Preliminary Results of a Retrospective Review of Hip Fracture Operations at Night versus Daytime
Miguel A. Ramirez MD, Lars C. Richardson MD, Joseph Hong, Edward K. Rodriguez MD, Arun J. Ramappa, MD
The Beth Israel Deaconess Medical Center
Introduction
Since the death of Libby Zion at New York Hospital in
1984, fatigue and sleep deprivation in medicine has become
an issue of concern, ultimately leading to recent changes in
Resident work hours.6 The amount of continuous duty and
work hours demanded of the profession exceed those that are
legally allowed in nuclear power and transportation industries.7
As a result, it has been of interest to researchers to try to explain
whether or not long hours and lack of sleep have a negative
effect in patient care.
Surgeries performed outside of the regular work day have
been correlated with increased in-hospital mortality. In a 2001
study, Bell et al2 found that patients admitted during weekends
for ruptured abdominal aortic aneurysms, acute epiglottitis,
and pulmonary embolism had a significantly greater mortality
than those admitted on weekdays. In hip fracture surgeries,
Foss et al5 found that 5-day and 30-day mortality post hip fracture
repair were significantly higher when performed during
holidays and weekends.
Currently, there are no studies that have looked at the
differences in outcomes of hip fracture surgeries performed in
the daytime hours versus those after hours. The purpose of
this study is to assess whether there is a risk associated with
performing hip fracture surgeries after-hours as compared to
those performed during the daytime hours. We believe that
due to short staffing overnight and surgeon fatigue, there will
be a significantly number of complications when surgeries are
performed at night versus the daytime.
MATERIALS AND METHODS
Using Beth Israel Deaconess Medical Center hospital
records, we retrospectively identified all patients admitted with
ICD9 codes pertaining to hip fractures from January 2000 to
June December 2005. We have reviewed over 750 records so
far.
Procedures were stratified into 3 groups based on time of
incision. Group 1 included those whose incision was between
07:00 and 17:59. Group 2 had procedures started between
18:00 and 23:59. Operations in Group 3 took place between
00:00 and 06:59.
Operative reports were reviewed for procedure type and
length, anesthesia time, blood loss, IV fluids, transfusions,
number of staff present, ASA status, and intra-operative complications,
and mortality.
In-house records were reviewed for complications including
infection, pneumonia, implant failure, reoperation, and
mortality. Transfusions, length of hospital stay, and discharge
location was also recorded.
Follow-up complications were recorded such as infection,
GI bleeding, deep venous thrombosis (DVT), pulmonary
embolus, Non-union, refracture, and reoperation.
Mortality assessments were made 1. During their hospital
stay. 2. One-month post-operatively, and 3. One-year postoperatively.
Mortality data was obtained from the Social Security
Death Index (SSDI) online at http://ssdi.rootsweb.com and
from patient records where available.
RESULTS
750 records have been reviewed so far. Data analysis was
carried out on 300 records.
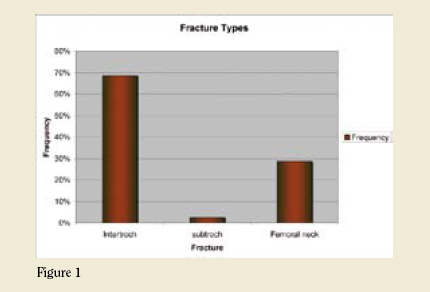
There was no demographic difference found between the
groups in terms of age, gender, ASA status, and fracture types.
Median age at the time of surgery was 77 years with a range
of 19-100 years. Approximately 2/3 of fractures were intertrochanteric,
(Figure 1).
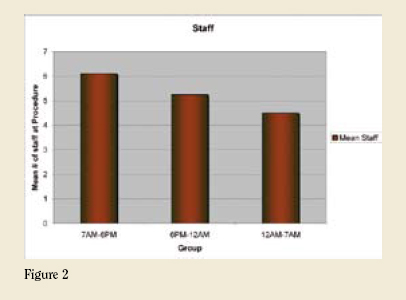
There was fewer staff in surgeries performed overnight
versus the daytime (Figure 2). There was also greater likelihood
of an assistant being present during the day. There was a small,
non-significant difference in anesthesia time, with after-hours
surgeries having longer time under anesthesia. There was no
difference seen in intra-operative factors in terms of blood
loss, IV fluids, and complications among the different groups
(table1).
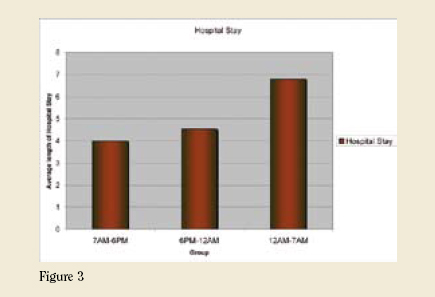
While in-house, there was no difference seen in the number
of complications or transfusions. There was a non-significant
difference in hospital stay among the different groups
(Figure 3).
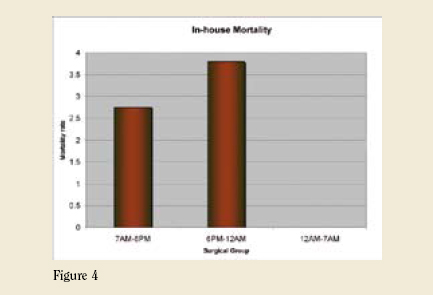
In-house mortality was significantly higher when surgeries
were performed 6PM and 12 AM than those during the day
hours (Figure 4). There was no difference seen in one-month
or one-year mortalities among the groups.
DISCUSSION
Several studies have shown that fatigue and sleep deprivation
negatively impairs performance, alertness, and mood.1,3,4,10,11
House officer function after a long call night has been shown
to be equivalent to having a blood alcohol concentration of
0.04 to 0.05 g%.1 Reaction times of residents with heavy call
were 7% slower than those with a light call. Taffinder et al
found that surgeons who had no sleep committed 20% more
errors and took 14% longer to complete a laparoscopy simulator
exercise than when they had a full night of sleep.14 Another
study looking at medical errors performed by residents found
that approximately one third of errors occurred as a result of
working long hours.8
There is unclear evidence to support how these fatigue
impairments in surgical dexterity and attention translate to
poor clinical performance. Resident on-call status had no
effect on their performance on the American Board of Surgery
In-Training Examination (ABSITE).13 A study comparing
the difference in medical errors between a night float system
vs. traditional on-call system found that although residents
in traditional call system performed significantly lower on
memory scanning and addition tasks than those in the nightfloat
system (p<0.05), errors were not different among the two groups.9 These results suggest that although cognitive and physical performance may be impaired with lack of sleep, this does not seem to translate negatively into patient care. A potential reason for this may be that residents that are sleepdeprived are able to compensate for sleep loss in crises or stressful situation, however, they may be more prone to errors on routine tasks, or tasks that require constant attention, such as surgery12. 
Based on preliminary results from our study, there seems
to be little difference in surgeries performed at night versus the
daytime. Despite the fact that surgeries performed after-hours
had fewer staff and were less likely to have an assistant, there
was no significant difference in surgery complications between
the groups. There was no difference in complications in-house
or at follow-up.
There was a higher in-hospital mortality associated with
surgeries performed between 6PM and 12 AM. Most deaths
were caused by cardiopulmonary arrest, with no intraoperative
deaths. There were, however, no perceived differences in
one-month or one-year mortality rates. Patients operated afterhours
had longer hospital stays than those operated between
7AM and 6 PM.
This project is currently at 70% of data collection and 30%
of data analysis. We hope to have a finished project in early
July 2006.
CONCLUSIONS
Preliminary results show that there is an increased risk
of intra-hospital mortality associated with after-hour surgeries.
So far, there is no statistical difference in one-month or
one-year mortality rates. Surgeries performed at night are significantly
fewer-staffed and have less of a likelihood to have an
assistant than those performed during the day. There is also no
difference seen in intraoperative or in-house complications.
Miguel A. Ramirez M.D. is the Doris Duke Fellow at Beth Israel Deaconess Medical Center.
Lars C. Richardson M.D. is a Clinical Instructor of Orthopedic Surgery at Harvard Medical School.
Edward K. Rodriguez M.D. is a Clinical Instructor of Orthopedic Surgery at Harvard Medical School.
Arun J. Ramappa M.D. is a Clinical Instructor of Orthopedic Surgery at Harvard Medical School.
Address correspondence to:
Arun Ramappa M.D.
Beth Israel Deaconess Medical Center
330 Brookline Ave
Boston, MA 02115
References:
- Arnedt, J. T.; Owens, J.; Crouch, M.; Stahl, J.; and Carskadon, M. A.: Neurobehavioral performance of residents after heavy night call vs after alcohol ingestion. Jama, 294(9): 1025-33, 2005.
- Bell, C. M., and Redelmeier, D. A.: Mortality among patients admitted to hospitals on weekends as compared with weekdays. N Engl J Med, 345(9): 663-8, 2001.
- Caldwell, J. A.; Caldwell, J. L.; Smith, J. K.; and Brown, D. L.: Modafinil’s effects on simulator performance and mood in pilots during 37 h without sleep. Aviat Space Environ Med, 75(9): 777-84, 2004.
- Dinges, D. F.; Pack, F.; Williams, K.; Gillen, K. A.; Powell, J. W.; Ott, G. E.; Aptowicz, C.; and Pack, A. I.: Cumulative sleepiness, mood disturbance, and psychomotor vigilance performance decrements during a week of sleep restricted to 4-5 hours per night. Sleep, 20(4): 267-77, 1997.
- Foss, N. B., and Kehlet, H.: Short-term mortality in hip fracture patients admitted during weekends and holidays. Br J Anaesth, 2006.
- Friedman, W. A.: Resident duty hours in American neurosurgery. Neurosurgery, 54(4): 925-31; discussion 931-3, 2004.
- Gaba DM, H. S.: Fatigue Among Clinicians and the safety of patients. New England Journal of Medicine, 347(16): 1249-1255, 2002.
- Gawande, A. A.; Zinner, M. J.; Studdert, D. M.; and Brennan, T. A.: Analysis of errors reported by surgeons at three teaching hospitals. Surgery, 133(6): 614-21, 2003.
- Lee, D. T.; Chan, S. W.; and Kwok, S. P.: Introduction of night shift call system for surgical trainees: a prospective self-controlled trial. Med Educ, 37(6): 495-9, 2003.
- Leung, L., and Becker, C. E.: Sleep deprivation and house staff performance. Update 1984-1991. J Occup Med, 34(12): 1153-60, 1992.
- Philibert, I.: Sleep loss and performance in residents and nonphysicians: a meta-analytic examination. Sleep, 28(11): 1392-402, 2005.
- Samkoff, J. S., and Jacques, C. H.: A review of studies concerning effects of sleep deprivation and fatigue on residents’ performance. Acad Med, 66(11): 687-93, 1991.
- Stone, M. D.; Doyle, J.; Bosch, R. J.; Bothe, A., Jr.; and Steele, G., Jr.: Effect of resident call status on ABSITE performance. American Board of Surgery In-Training Examination. Surgery, 128(3): 465-71, 2000.
- Taffinder, N. J.; McManus, I. C.; Gul, Y.; Russell, R. C.; and Darzi, A.: Effect of sleep deprivation on surgeons’ dexterity on laparoscopy simulator. Lancet, 352(9135): 1191, 1998.
|