Osteoanabolic Agents: State of the Art and Potential for Orthopaedic Surgery
Julie Glowacki, PhD
Brigham and Women’s Hospital
INTRODUCTION
Progress in development of safe and effective osteoanabolic
agents has been made in the area of osteoporotic bone loss but
may have other applications for orthopedic surgery. Skeletal
aging is explained as the inexorable loss of bone mass that
results from an imbalance between bone formation and resorption
that may increase the risk of fracture. Approaches to prevention
start in childhood with optimizing the accretion of peak
bone mass by appropriate exercise and nutrition. In adults, in
addition to proper exercise, nutrition, and avoidance of skeletal
toxins like smoking, pharmacological tactics have been devised
to diminish the rate of bone resorption with agents such as
estrogen, calcitonin, raloxifene, and bisphosphonates. Past
trials with osteoanabolic agents like fluoride, growth hormone,
and insulin-like growth factor (IGF) have been disappointing
because of unacceptable side effects and narrow range of effective
doses. There are ongoing strategies to improve the advantage-
to-disadvantage profiles of such agents, and to evaluate
their potential for other indications, such as accelerating fracture
healing or incorporation of prostheses.
THE PARATHYROID HORMONE (PTH) PARADOX
Recent FDA approval of teriparatide (a fragment of parathyroid
hormone identified as PTH(1-34) for management of
osteoporosis has renewed interest in anabolic actions of different
forms of PTH. PTH has been recognized as a hormone
that stimulates osteoclast differentiation and bone-resorbing
activity. This apparent contradiction is resolved by information
about the mechanisms of PTH’s anabolic actions.
The intact form of PTH is a peptide with 84 amino acid
residues, designated as PTH(1-84). Primary hyperparathyroidism
presents with hypercalcemia due to excess secretion of PTH
by benign adenoma(s) in the parathyroid gland and historically
was associated with radiographic evidence of subperiosteal
bone resorption of the distal phalanges, loss of the lamina
dura of the teeth, tapering of distal clavicles, “salt-and-pepper”
appearance of the skull, bone cysts, and giant cell tumors in the
long bones or gingiva. It is treated by surgical removal of the
adenoma(s). In the United States, overt hyperparathyroid bone
disease is now seen in less than 5% of patients with primary
hyperparathyroidism, but primary hyperparathyroidism itself
is a common endocrine disease with incidence of 1 in 500 to 1
in 1000. Only diabetes mellitus and hyperthyroidism are more
common endocrine diseases.
In 1932, Selye showed that administration to rats of
continuous high doses of PTH resulted in bone loss, whereas
intermittent low doses of PTH or some of its fragments resulted
in increased bone mass (1). Clinical and experimental research
with the latter led to the development of new anabolic therapies
capable of increasing the production of bone matrix by osteoblasts
and reversing microarchitectural deterioration, resulting
in major improvements in both bone quality and bone quantity.
Teriparatide, a recombinant human parathyroid hormone
consisting of the first 34 of 84 amino acids in human parathyroid
hormone, was shown to reduce significantly the risk of
both vertebral and non-vertebral fractures in postmenopausal
women (2) and in men (3). There are still many unanswered
questions regarding PTH treatment of osteoporosis, including
the optimal duration of treatment, optimal dosing regimen,
mechanism of resistance to its effect after 18-24 months, and
the effect of subsequent rechallenge.
CENTRAL ROLE OF THE SKELETAL IGF SYSTEM
Adult bone homeostasis is characterized by a balance
between bone formation by osteoblasts and bone resorption by
osteoclasts, a process called bone remodeling. Remodeling is
regulated by many factors including circulating, i.e. systemic,
factors as well as local factors produced and acting within the
bone microenvironment. Skeletal insulin-like growth factors
(IGFs, a.k.a. somatomedins) are important local factors that
stimulate bone formation and that serve as intermediary factors
by which systemic agents promote bone formation.
IGFs are part of an axis whereby hypothalamic Growth
Hormone Releasing Factor (GHRH) stimulates release of pituitary
Growth Hormone (GH, a. k. a. somatotropin). Circulating
GH exerts many effects on remote organs, the liver being one
of its major target organs. GH induces both hepatic and skeletal
production of IGF. IGFs bind to specific receptors on the
surface of osteoblasts and result in DNA or matrix synthesis
depending on receptor density and differentiation stage of the
osteoblast. Activity of IGFs can be modulated by high-affinity
IGF-Binding Proteins (IGF-BPs), which are produced by bone
cells and co-regulated with IGFs. The BPs can be activating or
inactivating, in same cases depening upon the phosphorylation
state of the protein. In turn, IGF-BP effects can be modified
by specific proteases that catalyze their proteolysis. Thus, IGF
bioavailability is a complex result of many interactions and can
explain temporal and spacial specificity of bone responses to
manipulations or treatments.
ROLE OF NUTRITION AND IGF IN SKELETAL HEALTH
Many factors influence the extent of bone formation in an
individual, especially nutritional ones. Adequate intake of protein
is essential for skeletal growth and maintenance, but excess
intake of animal proteins, such as found in Western diets, is
associated with osteoporosis. Acid-forming proteins from
animal foods cause hypercalciuria and drain the bone of stored
mineral. This is an explanation for some vegetarian diets being
more protective of bone health. Calcium is required for bone
growth and maintenace, but adequate levels are not achieved
with typical American diets. Current best estimates for the
average calcium requirement are in the range of 1000 mg/day
for mature adults and rising to 1200-1400 mg/day by age 75
years. Intestinal absorption of calcium averages approximately
30% and decreases with age. Calcium absorption is inhibited by
phosphates, found in abundance in cola softdrinks and in many
processed foods. Americans often exceed the phosphate recommendation
of 700 mg/day for adults. High intake of sodium
leads to increased urinary calcium excretion. Thus, for skeletal
health, it is necessary to achieve the proper intake of protein
and the proper proportions of calcium and phosphate, and of
sodium and potassium in the diet. This is especially difficult
for elders to achieve. In addition, dietary micronutrients like
vitamin D, vitamin C, vitamin K, magesium, boron, and other
trace minerals have essential roles in bone tissues.
The rate of complications after fracture can be increased
by nutritional insufficiencies. The IGF system appears to be
directly involved in the mechanisms leading to osteoporotic
fracture and to its complications. Studies show low serum
concentrations of IGF-I in patients with osteoporotic fractures.
Baseline IGF-I levels are associated with length of stay in rehabilitation
hospitals. The effects of protein repletion have been
investigated in elderly undernourished patients with a recent
hip fracture. In several studies, clinical outcomes, including
shorter rehabilitation hospital stay, were significantly improved
by nasogastric, parenteral, or oral supplementations that rectified
protein intake. In the presence of adequate calcium and
vitamin D, protein supplements increase serum IGF levels.
Evidence shows the importance of nutritional support to prevent
and to heal osteoporotic fractures.
THE SOMATOPAUSE
Growth Hormone and IGFs are needed to support skeletal
growth of children. Deficiency in children results in short
stature. Increased secretion of GH by pituitary tumors leads
to gigantism before puberty and to acromegaly after puberty.
With aging, there is a decline in serum levels of both GH and
IGFs, a process termed the somatopause. Because GH deficiency
is associated with low bone mass that is enhanced with
GH therapy, interest rose for replenishing GH and/or IGF to
prevent age-associated bone loss and musculoskeletal fragility.
An early study reported that administration of GH to healthy
elderly men resulted in reduced adiposity and increases in lean
body mass and strength (4). Unfortunately, the small 1.6%
increase in lumbar bone mineral density was not sustained. For
unknown reasons, some subjects appeared to be GH-resistant.
Even more troubling is the high incidence of side effects in
many trials with recombinant GH, including glucose intolerance
(i.e. diabetes mellitus), edema, carpal tunnel syndrome,
gynecomastia, orthostatic hypotension, and weight gain. Use
of GH-releasing analogs is not associated with significant sideeffects,
but further studies are needed to show efficacy on bone
mass.
There are potential benefits to using recombinant IGF-I
rather than GH in the treatment of osteoporosis: direct action
on bone formation, avoidance of GH resistance, and reduction
in side effects. Nevertheless, a recent study on the relationship
between serum IGF-I concentration and the incidence of side
effects of therapy with recombinant human growth hormone
(rhGH) and recombinant human insulin-like growth factor-I
(rhIGF-I) revealed that for both agents, the magnitude of the
initial increase in the serum IGF-I concentration was a powerful
risk factor for severe orthostatic hypotension, diffuse myalgias,
and drug-induced hepatitis (5).
In vivo, IGF-I is transported in blood with a protein, IGF
binding protein-3 (IGFBP-3). Because of animal studies showing
that administration of the complex of IGF-I/IGFBP-3 had
improved safety and efficacy compared with IGF-I alone, the
complex was given to severely osteoporotic elderly women for
8 weeks following surgical management of hip fracture (6). All
subjects lost hip bone density after hip fracture, but at 3 and 6
months the treated group regained lost bone while the placebo
group continued to lose even more. In addition, post-surgical
muscle strength and function ability were improved only in
the treated group. There were no differences in side effects or
clinical abnormalities. Other trials with stable complexes of
IGF-I and IGFBP-3 are ongoing to assess long-term safety and
efficacy in different populations.
ANABOLIC EFFECTS OF PARATHYROID HORMONE (PTH) VIA SKELETAL IGFS
Another strategy to enhance IGF-I action specifically in
bone is exemplified by administration of an agent such as PTH.
Animal studies with intermittent PTH demonstrated significant
increases in cancellous bone mass and with no changes or
slight decreases in cortical bone. PTH was unable to increase
bone formation in IGF-I-deficient mice (7). It is also clear from
in vitro studies that PTH induces IGF-I expression and secretion
in osteoblasts (8). Given the issues of safety with administration
of GH or IGF-I, it is possible that PTH acts at least in part by
increasing local production of IGF-I or serum complexes of IGF
and its modulating binding proteins, rather than by increasing
serum levels of free IGF.
EFFECTS OF PARATHYROID HORMONE (PTH) ON HUMAN BONE MARROW CELLS (9)
 We treated marrow-derived adherent stromal cells (MSCs,
a.k.a mesenchymal stem cells) obtained from subjects undergoing
hip replacement with osteogenic supplements (10 nM
dexamethasone, 5 mM glycerophosphate, and 170 �M ascorbic
phosphate) � 10 nM PTH(1-34). Osteoblast differentiation
was assessed by measurement of alkaline phosphatase, an early
marker of the osteoblast phenotype. In cultures from a 42-yearold
woman, for example, PTH significantly stimulated alkaline
phophatase (780 � 49 nmole/min/g compared with control,
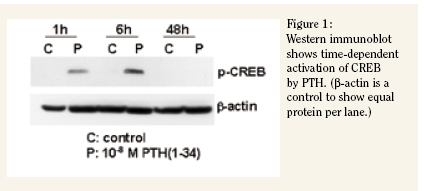
601 � 80, p=0.03). One of the signaling pathways that PTH
stimulates in its target cells results in the phosphorylation of
CREB (cAMP-responsive element binding protein). We assessed
that mechanism with Western immunoblot of phosphorylated
CREB in protein extracts of the same MSCs at intervals following
treatment with 10nM PTH(1-34). These assays provides
evidence for increased osteoblastogenesis and signaling by
PTH in human MSCs and indicates the suitability of this cell
culture system to assess osteoanabolic effects of PTH and other
agents.
We treated marrow-derived adherent stromal cells (MSCs,
a.k.a mesenchymal stem cells) obtained from subjects undergoing
hip replacement with osteogenic supplements (10 nM
dexamethasone, 5 mM glycerophosphate, and 170 �M ascorbic
phosphate) � 10 nM PTH(1-34). Osteoblast differentiation
was assessed by measurement of alkaline phosphatase, an early
marker of the osteoblast phenotype. In cultures from a 42-yearold
woman, for example, PTH significantly stimulated alkaline
phophatase (780 � 49 nmole/min/g compared with control,
601 � 80, p=0.03). One of the signaling pathways that PTH
stimulates in its target cells results in the phosphorylation of
CREB (cAMP-responsive element binding protein). We assessed
that mechanism with Western immunoblot of phosphorylated
CREB in protein extracts of the same MSCs at intervals following
treatment with 10nM PTH(1-34). These assays provides
evidence for increased osteoblastogenesis and signaling by
PTH in human MSCs and indicates the suitability of this cell
culture system to assess osteoanabolic effects of PTH and other
agents.
OSTEOANABOLIC THERAPIES AND ORTHOPEDIC SURGERY
Currently, anabolic PTH therapy is available only by daily
injection of the peptide and is approved for treatment of osteoporosis.
Research is targeted to the development of effective
oral, buccal, sublingual, transdermal, nasal and pulmonary
inhalation formulations.
Once easier delivery forms are available, there may be
new enthusiasm for applying osteoanabolic therapies for other
orthopedic indications such as impaired fracture healing or
joint reconstruction. A number of rat studies, such as (10)
and (11), suggest that PTH may enhance fracture healing,
but more needs to be known for situations in which repair is
compromised and whether the magnitude of stimulation is of
clinical significance.
Studies indicate a dramatic drop in serum IGF-I in elders
after a hip fracture (12). Whether this drop is a result of chronic
malnourishment prior to surgery, of the injury itself, of the
surgery, and/or of hospitalization, the theoretical possibilty that
short-term PTH treatment could have benefical effects on healing
needs further exploration.
DISADVANTAGES OF OSTEOANABOLIC THERAPY
As with other powerful anabolic therapies, there are concerns
about overstimulation with chronic therapy for osteoporosis.
Long-term carcinogenicity studies in rats revealed
that up to 53% of rats that received hPTH (1-34) for 2 years
developed osteosarcoma. That is the basis for the FDA requiring
a black box warning in the package insert and limiting use
for osteoporosis in humans to 2 years. It is generally believed
that osteosarcoma is a low risk in humans because of little
literature on osteosarcoma in primary hyperparathyroidism
(although new reports have appeared since the approval of
teriparatide), no osteosarcomas in the thousands of patients
treated with teriparatide, the known susceptibility of Fischer
344 rats to osteosarcoma, and the very high doses given to
the rats. Hypercalcemia and hypercalciuria are associated with
PTH(1-34) (requiring patients to minimize calcium intake), but
may be avoided with other PTH analogs. For all these reasons,
teriparatide is recommended mainly for patients with severe
osteoporosis who are refractory to other forms of anti-osteoporotic
therapy. Cost is also an issue; teriparatide (Forteo�) costs
$600 per month.
Some immunological responses have been reported. Some
tested patients developed antibodies to the peptide and some
developed generalized urticarial reactions or local irritation at
the injection site. It appears that skeletal responsiveness to
teriparatide diminishes after 1.5 years of treatment, but the
basis is not known.
Second generation forms of anabolic PTH are being developed
to avoid these issues. In blood there are many fragments
of PTH besides the 84-amino acid form. It had been believed
that they were inactive degradation products, but recent studies
indicate distinct and specific activities of many of them. These
are being evaluated and derivatized for enhanced potential for
osteoanabolic effects without side-effects.
SUMMARY
Research with osteoanabolic agents has eliminated many
candidate compounds because of unacceptable side effects and
narrow range of effective doses. Increased understanding of the
important regulatory role of skeletal IGF raises interest in treatments
that work through that mechanism but in a highly controlled
manner. Information gained from clinical use of PTH
for osteoporosis may have applications for short-term therapy
for other orthopedic applications such as fracture healing and
joint reconstruction.
Questions remain about patient selection, avoidance of
antibody production, and strategies for administration by other
than subcutaneous injection. More information is needed
about the apparent selectivity of PTH for trabecular bone.
Although there are concerns about long-term use of teriparatide,
it is likely that short-tem use of other PTH derivatives in
orthopedic settings will have lower risk for complications.
Julie Glowacki, Ph.D. is a Professor of Orthopedic Surgery, Professory of Oral & Maxillofacial Surgery, Brigham and Women’s Hospital
Address correspondence to:
Julie Glowacki Ph.D.
Brigham and Women’s Hospital
75 Francis Street, MRB 1
Boston, MA 02115
References:
- Selye H. On the stimulation of new bone formation with parathyroid extract and irradiated ergosterol. Endocrinology 16:547-558, 1932.
- Neer RM et al. Effect of parathyroid hormone (1-34) on fractures and bone mineral density in postmenopausal women with osteoporosis. New Engl J Med 344:1434-41, 2001
- Orwoll ES et al. The effect of teriparatide [human parathyroid hormone (1-34)] therapy on bone density in men with osteoporosis. J Bone Miner Res. 2003 Jan;18(1):9-17.
- Rudman D et al. Effects of human growth hormone in men over 60 years old. N Engl J Med. 1990;323:1-6.
- Sullivan DH, Carter WJ, Warr WR, Williams LH. Side effects resulting from the use of growth hormone and insulin-like growth factor-I as combined therapy to frail elderly patients. J Gerontol A Biol Sci Med Sci. 1998;53:M183-7.
- Boonen S et al. Musculoskeletal effects of the recombinant human IGF-I/IGF binding protein-3 complex in osteoporotic patients with proximal femoral fracture: a doubleblind, placebo-controlled pilot study. J Clin Endocrinol Metab. 2002;87:1593-9.
- Yakar S et al. The ternary IGF complex influences postnatal bone acquisition and the skeletal response to intermittent parathyroid hormone. J Endocrinol. 2006;189:289-99.
- McCarthy TL, Centrella M, Canalis E. Parathyroid hormone enhances the transcript and polypeptide levels of insulin-like growth factor I in osteoblast-enriched cultures from fetal rat bone. Endocrinology. 1989;124:1247-53.
- Glowacki J, Zhou S, Amato I, Adler C, Epperly MW, Greenberger JS. Age-related intrinsic changes in human marrow stromal cells and their differentiation to osteo blasts. Orthopedic Res Soc, March, 2006, Chicago IL.
- Andreassen TT, Ejersted C, Oxlund H. Intermittent parathyroid hormone (1-34) treatment increases callus formation and mechanical strength of healing rat fractures. J Bone Miner Res. 1999;14:960-8.
- Alkhiary YM et al. Enhancement of experimental fracture-healing by systemic administration of recombinant human parathyroid hormone (PTH 1-34). J Bone Joint Surg Am. 2005;87:731-41.
- Cook F et al. Major changes in the circulatory IGF regulatory system after hip fracture surgery. J Bone Min Res 1996; 11: S327;
|