0.16). Results from the Cincinnati Knee score reflected significant improvement at 12 and 24 months (p<0.001). Management of Complications To date there have been no intra-articular joint infections following ACI in our patients. Minor superficial wound infections have occurred, as well as complications related to open arthrotomy. The most common postoperative problem seen is periosteal hypertrophy. This usually manifests 3 to 7 months after surgery (at second look arthroscopy) as a proliferative hypertrophic periosteal healing response. Patients may present with new onset catching from a previously smooth track-ing knee with symptoms of pain and effusion. If this occurs, activity level should be decreased and arthroscopic shaving is recommended to resolve the prominent overgrowth. Periosteal problems may occur as often as 25% of the time. In most cases, the catching response settles and the patient remains asymptomatic. Intra-articular adhesions are rare except in the case of large intra-articular periosteal patches taken from the femur, which can lead to intra-articular fibrosis. If this occurs, adhesions are best released with arthroscopic electrocautery, elec-troablation, or shaving of adhesions. After intra-articular adhesions are released, the grafts are visualized to ensure that there are no adhesions to the grafts. Gentle manipulation then confirms adequate release. Discussion Rationale for the treatment of cartilage damage in younger patients depends on a thorough understanding of the predisposing factors for the chondrosis and the stage of disease. Implantation with autologous cultured chondrocytes allows for resurfacing of larger defect areas, with good to excellent results in 90% of patients with isolated lesions of the femoral condyle. Patellar lesions may be successfully treated, but strict attention must be given to correction of malalignment. Results in patients with tibial and salvage lesions are encouraging, however these results should be viewed with caution due to the small number of patients with two year follow-up. At present, ACI involves an open technique with the inherent disadvantages of adhesions and prolonged recovery. However, these disadvantages must be weighed against the procedure's ability to produce a hyaline-like tissue with greater durability than the fibrocartilaginous tissue that is produced by traditional marrow-stimulation techniques. For this reason, it is recommended that the treating surgeon match the treatment procedure to patient demographics and expectations, and the location and size of the chondral lesion. Based on the available literature, algorithms have been published (7-10) recommending that ACI be reserved as first-line treatment for high-demand patients with large lesions (> 2cm squared ) and as revision therapy in patients with lesions of all sizes who have failed alternative techniques. |
|||||||||||||||||||||||||||||
|
|||||||||||||||||||||||||||||
| HOJ HOME | Chiefs Reports | Osgood Day | Scientific Articles | Alumni Association |
|
||||||||||||||||||||||||||||||||||
|
TOP OF PAGE | HOJ HOME |
| HOJ HOME | Chiefs Reports | Osgood Day | Scientific Articles | Alumni Association |