Free Vascularized Fibula Grafting: Principles, Techniques, and Applications in Pediatric Orthopaedics
Donald S. Bae, MD and Peter M. Waters, MD
Children’s Hospital
Introduction
 Bone grafts are commonly used in all specialties of orthopaedic surgery, and an understanding of the principles and
techniques of bone grafting is critical to the care of traumatic, developmental, and reconstructive musculoskeletal conditions.
While most orthopaedic surgeons are familiar with the utilization of non-vascularized bone graft and bone graft substitutes,
the applications of vascularized bone grafts --and free vascular fibula grafts in particular—are often less well understood. The
purpose of this article is to review the principles and technique of free vascularized fibula grafting, with particular attention to
its applications in pediatric orthopaedic surgery.
Bone grafts are commonly used in all specialties of orthopaedic surgery, and an understanding of the principles and
techniques of bone grafting is critical to the care of traumatic, developmental, and reconstructive musculoskeletal conditions.
While most orthopaedic surgeons are familiar with the utilization of non-vascularized bone graft and bone graft substitutes,
the applications of vascularized bone grafts --and free vascular fibula grafts in particular—are often less well understood. The
purpose of this article is to review the principles and technique of free vascularized fibula grafting, with particular attention to
its applications in pediatric orthopaedic surgery.
THE RATIONALE FOR VASCULARIZED BONE GRAFTS
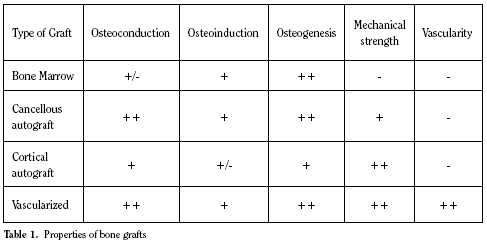
Bone grafts and bone graft substitutes have a number of
inherent properties which allow them to initiate, stimulate,
and facilitate bony healing.(1,2) (Table 1) Osteoconduction
refers to the process by which the graft provides a scaffold for
the ordered 3-D ingrowth of capillaries, perivascular tissue, and
osteoprogenitor cells. Osteoinduction refers to the recruitment
of osteoprogenitor cells from surrounding tissue. Osteogenesis
refers to the formation of new bone from either the host or graft
tissue. In addition to these three properties, it is important to
consider the mechanical strength and vascularity of the bone
graft material.
Autogenous and allogenic cortical and cancellous bone
grafts are all, to varying degrees, osteoconductive, osteoinductive,
and osteogenic. For these reasons, non-vascularized
bone grafts are effective in facilitating bony healing. When
appropriately utilized, non-vascularized bone grafts may be
incorporated into the adjacent host bone through the process
of “creeping substitution.” The bone graft material, through
the invasion of capillaries, perivascular tissue, and inflammatory
cells, is gradually revascularized and
ultimately resorbed, allowing for the formation
of new living bone which is incorporated
and remodeled into the host skeleton.
However, this process takes time, during
which the structural integrity and mechanical
strength of the bone graft and host bone
may be compromised.(1)
Vascularized bone grafts, by definition,
are placed with their vascularity intact, and
thus are immediately viable. As a result,
vascularized bone grafts obviate the need
for incorporation by creeping substitution
and may instead incorporate into the adjacent
host bone via primary (or secondary)
bone healing. This process allow allows for the mechanical
strength and structural integrity of the vascularized graft to be
preserved, which may confer greater strength and more immediate
stability to the recipient site.
FREE VASCULARIZED FIBULA GRAFTS
The fibula has been long recognized as an attractive choice
for vascularized bone grafting procedures.(3,4) Biomechanically,
the fibula bears only 15 percent of the axial load across the
ankle, allowing for its use as an autogenous bone graft with
minimal biomechanical consequences on the weight-bearing
status of the lower limb.(5) As the distal fibula also plays an
important role in conferring rotational stability and restraint
against lateral translation of the talus, efforts are made to preserve
the distal fibula during graft harvest to avoid subsequent
ankle deformity or instability.(6,7,9)
Furthermore, the vascular supply to the fibula has been
well established.(4,9) The endosteal blood supply to the fibula
is provided by a nutrient artery which typically enters the pos-
terior fibular cortex at the junction of the proximal one-third
and distal two-thirds. This nutrient artery is a branch of the
peroneal artery, which runs along the posterior aspect of the
fibular diaphysis. In addition to this nutrient vessel, the fibula
receives additional vascularity via a number of segmental musculo-
periosteal vessels which also emanate from the peroneal
artery. Based upon this understanding of the vascularity of the
fibula, techniques of vascularized fibula graft harvest have been
developed which preserve both the nutrient artery and the rich
periosteal blood supply.
 Vascularized fibular grafting also has a number of additional
theoretical advantages over conventional, non-vascularized
bone grafting techniques. Given the length of fibular diaphysis
that may be harvested, free fibular grafts are well suited for
the reconstruction of segmental defects of the long bones,
providing both mechanical strength and biological stimulus for
healing. Furthermore, based upon the fasciocutaneous arterial
branches of the peroneal artery, skin, fascia, and muscle may
be harvested concomitantly with the fibula to allow for more
complex soft tissue reconstruction. Finally, given the ability
to transfer the proximal fibular epiphysis with the diaphysis
during free vascularized fibular grafting, there is potential for
preserving continued skeletal growth of the fibular graft.(10)
Vascularized fibular grafting also has a number of additional
theoretical advantages over conventional, non-vascularized
bone grafting techniques. Given the length of fibular diaphysis
that may be harvested, free fibular grafts are well suited for
the reconstruction of segmental defects of the long bones,
providing both mechanical strength and biological stimulus for
healing. Furthermore, based upon the fasciocutaneous arterial
branches of the peroneal artery, skin, fascia, and muscle may
be harvested concomitantly with the fibula to allow for more
complex soft tissue reconstruction. Finally, given the ability
to transfer the proximal fibular epiphysis with the diaphysis
during free vascularized fibular grafting, there is potential for
preserving continued skeletal growth of the fibular graft.(10)
Despite its many theoretical advantages and applications,
however, free vascularized fibula grafting is technically challenging
and confers its own set of inherent risks and potential
complications. Sound microsurgical technique is essential in
performing the required arterial and venous anastamoses and
ensuring long-term graft viability. Furthermore, donor site
morbidity has been well documented, and up to 10% of patients
may subsequently develop ankle pain, instability, and/or progressive
valgus deformity if fibula harvest is not performed
with proper technique.(7,8) Given these considerations, free
vascularized fibula grafting should be employed in specific
clinical situations.
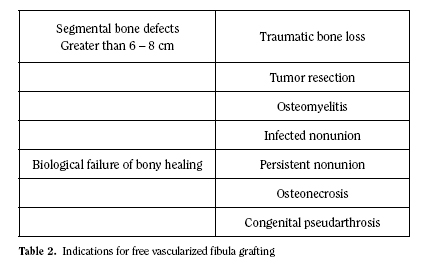
Presently, the indications for free vascularized fibula grafting
fall into two categories.(11) (Table 2) The first indication is
for segmental bony defects of greater than 6 to 8 cm, such as
seen in post-traumatic or post-infectious bone loss and tumor
resection. The second indication is for smaller bony defects in
which there has been a biological failure of bony healing, such
as seen in recalcitrant fracture nonunions, congenital pseudarthroses,
and osteonecrosis.
SURGICAL TECHNIQUE
While a detailed explanation is beyond the scope of this
review, a brief description of the technique of free vascularized
fibula graft harvest is provided to give the reader some insight
into the pertinent surgical considerations and applications.
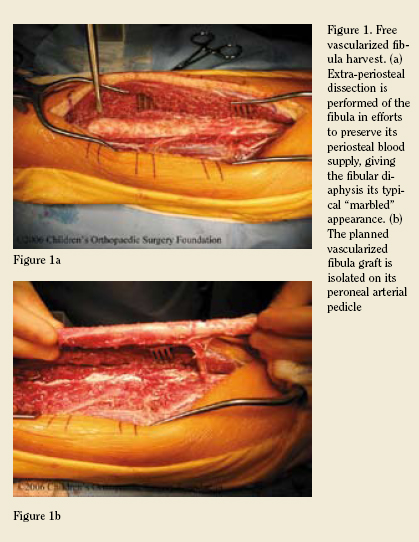
When the fibula is to be harvested without accompanying
skin or soft-tissue, a longitudinal incision is made over the
lateral aspect of the fibula. Superficial dissection is performed
in the interval between the peroneus longus muscle anteriorly
and the soleus posteriorly. The diaphysis of the fibula is then
circumferentially exposed with care being made to preserve
the periosteum and periosteal blood supply; this results in the
typical “marbled” appearance to the fibular graft. (Figure 1a)
Circumferential dissection of the fibula is continued anteriorly
and posteriorly, reflecting the peroneal and flexor hallucis
longus muscles, respectively. The peroneal artery and vein are
identified along the posterior aspect of the fibula and carefully
protected as the intermuscular septum is divided along the
length of the proposed graft. The fibula is osteotomized proximally
and distally, with preservation of the peroneal vessels.
(Figure 1b) Once the recipient site is prepared, the vascular
pedicle may be divided and the fibula transferred to the desired
location. Following stabilization of the fibula to the recipient
site ---typically performed with rigid internal screw fixation—
microvascular anastamoses are performed, reconstituting both
arterial inflow and venous outflow to the fibular graft.
 APPLICATIONS IN PEDIATRIC ORTHOPAEDICS
APPLICATIONS IN PEDIATRIC ORTHOPAEDICS
Congenital Ulnar Pseudarthros
Congenital ulnar pseudarthrosis is a
rare abnormality of skeletal growth characterized
by the development of pathological
fractures of the ulna and longstanding
pseudarthroses. Often associated
with neurofibromatosis or fibrous
dysplasia, congenital ulnar pseudarthrosis
may lead to pain, deformity, and growth
disturbance. Traditional methods of fracture care, including
open reduction and internal fixation with non-vascularized
bone grafting, are often unsuccessful. For these reasons, free
vascularized fibula grafting has been proposed as a potential
treatment option.
We have recently reviewed our institution’s experience in
treating congenital ulnar pseudarthrosis with free vascularized
fibula grafting.(12) In a retrospective analysis of 4 patients
(average age 10 years), free vascularized fibula grafting resulted
in successful bony healing in all cases. In addition to achieving
bony healing across the site of the previous pseudarthrosis,
careful restoration of ulnar length and alignment resulted in
preserved elbow and wrist motion and distal radioulnar joint
stability in all cases. Furthermore, when used in an intercalary
fashion, vascularized fibula graft allowed for the revascularization
of the dystrophic, hypoplastic distal ulnar segment.
In addition, two of the patients in this series underwent
concomitant proximal fibular epiphyseal transfer in efforts to
preserve skeletal growth potential.(10,12) (Figure 2) At most
recent follow-up, there was clinical and radiographic evidence
of continued skeletal growth of the “distal ulna” in both
instances.

Based upon this report as well as others, we conclude
that free vascularized fibula grafting is an attractive treatment
option for congenital ulnar pseudarthrosis. Concomitant proximal
fibular epiphyseal transfer should be considered in young
patients with considerable skeletal growth remaining.
Allograft Nonunion
Limb salvage surgery is an appealing option in skeletally
immature patients with malignant bone tumors. In these
situations, intercalary or osteoarticular allograft is often utilized
during bony reconstruction. Unfortunately, allograft fracture
occurs in up to 20% of cases, and traditional methods of fracture
care are often unsuccessful in these cases due to the high
mechanical stresses and altered biological milieu.(13) Free
vascularlized fibular grafting has been proposed in these situations
to promote fracture healing while preserving allograft
structural integrity.
We recently completed a retrospective
study of patients who underwent
free vascularized fibular grafting for
established allograft fracture nonunions
following limb salvage surgery for malignant
bone tumors.(14) All patients had
established allograft fracture nonunions
following the use of allograft reconstruction
for either osteosarcoma or Ewing’s
sarcoma of the extremities. Average age at the time of surgery
was 13 years, and average clinical and radiographic follow-up
was almost 4 years.

Almost 90% of patients achieved successful bony healing
following free fibular grafting, resulting in limb preservation,
pain relief, extremity stability, and satisfactory functional outcomes.
(Figure 3) Despite the relatively high complication rate,
these results support the use of free vascularized fibular grafting
in these complex clinical situations. Careful attention to rigid
internal fixation, meticulous microvascular surgical technique,
and anatomic limb alignment is essential to optimize clinical
outcomes.
Osteonecrosis of the Femoral Head
Osteonecrosis of the femoral head continues to be a cause
of pain and disability to thousands of adolescents and young
adults each year.(15) This is particularly true in the pediatric
patient population, where osteonecrosis of the femoral head
may be a result of hip trauma, septic arthritis of the hip,
slipped capital femoral epiphysis, Legg-Calve-Perthes disease,
or chronic steroid use (such as seen following solid organ
transplantation). While many treatments have been proposed,
no universal solution has been found.
Free vascularized fibular grafting has been proposed to
provide mechanical support to and revascularization of the
femoral head.(15,16,17) (Figure 4) Dean et al., in one of the
largest published series in pediatric patients, reported the early
results of free fibular grafting in 50 patients, average age 14.8
years. The majority of patients developed osteonecrosis as a
result of prior hip trauma, slipped femoral epiphysis, or steroid
use. Average Harris Hip Scores improved from 55 pre-operatively
to 90 post-operatively, and at most recent follow-up, only
16% of patients had clinical symptoms or radiographic progression
severe enough to warrant conversion to hip arthrodesis or
arthroplasty. Based upon these results, the authors conclude
that free fibular grafting in pediatric patients with femoral head
osteonecrosis may relieve pain, improve function, and delay the
need for future hip arthroplasty.
CONCLUSIONS
Free vascularized fibula grafting provides an attractive
reconstructive option for the orthopaedic surgeon. Given its
ability to provide immediate structural support and vascularity
– as well as its inherent osteoconductive, osteoinductive, and
osteogenic properties—free fibular grafting should be considered
in the management of large segmental bony defects as
well as situations in which there has been a biological failure
of bony healing. The use of rigid internal fixation, careful softtissue
and bony reconstruction, and meticulous microvascular
surgical technique are essential in achieving the best possible
outcomes.
References:
- 1. JA Buckwalter, TA Einhorn, SR Simon, eds. Orthopaedic Basic Science. Chicago: American Academy of Orthopaedic Surgeons, 2000.
- 2. Khan SN, Cammisa FP, Sandhu HS, Diwan AD, Firardi FP, Lane JM. The biology of bone grafting. J Am Acad Orthop Surg 2005; 13: 77-86.
- 3. Huntington TW. Case of bone transference. Use of a segment of fibula to supply a defect in the tibia. Ann Surg 1905; 41:249.
- 4. Taylor GI, Miller GDH, Ham FJ. The free vascularized bone graft. A clinical extension of microsurgical technique. Plast Reconstr Surg 1975; 55: 533.
- 5. Lambert KL. The weight-bearing function of the fibula. A strain gauge study. J Bone Joint Surg Am 1971; 53: 507-513.
- 6. Pacelli LL, Gillard J, McLoughlin SW, Buehler MJ. A biomechanical analysis of donor-site ankle instability following free fibular graft harvest. J Bone Joint Surg Am 2006;85: 597-603.
- 7. Vail TP, Urbaniak JR. Donor-site morbidity with the use of vascularized autogenous fibular grafts. J Bone Joint Surg Am 1996; 78: 204-211.
- 8. Kanaya K, Wada T, Kura H, Yamashita T, Usui M, Ishii S. Valgus deformity of the ankle following harvesting of a vascularized fibular graft in children. J Reconstr Microsurg 2002;18: 91-96.
- 9. Malizos KN, Zalavras CG, Soucacos PN, Beris AE, Urbaniak JR. Free vascularized fibular grafts for reconstruction of skeletal defects. J Am Acad Orthop Surg 2004; 12:360-369.
- 10. Tsai TM, Ludwig L, Tonkin M. Vascularized fibular epiphyseal transfer. A clinical study. Clin Orthop Relat Res 1986; 210: 228-234.
- 11. DP Green, RN Hotchkiss, WC Pederson, S Wolfe, eds. Green’s Operative Hand Surgery, 5th ed. Philadelphia: Churchill Livingston, 2005.
- 12. Bae DS, Waters PM, Sampson CE. Use of free vascularized fibular graft for congenital ulnar pseudarthrosis: surgical decision-making in the growing child. J Pediatr Orthop Am 2005; 25: 755-762.
- 13. Sorger JI, Hornicek FJ, Zavatta M, Menzner JP, Gebhardt MC, Tomford WW, Mankin HJ. Allograft fractures revisited. Clin Orthop Relat Res 2001; 382: 66-74.
- 14. Bae DS, Waters PM, Gebhardt MC. Free vascularized fibular grafting for allograft fracture nonunions following limb salvage surgery for malignant bone tumors. Presented at the 60th Annual Meeting of the American Society for Surgery of the Hand, San Antonio, Texas, September 22-24, 2005.
- 15. Urbaniak JR, Harvey EJ. Revascularization of the femoral head in osteonecrosis. J Am Acad Orthop Surg 1998; 6: 44-54.
- 16. Urbaniak JR, Boogan PG, Gunneson EB, Nunley JA. Treatment of osteonecrosis of the femoral head with free vascularized fibular grafting. J Bone Joint Surg Am 1995; 77: 681-694.
- 17. Dean GS, Kime RC, Fitch RD, Gunneson E, Urbaniak JR. Treatment of osteonecrosis in the hip of pediatric patients by free vascularized fibular graft. Clin Orthop Relat Res.2001; 386: 106-113
|