| HOJ HOME | Chiefs Reports | Osgood Day | Scientific Articles | Alumni Association |
|
| Click here to visit our web site |
| |||||||||
|
Historical Background Pigmented villonodular synovitis (PVNS) is most often a monoarticular disease affecting patients in their third or fourth decade. The knee joint is most commonly affected and due to the large recesses in the knee, patients often present late after the disease has insidiously spread to extraarticular sites around the knee. Up to 50% of patients report a history of asso-ciated trauma. (18) Although Chassaignac was the first to describe the lesion in 1852, it was Jaffe who proposed the name of pigmented vil-lonodular synovitis in 1941. (11) Jaffe thought the histology showed a fibrous stroma, pigment deposition, histiocyte infiltrate, and giant cells within the synovial membrane, hence the term pigmented villonodular synovitis. (11) Granowitz et al., (7) fur-ther classified PVNS according to whether there was a discrete lesion (localized) or a diffuse lesion. Confusion still exists as to the etiology of PVNS and whether it is a true neoplasm or a reactive inflammatory process. (3,5,11,18,22,23,24) Without a clear understanding of the patho-physiology of the disease, treatment remains controversial. It is widely accepted that surgical resection often cures the localized form of PVNS with low rates of recurrence. In contrast, treatment of the diffuse form (DPVNS) remains controversial with high rates of recurrence and substantial morbidity after surgery. (2,3,4,6,9,16,19,20,22,25,28) In our opinion, arthroscopic
and limited open techniques (4,20,28) provide inadequate exposure of the
knee joint, particularly postero-laterally and in the region of the popliteus
tendon. Furthermore, most reports of treatment of DPVNS have small numbers
of patients, often collected over a number of years with more than one
joint included. (1,2,8,8,12,16,18,22) To the best of our knowledge, no
reports in the literature contain large numbers of patients with DPVNS
of the knee, with adequate preoperative staging, and long-term clinical
or MRI evaluation. (15,17,21)
Materials and Methods Over 40 consecutive
patients referred to the Brigham & Women's Hospital between 1990 and 1999
with histologically confirmed DPVNS of the knee were interviewed and examined,
and their clinical records reviewed. Outcome data was gath-ered from 38
patients who were referred after one or more failed arthroscopic synovectomy
procedures to determine pre-and post-arthroscopic-synovectomy function.
(20) The average age of the patients at index arthroscopy was 31.7 years
(range 11 to 65 years). We also reviewed the records of 39 patients who
underwent a standardized combined posterior and anteri-or open synovectomy
by one surgeon (GWB) at our hospital. These patients were retrospectively
assigned to one of three groups: group I received surgery alone (6 patients),
group II had surgery and intra-articular radiation synovectomy using dysprosium-165
( 165 Dy) (27 patients), and group III had surgery and external beam radiation
(6 patients) performed three months postoperatively. Group I patients
were more recent patients who were treated after the senior author (GWB)
no longer favored the use of Dysprosium-165. Group II patients were mostly
treated during a period when Dr. Clement Sledge and Sonya Shortkroff 26
were experimenting with Dysprossium-165 to treat DPVNS of the knee. Group
III patients had post-operative MRI findings suggestive of residual disease
larger than 5 millimeters. Outcome was assessed according to the clinical
rating system of The Knee Society, with assignment of a maximum of 100
points for knee scores and functional scores. (10)
Magnetic resonance
imaging was used in all cases to identify sites of DPVNS infiltration
preoperatively, to confirm adequate tissue removal at three months post-operatively
prior to radiation therapy, and to follow patients annually thereafter.
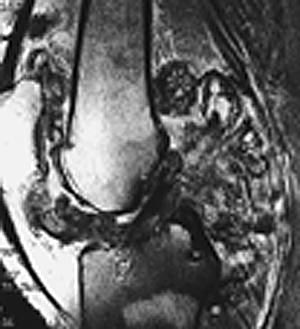
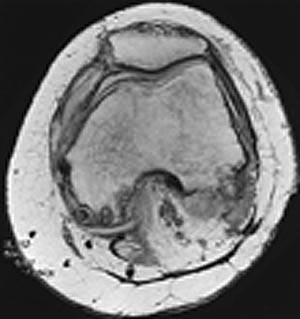
Surgical Technique Open synovectomy was performed as a single staged procedure with the posterior approach being undertaken first. An S-shaped incision with the proximal limb based postero-laterally allows adequate exposure of the peroneal nerve proximally. The distal limb placed on the postero-medial side allows extensile exposure and excision of any large semimembranosus bursa that may be present. Extra-articular sites of DPVNS included the semimembranosus bursa, beneath both heads of the gastrocnemius muscles, posterior to the posterior cruciate ligament, the popliteus sheath, superior to the posterior aspects of the medial and lateral femoral condyles as well as previous arthroscopy portals. The posterior dissection included mobilization of both the medial and lateral heads of the gastrocnemius, exploration of the popliteus sheath, and detachment of the peripheral attachments of the menisci. A standard paramedian arthrotomy was used to expose the anterior aspect of the joint. Over three liters of irrigation was used during the posterior and anterior approaches to reduce the risk of leaving residual DPVNS tissue. Postoperative management included epidural anesthesia for 48 hours with continuous passive motion (CPM) immediately post-op and for three weeks for 1.5 hours each day. Weight bearing as tolerated with a pair of crutches is allowed immediately post-op. Results The most common presenting symptoms were pain and swelling. Approximately half recalled trauma to the affected knee prior to being diagnosed with DPVNS, but less than 10% recalled trauma after they were diagnosed with DPVNS. Many patients had associated diagnoses such as medial and lateral meniscus tears, Baker's cyst, torn anterior cruciate ligament, and recurrent patella dislocation. More than half of the patients had one or more procedures after the first arthroscopic syn-ovectomy without eradication of their disease.(Fig. 1 A-B) Most patients reported some improvement of their symptoms fol-lowing arthroscopic synovectomy. However, all patients rated their symptoms and function as worse than prior to arthro-scopic synovectomies at the latest follow up of about four years (range 0.25 to 19.5 years) after the first arthroscopic synovec-tomy. Most patients lost some degree of knee motion longterm. The mean post-operative score for pain, function, range of motion, and synovitis was substantially worse than the preoperative scores in all patients who had recurrence after arthroscopic synovectomy. In contrast, the patients who had the standardized open antero-posterior synovectomy had an average of a twenty-point improvement in Knee Society Scores for pain and function at an average of 4.5 years following the index procedure. Most had substantial improvements in post-operative knee motion. Most patients considered themselves improved at the latest follow up. There was less than 20% incidence of recur-rence on MRI.(Fig. 2 A-B) A majority of these patients had no clinical signs of a recurrence. Recurrence rate was zero in group I, and slightly higher in groups II and III. Three patients with early postoperative stiffness required closed manipulation under anesthesia before regaining almost full range of motion. Four patients with advanced preoperative degenerative arthri-tis continued to have pain postoperatively necessitating a total knee replacement. Discussion Recent reports of "complete" arthroscopic synovectomy suggest good results following arthroscopic synovectomy for DPVNS of the knee. (20,28) However, none of these reports include both preoperative and post-operative MRI assessment to docu-ment the extent of the disease or to follow the patients after arthroscopy. When MRI confirms extra-articular disease, arthro-scopic synovectomy, even in the best hands, is unlikely to eradicate extra-articular disease in hard to reach locations such as the popliteus sheath, medial and lateral gutters, behind the posterior cruciate ligament, and the infra-patellar fat pad. In the absence of MRI assessment, no comment can be made regard-ing the true extent of the disease in any series. Nevertheless, studies by Zvijac et al., (28) and Ogilvie et al., (20) have confirmed that arthroscopic synovectomy can provide short-term relief of symptoms associated with DPVNS of the knee. This conclusion was borne out in the present study with most patients experi-encing some subjective improvements in their symptoms in the short-term following arthroscopic synovectomy. It has been reported that failure to eradicate DPVNS of the knee is associated with poor outcomes and a need for further surgery. (2,18,19,20) We have found similar results, with over half the patients who underwent arthroscopic synovectomy requiring one or more additional procedures. This finding is especially concerning in light of recent reports that have suggested that PVNS is a neoplastic proliferation of synovial fibroblasts and histiocytes. (3,5,22,23) Thus, failure to eradicate DPVNS by limited open techniques or arthroscopic synovectomies may predispose patients to locally disseminated disease, major symptoms, and subsequent loss of function. Furthermore, it is theoretically possible that arthroscopy and surgical manipulation could result in dissemination of the tumor beyond the joint space. Conclusion A critical review of prior reports and our experience does not support routine arthroscopic synovectomy alone or in combination with limited open synovectomy for the treatment of DPVNS of the knee, especially when the disease is also pre-sent in extra-articular sites. It is our current recommendation to treat any patient presenting with advanced DPVNS of the knee with the combined anterior and posterior open synovec-tomy technique, post-operative CPM, and weight bearing as tolerated. Extensive pre-operative degenerative joint disease predisposes patients to a poor result. Patients should be fol-lowed preoperatively and postoperatively with MRI assessment. We could not confirm the benefits of Dysprossium-165 or external beam radiation to treat DPVNS of the knee, since recurrences occurred following both types of treatment. The results of our study suggest that complete synovectomy is the procedure of choice to decrease the risk of recurrence of DPVNS of the knee. Arthroscopic or limited open techniques or radiotherapy may reduce the amount of DPVNS tissue and associated symptoms in the short term, but will not eradicate the disease. In contrast, an extensile open surgical approach allows excellent visualization for removal of intra-and extra-articular DPVNS tissue with an acceptably low complication rate. We continue to use arthroscopy for pre- or post-operative diagnostic biopsies or treatment of early primary or residual disease following open synovectomy. Our current practice is to assess patients with MRI pre-operatively, three months post-operatively, and annually thereafter. |
|||||||||
|
|||||||||
| HOJ HOME | Chiefs Reports | Osgood Day | Scientific Articles | Alumni Association |
| References | |
| 1. | Atmore, WG, Dahlin DC, and Ghormley RK.: Pigmented villonodular synovitis. A clinical and Pathologic Study. Minnesota Med., 39:196-202, 1956. |
| 2. | Byers PD, Cotton RE, Deacon OW, Lowy M, Newman PH, Sissons HA, Thomson AD. The diagnosis and treatment of pigmented villonodular synovitis. J. Bone and Joint Surg. 50-B:290-302, May 1968. |
| 3. | Choong PFM, Willen H, Nilbert M, Mertens F, Mandahl N, Carlen B, Rydholm A. Pigmented villonodular synovitis, monoclonality and metastasis-a case for neoplastic origin? Acta Orthop Scand 66(1):64-68, 1995. |
| 4. | Flandry FC, Hughston JC, Jacobson KE, Barrack RL, McCann SB, Kurtz DM. Surgical treatment of diffuse pigmented villonodular synovitis of the knee. Clin. Orthop. 300:183-192, 1994. |
| 5. | Fletcher JA, Henkle C, Atkins L, Rosenberg AE, Morton CC. Trisomy 5 and trisomy 7 are nonrandom aberrations in pigmented villonodular synovitis: Confirmation of trisomy 7 in uncultured cells. Genes chromocomes Cancer 4(3):264-266,1992. |
| 6. | Friedmann M, Schwartz EE. Irradiation therapy of pigmented villonodular synovitis. Bulletin of the Hospital for Joint Diseases 18:19-32, 1957. |
| 7. | Granowitz SP, D'Antonio J, Mankin HJ.: The pathogenesis and long-term end results of pigmented villonodular synovitis.Clin. Orthop. 114:335-351,1976. |
| 8. | Granowitz SP, Mankin HJ. Localized pigmented villonodular synovitis of the knee. J. Bone and Joint Surg. 49-A:122-128,January 1967. |
| 9. | Hamlin BR, Gavan DP, Trousdale RT, Morrey BF. Total knee arthroplasty in patients who have pigmented villonodular synovitis. J. Bone and Joint Surg. 80-A:76- 82,January 1998. |
| 10. | Insall JN, Dorr LD, Scott RD, Scott WN.: Rationale of the Knee Society clinical rating system. Clin Orthop., 248:13-14, 1989 |
| 11. | Jaffe HL, Lichtenstein L, Sutro CJ.: Pigmented villonodular synovitis, bursitis, and tenosynovitis of the knee. A discussion of the synovial and bursal equivalents of the tenosynovial lesion commonly denoted as xanthoma, xanthogranuloma, giant cell tumor, or myeloplaxoma of the tendon sheath, with some consideration of this tendon sheath lesion itself. Arch. Pathol., 31:731-765, 1941. |
| 12. | Johansson JE, Ajjoub S, Coughlin LP, Wener JA, Cruess RL. Pigmented villonodular synovitis of joints. Clin. Orthop. 163:159-166,1982. |
| 13. | Larmon WA. Pigmented villonodular synovitis. Med. Clin. North America, 49: 141-150, 1965. |
| 14. | Mancini GB, Lazzeri S, Bruno G, Pucci G. Localized pigmented villonodular synovitis of the knee. Arthroscopy. 14(5):532-6, 1998 Jul-Aug. |
| 15. | Mandelbaum BR, Grant TT, Hartzman S, Reicher MA, Flannigan B, Bassett LW, Mirra J, Finerman GAM. The use of MRI to assist in diagnosis of pigmented villon-odular synovitis of the knee joint. Clin. Orthop. 231:135-9,1988. |
| 16. | McMaster PE.: Pigmented Villonodular Sunovitis with Invasion of Bone. Report of Six Cases. J. Bone and Joint Surg., 42-A:1170-1183, Oct. 1960. |
| 17. | Muscolo DL, Makino A, Costa-Paz M, Ayerza MA. Localized pigmented villonodular synovitis of the posterior compartment of the knee. Diagnosis with magnetic reso-nance imaging. Arthroscopy 1995;11:482-485. |
| 18. | Myers BW, Masi AT, Freigenbaum SL. Pigmented villonodular synovitis and tenosynovitis. A clinical epidemiological study of 166 cases and literature review. Medicine (Baltimore) 59:223-38, 1980. |
| 19. | O'Sullivan B, Cummings B, Catton C, Bell R, Davis A, Fornasier V, Goldberg R.: Outcome following radiation treatment for high-risk pigmented villonodular synovi-tis. I. J. Radiation Oncology Biol. Phys., 32:777-786, 1995. |
| 20. | Oglivie-Harris DJ, McLean J, Zarnett ME.: Pigmented villonodular synovitis of the knee. The results of total arthroscopic synovectomy, partial arthroscopic synovecto-my, and arthroscopic local excision. J. Bone and Joint Surg. 6-A:119 , 1992. |
| 21. | Poletti SC, Gates III HS, Martinez SM, Richardson WJ. The use of magnetic resonance imaging in the diagnosis of pigmented villonodular synovitis. Orthopedics 13:185-190, 1990. |
| 22. | Rao AS, Virgorita VJ Pigmented villonodular synovitis, a review of 81 cases. J Bone and Joint Surg., 66-A:76-94, 1984. |
| 23. | Ray RA, Morton CC,Lipinski KK, Corson JM, Fletcher JA. Cytogenic evidence of clonality in a case of pigmented villonodular synovitis. Cancer 67(1):121-125,1991. |
| 24. | Sakkers RJB, De Jong D, Van Der Heul RO.: X-Chromosome Inactivation in Patients who have Pigmented Villonodular Synovitis. J. Bone and Joint Surg., 73_A:1532- 1536, 1991. |
| 25. | Schwartz HS, Unni KK, Pritchard DJ.: Pigmented villonodular synovitis. Clin. Orthop. 247:243-255,1989. |
| 26. | Sledge CB, Atcher RW, Shortkroff S, Anderson RJ, Bloomer WD, Hurson BJ. Intra-articular radiation synovectomy. Clin. Orthop. 182:37-40, 1984. |
| 27. | Wiss DA. Recurrent villonodular synovitis of the knee. Successful treatment with Yttrium-90. Clin. Orthop. 169:139-143,1982. |
| 28. | Zvijac JE, Lau AC, Hechtman KS, Uribe JW, Tjin-A-Tsoi EW. Arthroscopic treatment of pigmented villonodular synovitis of the knee. Arthroscopy. 15(6):613-7, 1999 Sep. |
|
TOP OF PAGE | HOJ HOME |
| HOJ HOME | Chiefs Reports | Osgood Day | Scientific Articles | Alumni Association |