Proximal Tibial Lesion in a Young Adult: Early Diagnosis Allowing Unique Reconstruction
James B. Ames, MD, John A. Abraham, MD, David S. Geller, MD, Jeffrey Goldsmith, MD, Mark C. Gebhardt, MD
Beth Israel Deaconess Medical Center
CASE PRESENTATION
 History and Physical Examination
History and Physical Examination
The patient is a 21-year-old male high school custodian
who suffered acute onset of right knee pain one Friday in
December after a long day of work driving his pickup truck and
clearing snow. The pain persisted over the weekend becoming
severe enough on Sunday night that it woke him from sleep.
He was evaluated by his primary care physician the following
morning and found on exam to have medial joint line tenderness.
A possible intra-articular injury was suspected and the
patient was referred to a local orthopedic surgeon for evaluation.
Examination revealed pain with flexion of the knee beyond
90 degrees. Careful evaluation of the medial aspect of the knee
revealed pain with palpation of the proximal tibia just adjacent
to the medial joint line, but no actual joint line tenderness. Due
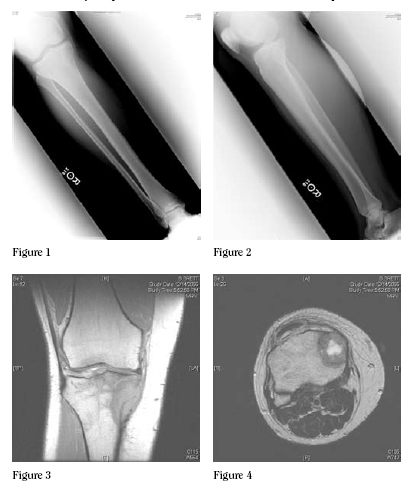
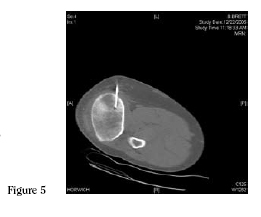
to this discrepancy, radiographs were obtained, which showed
a subtle radiolucent lesion in the proximal anteromedial tibial
metaphysis. This was recognized as an abnormality and an MRI
was ordered to more clearly define the lesion.
Imaging
Based on the imaging studies, what is your diagnosis and
how would you proceed with the evaluation of this patient?
Differential Diagnos
Benign lesions:
Giant Cell Tumor
Chondroblastoma
Aneurysmal Bone Cyst
Malignant lesions:
Osteosarcoma
Lymphoma
Ewing Sarcoma
 Histology
Histology
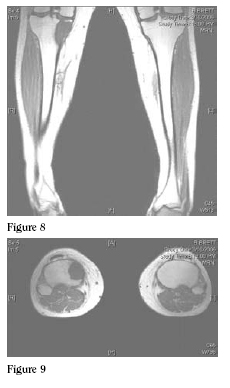
A CT guided needle biopsy
was obtained. Based on the histology,
what is your diagnosis?
Pathology and Further Workup
Histologic evaluation of CT guided core biopsies of the
lesion showed a spindled and epithelioid neoplasm with marked
cytologic atypia and atypical mitotic forms (Figure 6). Close
examination of the tumor showed, a pale-pink extracellular
matrix that is diagnostic of unmineralized bone or osteoid
(Figure 7). The combination of the malignant cytology and the
presence of osteoid are diagnostic of high-grade osteosarcoma.
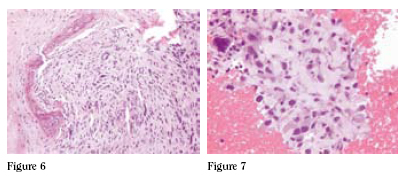
MRI showed the mass to involve the medial portion of the proximal
tibial metaphysis and epiphysis. Staging studies, including
computed tomography
scanning of the chest and
whole body bone scan,
were done which did not
show any evidence of
metastatic disease to the
lungs or other bony sites.
The patient was referred
to medical oncology for
induction of chemotherapy
for osteosarcoma. The
patient underwent three
months of neo-adjuvant
chemotherapy and then
underwent complete restaging
examinations followed
by operative resection
for local control of the
tumor. (Figures 8 and 9)
SURGICAL TREATMENT
Resection
The tumor was approached through a medial incision
extending from the medial femoral condyle to the mid portion
of the tibia. The biopsy site was kept in continuity with the
resected specimen. The saphenous vein was identified, dissected
and protected. The medial head of the gastrocnemius and
soleus were retracted posteriorly. The soleus arch was divided
while protecting the popliteal vessels. The pes anserine tendons
and semimembranosus were divided, and the medial meniscotibial
ligament was divided anteriorly as far as the patellar tendon.
The patellar tendon was preserved and retracted anteriorly.
The arthrotomy was extended posteriorly to the midline where
the popliteal vessels were again identified and protected. Care
was taken to preserve the entire medial meniscus. The anterolateral
tibia was then exposed by raising a large anterolateral
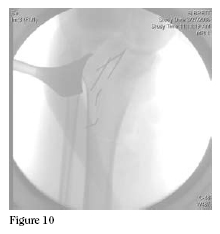
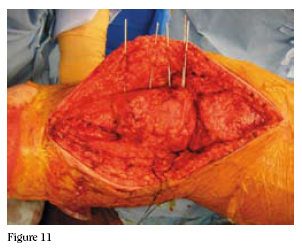
 flap. Then, using C-arm control, K-wires were placed outlining
the length and extent of our osteotomy. (Figures 10 and
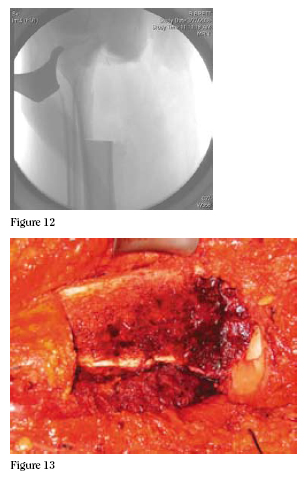
11) An oscillating saw and osteotomes were used to make the
osteotomy. We had direct visualization of the articular surface
at this point and placed the osteotome just medial to the tibial
spines, preserving the insertion of the cruciates by undercutting
of the tibial spines. The osteotomies were completed, the
specimen was passed off, and curettings were taken for a deep
margin. (Figures 12 and 13)
flap. Then, using C-arm control, K-wires were placed outlining
the length and extent of our osteotomy. (Figures 10 and
11) An oscillating saw and osteotomes were used to make the
osteotomy. We had direct visualization of the articular surface
at this point and placed the osteotome just medial to the tibial
spines, preserving the insertion of the cruciates by undercutting
of the tibial spines. The osteotomies were completed, the
specimen was passed off, and curettings were taken for a deep
margin. (Figures 12 and 13)
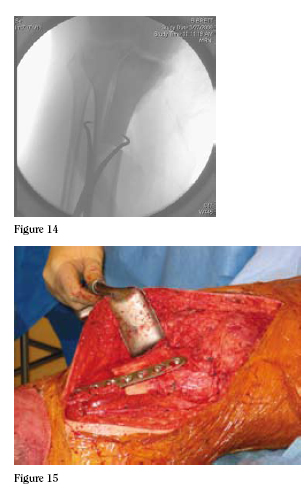
Reconstruction
An osteoarticular allograft had been thawed and cultured.
After getting confirmation of negative margins, we sculpted the
graft to fit the resection defect. (Figure 14) The meniscus from
the allograft was trimmed, leaving a small rim peripherally.
Sutures were then used to reattach the patient’s native menisco-
tibial ligament to the remaining rim of allograft meniscus.
An 8-hole narrow large fragment combi-plate was used to hold
the graft in place with two screws in compression across the
allograft-host junction. (Figure 15) The medial arthrotomy
was then closed, and the pes anserine tendons, MCL and medial
retinaculum were repaired. The subcutaneous tissues were
then closed in layers, the wounds were dressed, and the patient
was placed in a long posterior splint.
RESULTS
The patient was placed into a long leg cast and was given
instructions of touchdown weight bearing. He was allowed to
begin range of motion exercises approximately 6 weeks after
surgery.
DISCUSSION
 Patients with tumors about the knee present with a variety
of complaints that may initially be attributed to injuries or
other causes. A careful history and physical exam can often
lead to the proper diagnosis. Malignant lesions generally have
pain that is present at rest or at night, while benign lesions and
traumatic injuries are more likely to be painful with activity.
Identification of a palpable mass is a key finding on physical
exam and pain at the site of the mass or bony lesion must be
distinguished from joint line tenderness, tendonitis, or apophysitis
pain.
Patients with tumors about the knee present with a variety
of complaints that may initially be attributed to injuries or
other causes. A careful history and physical exam can often
lead to the proper diagnosis. Malignant lesions generally have
pain that is present at rest or at night, while benign lesions and
traumatic injuries are more likely to be painful with activity.
Identification of a palpable mass is a key finding on physical
exam and pain at the site of the mass or bony lesion must be
distinguished from joint line tenderness, tendonitis, or apophysitis
pain.
Sports related injuries are increasingly managed with
arthroscopy of the knee. Recent reports have described tumors
about the knee that were not initially recognized and were
treated as sports injuries – sometimes with arthroscopy. One
report showed that ultimate oncologic therapy was altered in
60% of these cases. The most common cause of these erroneous
diagnoses and treatments were insufficient or poor quality
radiographs.a
In this report we describe a case of a proximal tibial osteosarcoma
presenting with complaints suspicious for an intraarticular
injury. Careful and appropriate management by the
referring primary care physician and orthopaedic surgeon led to
timely diagnosis and treatment. A novel approach to resection
and reconstruction of this tumor is also described.
General Principles of Treatment
Current management of osteosarcoma requires a multidisciplinary
approach including a team of orthopedic oncologists,
pediatric oncologists, radiologists and pathologists. The
goal of treatment is to achieve local control of the tumor
and systemic control of the disease. Chemotherapy has been
the main factor in the increased survival rates seen over the
last several decades for patients with osteosarcoma. It is
imperative to think of high-grade osteosarcoma as a systemic
disease. For example, in patients with apparently isolated
osteosarcoma treated with amputation alone, metastatic disease
developed in 80-90% within the first two years following
surgery. This implies that the vast majority of patients have
undetectable micrometastatic disease at the time of initial
diagnosis. The addition of adjuvant chemotherapy to treat this
micrometatsatic disease has led to dramatic improvements in
disease free survival rates. Prior to the use of chemotherapy
the probability of remaining disease free after amputation for
osteosarcoma was less than 20%, the current probability is
estimated to be between 65 and 80%.b
Local Control

Amputation was once the standard of care for all patients
with high-grade osteosarcoma and remains an important tool in
the surgeon’s armamentarium. Currently however, the majority
of patients who present with osteosarcoma of all grades are
treated with limb-salvage surgery. Although randomized trials
have not been performed comparing survival rates of patients
treated with amputation versus limb salvage, non-randomized
retrospective studies do not show a survival advantage to treating
with amputation. Furthermore, an increase in local recurrence
with limb-salvage surgery has not been shown. With
amputation in some cases having poorer functional result than
limb salvage surgeryc d, and with the addition of chemotherapeutic
agents that are moderately to highly effective against this
tumor, limb salvage surgery has become the current standard
of care for treatment of most patients who present with osteosarcoma.
Reconstruction
The large majority of these tumors present in young
patients who are still growing or have recently completed
growth, as in this case presentation. The knee area (distal
femur and proximal tibia) is the most common site for
osteosarcoma, and several options have been developed for
reconstruction after resection of a malignancy from these
sites. Reconstruction options for various sites must be carefully
considered in order to maximize the patient’s result with
respect to function and durability. Particularly in the growing
child, reconstruction of a defect from a tumor resection can be
difficult and fraught with subsequent mechanical, wear-related,
and growth-related complications. Osteosarcoma about
the knee most commonly does not involve the joint itself,
and an intra-articular resection can usually be performed.e
Reconstruction can then be carried out with an osteoarticular
allograft, allograft prosthetic composite (APC), or a metallic
endoprosthesis. Metallic prostheses are more stable initially
and generally will return a patient to function earlier than an
allograft. However, concerns about loosening, particle disease
and overall implant longevity are a concern in this young
patient population.f2 Allografts require a longer post-operative
recovery period but have the advantage of restoring bone
stock. The first reported human osteoarticular allograft may
have been as early as 1902.g The longevity of articular cartilage
in osteoarticular allografts is indefinite, and some patients
will ultimately require traditional joint replacement surgery.
Other issues with allograft use include malunion or nonunion
at the osteosynthesis site, allograft fracture, joint laxity
and infection.h i In the case of the proximal tibia, allograft
reconstructions have the significant advantage of allowing
restoration of the extensor mechanism by reattachment of the
patellar tendon to the allograft tendon. The resulting extensor
mechanism is considered to be superior to the metallic
prosthesis, which relies on soft tissue ingrowth into a porous
surface on the implant. This type of reconstruction results in
an extensor lag that generally does not improve over time.
Hemicortical resection
In the case example presented here, a unicondylar wide
resection and reconstruction of a high-grade intramedullary
osteosarcoma of the proximal end of the tibia is described.
This type of resection and reconstruction is not commonly
performed for high-grade sarcomas because of the concern for
local recurrence. Whereas intramedullary margins have been
described for benign and low grade malignant tumors, this
case presents the use of this type of resection for a high grade
malignant osteosarcoma, because it was felt preoperatively that
adequate margins could be obtained.
The question of what distance of normal marrow defines
an adequate bony margin for a high grade osteosarcoma has
not been adequately described in the literature. Traditionally,
a resection of the entire segment of bone containing a 3-5cm
margin has been considered adequate.j2 However, recent evidence
from successful treatment of low grade parosteal osteosarcoma
without resection of the entire segment (hemicortical
resection) and with bony margins closer than previously
required has given credence to the thought that this type of
resection may be useful in the treatment of high grade osteosarcoma
as well. Several studies have shown that focal intramedullary
involvement in the case of surface osteosarcoma does not
increase the risk of local recurrence as long as the margin is
tumor-free.k l m n Further follow up on this patient will be necessary
to determine whether or not there is an impact on local
recurrence rate in this case, but if the suggestion from current
data on lower grade osteosarcoma holds true in the higher
grade cases, there should be no impact. A lengthy discussion
was had with the patient about the alternatives to this type of
resection, including amputation, and he was made aware of the
risks and benefits of this type of resection and reconstruction.
The difficulty in achieving a negative margin must be also
be considered in this case. The hemicortical resection described
here is technically demanding, and may significantly increase
the risk of obtaining an intra-operative cut through bone containing
tumor. Adequate and precise imaging both pre and post
neo-adjuvant chemotherapy is therefore a prerequisite for any
tumor for which this type of reconstruction is being considered.
The lack of an intra-operative imaging modality that can
identify the exact location of a tumor in the bone (such as MRI)
makes this type of resection challenging. This type of resection
is therefore not recommended for all tumors in this location,
and may only apply to a select subset of tumors such as the one
presented here where the anticipated benefit of hemicortical
resection outweighs the presumed additional risk. In this case,
the described resection allowed preservation of the native cruciate
ligaments, which should significantly improve the patient’s
functional outcome.
Current reports have demonstrated that proximal tibial
osteoarticular allograft reconstruction compare favorably to
metal endoprosthetic reconstruction in this location, and probably
have improved long term function because of the ability
to salvage the patellar tendon attachment.o In the described
resection, the majority of the functional components of the
joint are preserved, including not only the anterior and posterior
cruciate ligaments, but also the lateral collateral ligament
and greater than 50% of the articular cartilage of the tibial
plateau. Presumably this joint preservation will translate into
further improvements in graft survival and long-term function.
Although it remains to be seen whether there is additional risk
in terms of local recurrence with this type of resection, these
potential benefits must be considered.
In terms of allograft incorporation, multiple current studies
suggest that allograft incorporation in the metaphyseal region
is faster when compared to the diaphyseal region. Allograft
reconstruction in metaphyseal osteotomies heal at an average
of 6 months compared to a range of 9 to 18 months for diaphyseal
osteotomies.p q r It is not clear whether this is a function of
surface area or some other phenomenon, as at least one study
comparing oblique osteotomies, to transverse osteotomies, the
former having greater surface area than the latter, failed to show
a significant difference in healing times.s11 Nonetheless, the
broad metaphyseal surface area of the osteotomy described in
this surgical technique may lead to an accelerated healing time
in this hemicortical resection as compared to standard osteoarticular
reconstructions in this region in which the allografthost
junction is entirely diaphyseal.
Summary and future directions
The case presented in this article represents an unusual
circumstance in which a hemicortical intramedullary resection
could be performed for a high-grade malignant osteosarcoma
of the proximal tibia. This was possible in large measure by
the astute, early diagnosis made by the referring orthopaedic
surgeon and should remind all practicing orthopedic surgeons
to have a high index of suspicion in evaluating young patients
with atypical knee pain. It is our hope that with current modern
chemotherapy resulting in 95% or greater tumor necrosis
as in this case, that the resection described above with allow
adequate local control without any increased risk of local
recurrence, while offering significantly improved durability and
function compared to other standard reconstruction options.
Careful follow up over the next several years will be required
to demonstrate this. The future direction for this research, of
which this patient represents the first step, should be to set up
a prospective trial for patients that could reasonably undergo
this type of procedure to see if statistically significant differences
exists between the described resection and standard
resections.
James B. Ames, MD is a Resident, Orthopaedic Surgery, Dartmouth Orthopaedic Residency Program.
John A. Abraham, MD is a Fellow, Orthopaedic Oncology, Harvard Combined Orthopaedic Oncology Fellowship.
David S. Geller, MD is a Fellow, Orthopaedic Oncology, Harvard Combined Orthopaedic Oncology Fellowship.
Jeffrey Goldsmith, MD, Department of Surgical Pathology Beth Israel Deaconess Medical Center.
Mark C. Gebhardt, MD, Frederick W. and Jane M. Ilfeld, Professor of Orthopaedic Surgery, Harvard Medical School. Chairman, Department of Orthopaedic Surgery, Beth Israel Deaconess Medical Center.
Address correspondence to:
Mark C. Gebhardt M.D.
Beth Israel Deaconess Medical Center
330 Brookline Ave
Boston, MA 02115
References:
- Muscolo DL, Ayerza MA, Makino A, et al. Tumors about the knee misdiagnosed as athletic injuries. J Bone Joint Surg 85A;7:1209-1214. 2003
- Herring, JA, ed. Malignant Bone Tumors, in Tachdjian’s Pediatric Orthopaedics, 3 ed. Philadelphia: Sunders. 2002
- Harris IE, Leff AR, Gitelis S, Simon MA: Function after amputation, arthrodesis, or arthroplasty for tumors about the knee. J Bone Joint Surg 72A:1477-1485, 1990.
- Renard AJ, Veth RP, Schreuder HW, et al: Function and complications after ablative and limb-salvage therapy in lower extremity sarcoma of bone. J Surg Oncol 73(Suppl):198-205, 2000
- Unni, K.K., ed. Dahlin’s bone tumors:General aspects and data on 11,080 cases.5th ed. Philadelphia: Lippincott-Raven 1996.
- Parrish, FF: Allograft replacement of all or part of the end of a long bone following excision of a tumor. JBJS 55A, 1-22, 1973
- Brigman BE, Hornicek FJ, Gebhardt MC, Mankin HJ: Allografts about the knee in young patients with high-grade sarcoma. Clin Orthop 421 232-239, 2004
- Clohisy DR, Mankin HJ: Osteoarticular allografts for reconstruction after resection of a musculoskeletal tmor in the proximal end of the tibia. JBJS 76A, 549-554, 1994
- Lewis VO, Gebhardt MC, Springfield DS: Parosteal Osteosarcoma of the posterior aspect of the distal part of the femur: oncologic ad functional results following a new resection technique. JBJS 82A(8) 1083-1088, August 2000
- Campanacci M, Picci P, Gherlinzoni F, Guerra A, Bertoni F, Neff JR: Parosteal Osteosarcoma JBJS, 66B(3):313-321, 1984
- Okada K, Frassica, F; Sim, FH; Beabout, JW; Bond JR; Unni, KK: Parosteal Osteosarcoma. A clinicopathological study. JBJS 76-A; 366-378, March 1994
- Deijkers, RLM; Bloem RM; Hogendoorn PCW; Verlaan JJ; Kroon HM; Taminiau AHM: Hemicortical allograft reconstruction after resection of low-grade malignant bone tumours. BJBJS 84B; 1009-1014, September 2002.
- Gebhardt MC, Flugstad DI, Springfield DS, Mankin HJ: The use of bone allografts for limb salvage in high-grade extremity osteosarcoma. CORR 270: 181-196, Sept. 1991
- San Julian Aranguren, M, Leyes, M, Mora, G, Canadell, J: Consolidation of massive bone allografts in limb-preserving operations for bone tumours. Internat Orthop 19; 377-382, 1995.
- Mankin H, Springfield D, Gebhardt M, Tomford W: Current status of allografting for bone tumors. Orthopedics 15: 1147-1154. 1992.
- Vander GR: The effect of internal fixation on the healing of large allografts. JBJS 76: 657-664, 1994
|