Musculoskeletal Medicine: An Assessment of the Attitudes and Knowledge of Medical Students
Charles S. Day, MD, Albert C. Yeh, and Edward Krupat, PhD
Beth Israel Deaconess Medical Center
Abstract
Context: In September of 2005, the Association of
American Medical Colleges published a report on musculoskeletal
medicine education expressing growing concern that
physicians lack the skills necessary to recognize and treat the
expected increase in musculoskeletal disorders. Recent studies
have suggested that American and Canadian medical schools
may not be effectively addressing musculoskeletal medicine in
their curriculums.
Objectives: To assess the medical students’ attitude
towards musculoskeletal medicine and the musculoskeletal
curriculum and to measure their knowledge in this subject by
using a validated instrument.
Design, Setting, and Participants: A cross-sectional volunteer
survey study of first, third, and fourth year Harvard
Medical School students was conducted during the 2005-2006
academic school year. Overall response rates were 101/165
(61%), 120/183 (65%), and 80/153 (52%) of first, third, and
fourth year medical students respectively. Participants were
recruited through various courses and also through USMLE
Step II review sessions.
Main Outcome Measures: Perception towards impact of
musculoskeletal education on future career, self-reported confidence
in performing a physical examination, attitudes towards
the current musculoskeletal curriculum, and basic knowledge
in musculoskeletal medicine.
Results: The graduating class ranked musculoskeletal
medicine as being of “major importance” (3.95/5, [95% confidence
interval {CI}: 3.78-4.12]) towards their career but
rated the required curriculum time spent on musculoskeletal
medicine as “poor” (1.92/5, [95% confidence interval {CI}:
1.76-2.08]). Students who took clinical electives in the subject
improved their confidence in examining the musculoskeletal
system (electives: 2.04/5, no electives: 2.38/5, p<.001) and enhanced their performance on the competency exam (electives: 71.4%, no electives: 57.6%, p<.001). Only 25% (20/80) of the graduating class demonstrated competency in musculoskeletal medicine using a passing benchmark set by U.S. internal medicine residency program directors.
Conclusions: Medical students’ attitude and knowledge
of musculoskeletal medicine indicate that the undergraduate
medical institution may not be providing adequate training in
this field to address the current and projected trends in musculoskeletal
health care.
INTRODUCTION
The prevalence of musculoskeletal (MSK) symptoms seen
in a wide spectrum of medical practice has drawn much
attention to undergraduate MSK medicine education across
American and Canadian medical schools within the past five
years(1-8). MSK complaints and injuries comprise approximately
15-30% of primary care visits(5,9), 20% of emergency
room visits(10), and 20% of non-routine pediatric visits(11).
MSK symptoms have consistently accounted for the number
one or two reason for patient visits to physicians’ office(9,12,13)
and in 1995, resulted in 98.6 million office visits(13). In 2005, a
Medical School Objectives Project (MSOP) report issued by the
Association of American Medical Colleges (AAMC) suggested
that because people in the United States are living longer,
healthier lives, the prevalence of MSK conditions is increasing
and will continue to rise over time(1). This trend poses a significant
health problem to society due to the high impact that
MSK disorders have on disability(14), the resulting productivity
time lost in the workforce(15,16), and the subsequent cost to
health care estimated at $200 billion annually(16,17).
Despite compelling sources of evidence pointing at the
prevalence of MSK complaints in clinical practice, it is unclear
whether American and Canadian medical schools are effectively
educating medical students in this field(3-5,8). In 2001,
a comprehensive study reviewing the curricula of all Canadian
medical schools indicated that directors of undergraduate MSK
programs felt dissatisfied with the current time devoted to MSK
education(5). Also in the same year, survey responses by over
1,900 second-year residents in United States residency programs
revealed that residents felt poorly or very poorly prepared
in their training on examining various MSK body parts(6). In
2003, Freedman and Bernstein showed that 78% of all entering
residents at the University of Pennsylvania School of Medicine
failed to demonstrate basic competency in MSK medicine using
a nationally validated basic competency exam in MSK medicine.
The suggested passing criterion of the exam was determined by
58% of all internal medicine residency program directors across
the United States based on what they felt all medical school
graduates should know(2). The authors suggested that medical
school education in MSK medicine is likely to be inadequate.
Few studies have directly evaluated the effectiveness of
the medical students’ training in MSK medicine at the undergraduate
medical institution. Our study addresses this issue by
assessing the adequacy of the undergraduate MSK education
curriculum at Harvard Medical School. The objectives of the
study were: 1) to assess medical students’ attitude towards
MSK medicine and the MSK curriculum, and 2) to examine
the students’ knowledge in MSK medicine by using a validated
competency exam.
MATERIALS AND METHODS
Sample Selection and Administ ration
Institutional Review Board approval was obtained from
Harvard Medical School to anonymously survey all undergraduate
medical students in the first, third, and fourth year
classes during the 2005-2006 academic school year. First year
students participated in the study during the first month of
school and provided a baseline comparison in MSK knowledge
and attitudes. The survey was administered online through
the mandatory Human Body course. Third and fourth year
students were recruited because both cohorts have taken the
preclinical MSK block offered towards the end of their second
year. Third year students were surveyed at the end of their
mandatory general surgery rotation at three major teaching
centers affiliated with Harvard Medical School: Massachusetts
General Hospital, Brigham and Women’s Hospital, and Beth
Israel Deaconess Medical Center. Fourth year students were
recruited through a combination of clinical electives, USMLE
Step II review sessions, and personal contacts.
Population Subgroup
In order to assess the required curriculum for all students
as well as the impact of taking MSK electives, the composition
for the participants of each class was divided between elective
and non-elective takers. First year MSK electives, which were
taken prior to medical school, include biomechanics focusing
on MSK related injuries and anatomy and physiology. Third
year MSK electives include two weeks of orthopedics during
their general surgery rotation and a course on advanced clinical
anatomy. Fourth year MSK electives include advanced clinical
anatomy, advanced MSK physical diagnosis, and one month of
adult or pediatric orthopedics..
Survey Instrument
All students filled out a two part instrument. The first part
was an attitudes questionnaire designed for: 1) determining the
students’ perception of the impact of MSK education on their
future medical career, 2) measuring the students’ confidence
in performing MSK physical examinations, and 3) gauging
the students’ satisfaction of their undergraduate medical curriculum.
The second part contained Freedman and Bernstein’s
validated MSK basic competency exam(2) and was used to
measure the students’ knowledge in MSK medicine. The exam
consisted of 25 short answer questions, and the answer key
and grading scheme used was identical to the one described in
their 2002 study. First year students were asked to complete
a shortened version of the survey instrument in order to minimize
their potential frustration in taking a lengthy examination
in which they had little or prior knowledge or training. The
shortened competency exam consisted of only five of the twenty-
five original questions, four of which are among the easiest
as determined by Freedman and Bernstein(2).
Attitudes Questionnaire
Students responded to a 5-category Likert scale (no,
minor, average, major, and critical importance) that gauged
their perceived importance of MSK education towards their
future medical career, regardless of residency interest. For
comparison, the same scale was used to measure the perceived
importance of pulmonary education. Pulmonary medicine was
chosen for comparison since MSK and respiratory symptoms
comprise the top two reasons that patients seek medical attention(
2,9,12). To guard against the tendency towards ranking
all topics as being of major importance, the relative importance
of MSK medicine was measured in relation to other major
courses covered during the first two preclinical years at Harvard
Medical School. Third and fourth year students were asked
to rank MSK medicine along with seven other topics in the
order of importance towards their future medical career. These
topics included major human body systems and basic science
courses all which have dedicated curriculum time greater
than the amount of time devoted to MSK medicine. Clinical
confidence was gauged by student responses to a 5-category
Likert scale (none, low, adequate, high, complete) measuring
their level of confidence in performing an overall MSK physical
examination and in generating a differential diagnosis for
pain. For comparison, the same scale was used to measure
confidence in performing a respiratory examination. The third
and fourth year student participants also rated the amount of
curricular time spent on MSK pathophysiology and medicine
at Harvard Medical School by responding to a 5-category Likert
scale (inadequate, poor, adequate, good, excellent). They were
also given the option of recommending changes (if any) to MSK
education at Harvard Medical School.
Statistical Analysis
All analyses were conducted using SPSS version 13.0
(SPSS Inc, Chicago, Ill). Two-way analysis of variance (ANOVA)
was used to characterize interactions of students’ importance
ratings of MSK and pulmonary education in each class. Paired
t-tests were used to compare importance ratings of MSK education
to pulmonary education. Student’s t-tests were used to
compare self-reported clinical confidence between elective and
non-elective takers, self-reported clinical confidence between
the MSK and pulmonary systems, and competency exam scores
between elective and non-elective takers. The Mann-Whitney
test was used to compare student importance rankings of the
eight topics. Statistical significance was assessed at p<.05 throughout.
RESULTS
Study Population
Overall response rates for the first, third, and fourth year
classes were 101/165 (61.2%), 120/184 (65.2%), and 80/153
(52.3%) respectively. Each class’s participation was divided
between elective and non-elective takers. Of the first, third,
and fourth year class, four (4%), sixty-five (54%), and twentyfive
(32%) of responding students had taken MSK electives.
Twenty-four out of the 120 third year students had already
seen Freedman and Bernstein’s competency exam and so only
their responses to the attitudes questionnaire were included in
analysis.
Student Attitudes
On average, medical students estimated that MSK problems
comprise between 40% and 45% of all primary care visits
(1st year: 44�18%, 3rd year: 41�19%, 4th year: 45�18%).
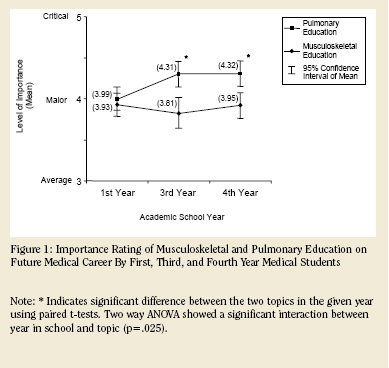
First year medical students did not indicate that there was a
significant difference in importance between MSK and pulmonary
education (p=.566), while third and fourth year students
deemed pulmonary education as being more important than
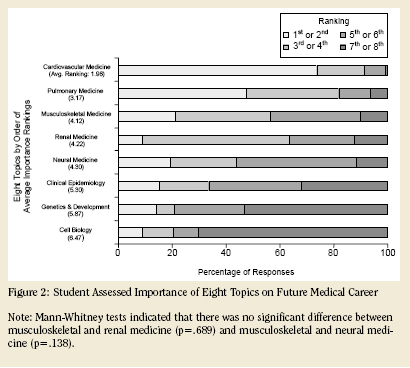
MSK education towards their future medical career (p<.001 for both groups, Figure 1). However, the ratings of both categories indicated that students in each year attributed both MSK and pulmonary education to be of �major importance� (score of 4/5). A two-way analysis of variance of academic year by topic revealed that as students progress into their clinical years, they feel that the relative importance of pulmonary education increases with respect to MSK education. When asked to rank 8 different preclinical curriculum topics, 3rd and 4th year students ranked MSK medicine as being the third most important topic to their future medical career, behind only cardiovascular and pulmonary medicine (Figure 2).
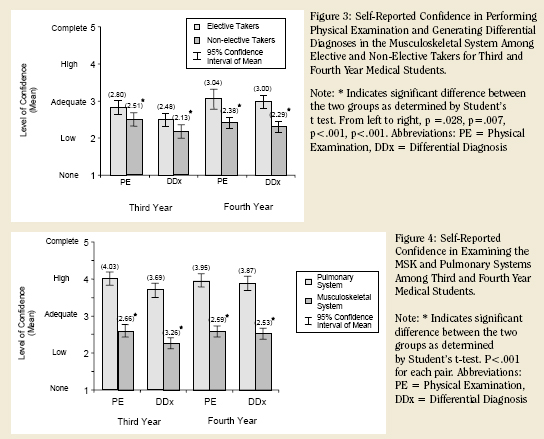
Third and fourth year medical students who have taken
MSK electives felt significantly more confident in performing
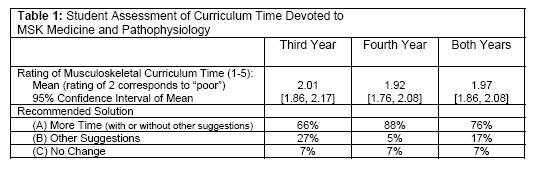
an MSK physical examination (3rd year: p<.05, 4th year: p<.001) and in generating a differential diagnosis (3rd year: p<.01, 4th year: p<.001) than those who have not taken any electives (Figure 3). A comparison between confidence in examining the MSK and pulmonary systems shows that while third and fourth year students generally felt a �high� (score of 4/5) level of confidence in examining the pulmonary system, the same students felt a �low� to �average� (score of 2/5 to 3/5) level of confidence in examining the MSK system (p<.001 for both years, Figure 4). Likewise, the students� confidence levels were significantly higher in generating a differential diagnosis for pain for the respiratory system (p<.001 for both years). Both third and fourth year students ranked the amount of curriculum time spent on MSK medicine as �poor� (score of 2/5), and 76% of these students recommended �more time� as a way to change the current MSK curriculum (Table 1).
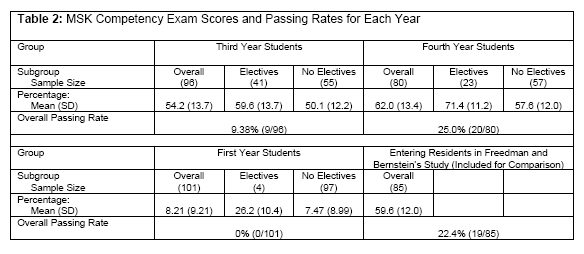
Competency Exam Results
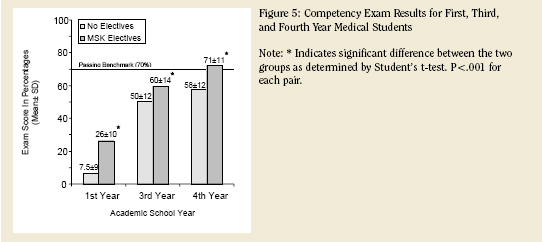
Both third and fourth year students who have taken
MSK related electives performed significantly better on the
competency test than those who have just taken the required
MSK curriculum (p=.001 for both groups, Figure 5). Overall
fourth year performance was not statistically different but was
slightly higher than the overall score of the entering residents
in Freedman and Bernstein’s study (4th Years: 62.0�13.4;
Residents: 59.6�12.0; p>.20). The overall passing rate on this
validated competency exam was 0%, 9.4%, and 25% for first,
third, and fourth years respectively (Table 2).
DISCUSSION
Despite the growing prevalence of MSK conditions and the
impact they have world-wide, these conditions have traditionally
suffered from a lack of attention because they are perceived
as being “less serious” than other disorders such as heart disease,
AIDS, and cancer(18). The designation of the years 2000
to 2010 as “The Bone and Joint Decade” was a global response
by the World Health Organization to outline strategies and
goals to address this lack of attention(19). The United States
adopted the National Bone and Joint Decade in 2002 as part of
this global initiative with the ultimate goal of reducing societal
burden arising from MSK conditions(20). Extending the collective
effort to the medical school level, the AAMC issued a MSOP
report in 2005 outlining MSK learning objectives in order to
assist medical schools in their efforts to improve education
about MSK conditions(1). However, there has been little direct
evidence supporting the need for MSK education reform at the
undergraduate level.
Previous studies have suggested that the discrepancy
between the magnitude of MSK problems and physician competency
in MSK medicine likely stems from educational deficiencies
at the medical school level(2,6-8). In 1998, Freedman
and Bernstein administered a basic MSK competency exam
to all 85 entering residents at the University of Pennsylvania
School of Medicine. According to a passing standard set by one
hundred and twenty four (81%) of all 154 orthopedic residency
program directors across the United States, seventy (82%)
of these first-year residents failed to
demonstrate basic competency in MSK
medicine as expected from medical
school graduates. A limitation of this
study was the potential bias of having
orthopedic residency directors set the
passing criterion. In 2002, the authors
addressed this limitation by re-validating
the basic competency exam, and a
different passing score was suggested by
two hundred and forty (58%) of all 417
internal medicine residency program
directors in the United States. Using
these new passing standards, however,
Freedman and Bernstein still found that
sixty-six (78%) of the entering residents
failed to demonstrate competency in
MSK medicine. From these results, the
authors suggested that undergraduate
medical education in MSK medicine is
insufficient. Results from our study,
which directly evaluated medical student
competency, validate their conclusion,
as 75% of our graduating class
failed to demonstrate competency using
the passing standard set by the internal
medicine residency program directors.
The first direct attempt at testing
Freedman and Bernstein’s hypothesis
at the undergraduate medical school
level was in 2005. Investigators from
the University of Washington Medical
Center administered modified versions
of Freedman and Bernstein’s validated
exam to the medical students. The
study divided the competency exam
into two shorter versions in part to increase response rate.
However, they attained responses from only 22% of the third
year and 29% of the fourth year class(3). Results of their study
indicated that the graduating class exhibited a passing rate of
43%, which is noticeably higher than the corresponding 25% at
our institution. A limitation of the University of Washington
study was the low response rate from their third and fourth
year medical students. Our study at Harvard Medical School
used the entire validated version of the basic competency exam
and recruited over 60% and 50% of the third and fourth year
students respectively.
 In addition to directly evaluating the medical students’
knowledge in MSK medicine, we also examined the attitudes
and perceptions of medical students toward MSK medicine
and the MSK curriculum. The responses suggest that medical
students are aware of the prevalence of MSK conditions and of
the relative importance of MSK education. They ranked MSK
medicine as being the third most important topic (tied with
neural and renal medicine) to their future medical career out
of eight topics. Furthermore, while students felt on average
that MSK medicine is of “major importance” towards their
future career, they also felt that the amount of curriculum
time devoted to MSK medicine was “poor”, with 76% of third
and fourth years recommending that more curriculum time be
devoted to the area.
In addition to directly evaluating the medical students’
knowledge in MSK medicine, we also examined the attitudes
and perceptions of medical students toward MSK medicine
and the MSK curriculum. The responses suggest that medical
students are aware of the prevalence of MSK conditions and of
the relative importance of MSK education. They ranked MSK
medicine as being the third most important topic (tied with
neural and renal medicine) to their future medical career out
of eight topics. Furthermore, while students felt on average
that MSK medicine is of “major importance” towards their
future career, they also felt that the amount of curriculum
time devoted to MSK medicine was “poor”, with 76% of third
and fourth years recommending that more curriculum time be
devoted to the area.
One way that students can remediate their deficiency in
this area is by taking MSK electives. Our results demonstrated
that both 3rd and 4th year students who had taken MSK electives
in their clinical years perform significantly better on the competency
exam and are significantly more confident in examining
the MSK system than those who had taken just the required
MSK curriculum. Despite that fact that most students from
our study seem to be aware of the importance and prevalence
of MSK conditions, however, only 54% of third years and 32% of
fourth years chose to take MSK electives. This data would suggest
that medical students themselves play a role in their relative
lack of competence and confidence in MSK medicine(4).
Nevertheless, as suggested by the AAMC MSOP report, more
attention needs to be devoted to the MSK curriculum at the
medical school institution itself. The students’ performance
in the competency exam along with their relative dissatisfaction
with the amount of curriculum time dedicated to this area
provide evidence of the need to re-examine the undergraduate
MSK medicine curriculum at Harvard Medical School.
RELEVANCE TO OTHER MEDICAL INSTITUTIONS
Harvard Medical School requires two weeks of preclinical
instruction focused on MSK medicine in the second year and
does not require a MSK clerkship during the clinical years. Of
the 122 medical schools in the continental United States and
Hawaii, fifty-seven schools (47%) do not require preclinical
nor clinical instruction in MSK medicine and fifty-four schools
(44%) require either preclinical or clinical instruction(4). Out
of the 16 Canadian medical schools, 11 (68%) do not require
MSK education in the clinical setting(
5). Thus approximately 90% of
United States and 70% of Canadian
medical schools devote a similar
amount of time to MSK medicine as
does Harvard Medical School(4,5).
Although individual institution’s
MSK curriculums vary in effectiveness,
it may still be reasonable to
infer that the majority of United
States and Canadian medical school
face a similar degree of deficiency in
MSK medicine education.
LIMITATIONS
Results from the study should
be interpreted within the context
of several limitations. First, there
may be selection bias among the
fourth year class, as 23 out of the
80 students surveyed participated by
attending an optional Step II MSK
boards review session. These participants
may have volunteered because of their self-perceived lack
of knowledge in MSK medicine and would therefore perform
worse on the exam. Student’s t-tests between those who took
the survey during the board review sessions and those who took
the survey elsewhere reveal no statistical difference in exam
scores (Boards: 58.7�14.6; Others: 63.4�12.1; p=0.146).
There was, however, a significant difference in the confidence
level in performing a physical examination on the MSK system
(Boards: 2.25�0.44; Others: 2.75�0.68; p<0.005). Second, MSK elective-takers may have performed better on the competency exam not because they took MSK electives, but because they have a higher level of interest in MSK medicine. To address this issue, we looked at the top residency choice for all twenty-five 4th year elective takers and found that 7 out of the 25 medical students listed orthopedics as their first residency choice. When competency exam scores of the 7 students interested in orthopedics were compared to the other 18 students, we found no statistical difference between the two groups� scores as shown by Student�s t-test (Orthopedics: 73.2�10; Others: 70.6�12; p="0.617)." This data suggests that the increase in MSK medicine competency is more strongly correlated to taking MSK electives than to interest alone. Third, this study is limited to a single institution; however, results are likely generalizable to other medical schools because of the similar required time dedicated to the MSK curriculums in over 90% of all United States medical institutions(4).
FUTURE DIRECTION
Harvard Medical School is currently in the midst of a major
undergraduate medical education reform. Instead of estimating
what adjustments are needed, the institution is in favor of
first assessing the effectiveness of the current MSK curriculum
before embarking on specific changes. As the AAMC suggested
in their MSOP guidelines, medical schools can better address
MSK education by striving to “integrate learning experiences
relevant to MSK medicine throughout the curriculum in ways
that explicitly identify the material as part of a coherent curriculum
component1”. A four-year MSK curriculum can aid in the
organization of the curriculum design and link together parts of
the MSK curriculum into various course blocks so that students
obtain a more comprehensive understanding and cohesive view
of MSK medicine. Results from our study as well as the one
at the University of Washington would support requiring MSK
training during the clinical years, as competency in MSK medicine
significantly increased when students were exposed to the
MSK clinical electives during their third and fourth years(3).
In conclusion, our study adds to the previous literature by
not only providing direct measurement of the effectiveness of
the undergraduate MSK education, but also by presenting the
medical students’ perspective towards MSK medicine and the
MSK curriculum. The increasing burden of MSK problems on
individuals and society mandates more focus on MSK medicine,
and a four year integrated MSK curriculum with dedicated
time spent in both preclinical and clinical years is one way that
medical schools can address this problem so that “young physicians
entering their residencies will feel as well prepared to deal
with such conditions as they are prepared to deal with problems
found in other body systems(6).
Charles S. Day, MD Department of Orthopedic Surgery, Beth Israel Deaconess Medical Center, Harvard Medical School
Albert C. Yeh Faculty of Arts and Sciences, Harvard College
Edward Krupat, PhD Director of Evaluation, Office of Educational Development, Harvard Medical School
Address correspondence to:
Charles S. Day, MD
Chief, Hand and Upper Extremity Surgery
Department of Orthopedic Surgery
Beth Israel Deaconess Medical Center
Harvard Medical School
330 Brookline Avenue – E/CC 2.
Boston, MA 02115
Phone: 617-667-2848
Fax: 617-667-2155
References:
- Association of American Medical Colleges. Contemporary issues in medicine: musculoskeletal medicine education. AAMC MSOP Report VII, 2005.
- Freedman KB, Bernstein J. Educational deficiencies in musculoskeletal medicine. JBJS(A), 84:604-608, 2002.
- Schmale GA. More evidence of educational inadequacies in musculoskeletal medicine. CORR, 437:251-259, 2005.
- DiCaprio MR, Covey A, Bernstein J. Curricular requirements for musculoskeletal medicine in American medical schools. JBJS(A), 85:565-567, 2003.
- Pinney SJ, Regan WD. Educating medical students about musculoskeletal problems: are community needs reflected in the curricula of Canadian medical schools? JBJS(A), 83:1317-1320, 2001.
- Clawson DK, Jackson DW, Ostergaard DJ. It’s past time to reform the musculoskeletal curriculum. Acad Med, 76:709-710, 2001.
- Bernstein J, Alonso DR, DiCaprio M, et al. Curricular reform in musculoskeletal medicine: Needs, opportunities, and solutions. CORR, 415:302-308, 2003.
- Freedman KB, Bernstein J. The adequacy of medical school education in musculoskeletal medicine. JBJS(A), 80A:604-608, 2002.
- Rosenblatt RA, Cherkin DC, Schneeweiss R, et al. The structure and content of family practice: current status and future trends. J Fam Pract, 14:681-722, 1982.
- De Lorenzo RA, Mayer D, Geehr EC. Analyzing clinical case distributions to improve an emergency medicine clerkship. Ann Emerg Med, 19:746-751, 1990.
- De Innocencio J. Epidemiology of musculoskeletal pain in primary care. Arch Dis Child, 2004:89:431-434.
- Kelsey, JL. Epidemiology of musculoskeletal Disorders. New York, Oxford University Press, 1982.
- National Center for Health Statistics, National Ambulatory Medical Care Survey, 1995. In MSK Conditions in the United States edited by Praemer A, Furner S, Rice DP. Ed. 2. Rosemont, IL: AAOS, 1999.
- Badley EM, Webster GK, Rasooly I. The impact of musculoskeletal disorders in the population: are they just aches and pains? Findings from the 1990 Ontario Health Survey, J Rheumatol, 21:505-514, 1994.
- Stewart WF, Ricci JA, Chee E, Morganstein D, Lipton R. Lost productive time and cost due to common pain conditions in the US workforce. JAMA, 11:291(6):694, 2004.
- Yelin E. Cost of musculoskeletal diseases: impact of work disability and functional decline. J Rheumatol Suppl. 68:8-11, 2003.
- Yelin E, Herrndorf A, Trupin L, Sonneborn D. A national study of medical care expenditures for musculoskeletal conditions: the impact of health insurance and managed care. J Arthritis Rheum. 44(5):1160-9, 2001.
- Delmas PD, Anderson M. Launch of the Bone and Joint Decade 2000-2010. Osteoporosis International, 11:95-97, 2000.
- Lidgren L. The Bone and Joint Decade 2000-2010: An update. Acta Orthop Scandinavica, 71(1):3-6, 2000.
- Weinstein SL. National Bone and Joint Decade: 2002-2011. Commentary on Proclamation. JBJS(A), 84(A):1298, 2002.
|