
A Brief Guide to Initial Management of Orthopedic Injuries in the Emergency Department
Harry M. Lightsey, IV, MD*, Caleb M. Yeung, MD*, Arvind von Keudell, MD
*Denotes equal contribution
The authors report no conflict of interest related to this work.
©2019 by The Orthopaedic Journal at Harvard Medical School
Orthopedic injuries are some of the most common reasons for patient presentation to the emergency department. Although the full spectrum of orthopedic injuries is broad, we have compiled a non-exhaustive guide regarding the most commonly seen orthopedic injuries. While patients often require individual care that does not always fit into generic algorithms for treatment, we hope that the following guide will provide a concise and useful summary of relevant presentations, pertinent exam findings, and initial steps in the management of patients in the emergency department with orthopedic injuries.
LEVEL OF EVIDENCE Level V Expert Opinion
KEYWORDSTrauma, management, fractures, splinting, X-rays, emergency department
Clavicle Fractures
Presentation
Young active patients after fall on outstretched arm or landing on lateral shoulder
Exam
Bruising or deformity over clavicle, potential skin tenting
Management
- Obtain clavicle as well as chest XR for contralateral comparison
- Proximal third (15%)
- Typically higher energy injury
- Check for other chest injuries
- Consider CT scan to ensure no SC joint dislocation
- If anteriorly dislocated - may manage conservatively in sling
- If posteriorly dislocated - will need operative intervention given danger to major vessels and airway
- Middle third (80%)
- >2cm shortening, >100% displaced, and/or significantly comminuted - may benefit from operative management given better short-term outcomes and lower nonunion rates1
- Distal third (5%)
- Most often managed non-operatively with sling immobilization
- Nonunion predictors - female, significant displacement, comminution, advanced age
Proximal Humerus Fractures
Presentation
Most commonly seen in the elderly after fall onto shoulder
Exam
- Bruising and swelling over deltoid or shoulder
- Arterial injury is rare, but check for intact radial pulse
- Axillary nerve is most commonly injured, check if patient can fire deltoid
Management
- Obtain full set of shoulder XRs - Grashey (true AP), scap Y lateral, and axillary lateral view.
- If patient cannot tolerate abduction of the arm, obtain Velpeau view
- If greater tuberosity is significantly displaced >5 mm, the fracture involves the joint surface with >2mm of displacement, or there is >100% displacement of the surgical neck of the humerus, and if the patient may be an operative candidate (young and active) - consider non-contrast CT scan.
- Check for glenohumeral joint dislocation - Dislocations with associated isolated greater tuberosity fracture can be reduced under conscious sedation. - one attempt only
- The humeral head may appear inferiorly subluxated - this is typically pseudosubluxation as a result of deltoid inhibition and intra-articular hematoma formation and does not represent a true dislocation
- Frequently managed non-operatively with sling immobilization and initiation of pendulum swings in 2-3 days. Follow up in orthopedic trauma clinic in 1-2 weeks.
- Surgical options may be considered for specific fracture patterns in younger patients.2
Shoulder Dislocation
Presentation
Majority are anterior shoulder dislocations, typically after fall with arm abducted and extended and/or with posteriorly directed force
Exam
- Palpable sulcus over glenohumeral joint and prominence anteromedially indicating an anterior dislocation
- Arm held abducted or above head (luxatio erecta) indicating an inferior dislocation
- Palpable sulcus posterolaterally under the acromion
- Assess for axillary nerve function
Management
- Inject 10-15 cc of 1% lidocaine without epinephrine for intra-articular hematoma block.
- Palpate sulcus over posterior shoulder - lidocaine should inject easily into the glenohumeral joint
- May use sheet around torso to help with counter-traction for abduction, external rotation, and axial traction moments for reduction of anterior shoulder dislocations
- There are various reduction maneuvers and different patients may require different techniques; familiarity with multiple maneuvers is helpful.3
- Place into sling immediately after reduction
- Obtain post-reduction shoulder films - if patient cannot tolerate axillary view, obtain Velpeau view. A scapular Y view may be inadequate to definitively confirm reduction.
- Maintain sling until follow up in clinic in 1 week
Humeral Shaft Fractures
Presentation
Bimodal (young patients with high-energy trauma and elderly patients with low-energy mechanisms)
Exam
- Check skin integrity to rule out open fracture
- Most common nerve injury is the radial nerve as it wraps around the humerus in the spiral groove - check for EPL function (thumb retropulsion: place hand flat on a table and lift up the thumb) and wrist extension
Management
- Obtain full length views of the humerus, consider addition of dedicated shoulder or elbow films if any concern for concomitant injury
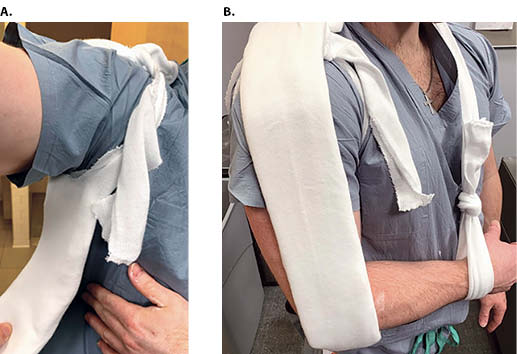
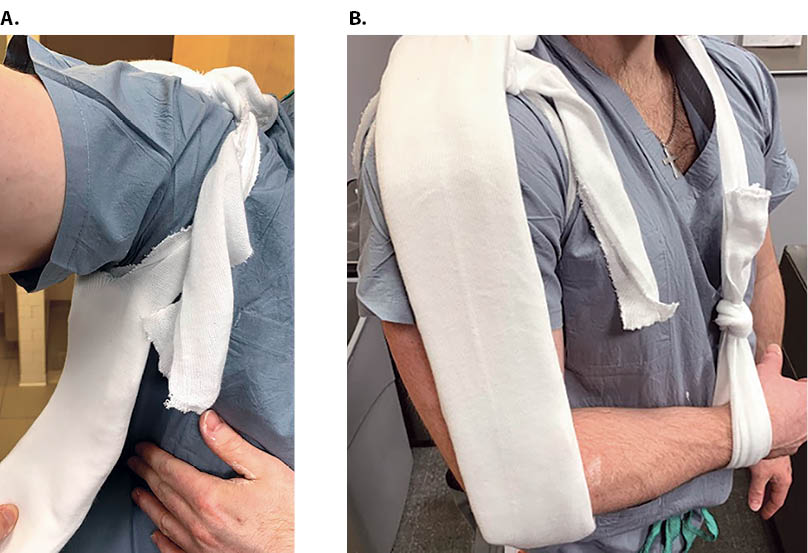
- Place arm into coaptation splint
- Obtain several feet of 4-inch stockinette, 4-inch plaster, ACE bandages, and several ABD pads
- Measure out splint appropriately - tuck one end of splint into axilla, then run the splint along the medial arm, around the elbow (flexed to 90 degrees), then along the lateral arm to just over the shoulder
- Use 10-12 layers of plaster and 5 layers of webril
- After wetting plaster, tunnel splint into stockinette. Place ABD pads into the stockinette to provide padding at appropriate points around the neck and wrist.
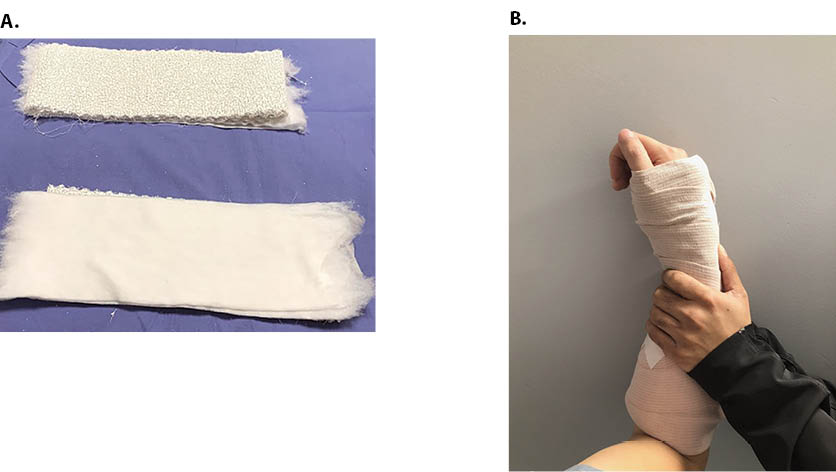
- Split one end of stockinette and tie around the shoulder to secure one end of splint into axilla (Figure 1A).
- Take free end of the stockinette and wrap over shoulder and around neck. Wrap the stockinette around the ipsilateral wrist so that the arm is maintained in adduction (Figure 1B). Wrap the arm with ACE bandage.
- Place a gentle mold on the lateral aspect of the splint to counter varus deforming forces.
- Obtain post-splinting films of the humerus
- Follow up in 1 week in ortho trauma clinic for transition into a Sarmiento brace
- Indications for surgical management include - polytrauma, open fracture, vascular injury, ipsilateral articular fractures, and floating elbow injury4
Distal Humerus Fractures
Presentation
Often after direct impact to elbow or axial loading mechanism
Exam
- Swelling over elbow with deformity
- Check for clinical position of elbow to assess for dislocation or fracture- dislocation
- Distal neurovascular status
Management
- Typically require surgical repair, ORIF preferred over elbow arthroplasty (except in elderly patients with highly comminuted fractures) in enabling early motion5
- Avoid ROM of the elbow as this can lead to neurovascular injury
- It may be helpful to obtain a traction view in the ED to assess for fracture pattern in highly comminuted and shortened fractures
- Typically admitted for operative intervention
- Place into a temporary posterior slab splint
- CT scan is often useful for determining fracture pattern if traction view is not tolerated or is insufficient
- Perform serial neurologic examinations as there can be a risk for compartment syndrome
Elbow Dislocation
Presentation
Majority are posterolateral dislocations in younger patients
Exam
- Evaluate skin for open injury
- Distal neurovascular status
- Shoulder/wrist exams
Management
- Obtain elbow XRs and determine if simple dislocation or if there areis associated fractures - if associated fractures, determine if any of these are intra-articular fragments that may block reduction
- Obtain 10cc of 1% lidocaine without epinephrine for intra-articular block
- Inject lidocaine posterolaterally in the center of the triangle formed by radial head, lateral epicondyle, and olecranon - in the dislocated elbow, this target will be a much larger sulcus
- Prepare a posterior elbow slab splint
- With arm in supination (shifts coronoid under trochlea), pull axial traction and put direct pressure on the olecranon to push it forward while flexing elbow
- After reduction, test for stability of elbow in varus and valgus stress, and range elbow in flexion-extension arc to determine stability
- Place into posterior slab splint and obtain post-reduction XRs. If any concern for fracture or incongruency of joint, obtain CT scan
- For simple dislocations, follow up in orthopedic clinic in 1 week to begin early motion
- For complex dislocations (i.e. concomitant fractures of the elbow), may admit these for fixation, or if reduced well and patient prefers, can be discharged with follow up within 1 week for discussion of possible operative fixation6
Both Bone Forearm Fractures
Presentation
Typically after fall from height with axial load or direct blow to forearm
Exam
- Usually obvious angular deformity of the forearm with possible skin tenting
- Assess for median nerve palsy (flexion of thumb IP and index DIP, “A-OK” sign)
- High risk for compartment syndrome (pain with passive movement of wrist or digits), especially in more complex or multipart fracture patterns7
- May also present with pain at elbow due to distal humerus fracture (floating elbow)
Management
- Typically admitted for surgical fixation
- Place into sugar tong splint - can use gentle traction to improve any gross deformity, but extensive reduction is not undertaken with these fractures
- Sugar tong splint - wraps from volar aspect of forearm starting at the MCPs around the posterior elbow to the dorsal MCPs. Use 8-10 layers of plaster and 5 layers of Webril. Wrap with ACE bandage.
- Serial compartment checks - do not block these patients
Distal Radius Fractures
Presentation
Most common orthopedic injury, bimodal (young patients with high energy trauma and elderly patients with falls onto outstretched arm)8
Exam
- Typically visible deformity, evaluate skin for open injury
- Assess distal neurovascular status (particularly median nerve function - displaced distal radius fractures may predispose to acute carpal tunnel syndrome characterized by escalating pain, numbness, and tingling in the palmar aspect of the thumb and index/middle fingers)
Management
- Obtain 10cc of 1% lidocaine without epinephrine for hematoma block
- Palpate fracture site dorsally - aim needle obliquely distally to position into fracture site
- Draw back on needle prior to injecting - if at the site of fracture/hematoma, should have a flash of blood into the syringe
- Inject 8-10cc into fracture site
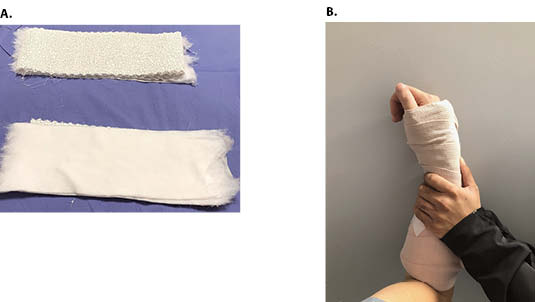
- Prepare dorsal volar slab splint - two slabs of plaster that extend from just proximal to MCPs to proximal forearm. Use 10 layers of plaster and 5 layers of webril (Figure 2A).
- Distal radius reductions can be helped tremendously by traction and should aim for preservation of soft tissue envelope8
- Suspend the upper extremity from IV pole with Kerlix looping around thumb and index finger. Position the elbow at 90 degrees, with the arm parallel to the floor.
- Apply 5 to 10 pounds of weights to the upper arm. This can be accomplished with several bags of saline. Make sure the Kerlix does not dig into the skin and this should be padded well with ABD pads.
- Typically hang arm for 10 minutes to help provide traction for reduction.
- Reduction maneuver is a combination of traction, recreation of the deformity to unhinge the fragments, and ulnar deviation.
- Apply dorsal and volar slab splints - do not extend beyond MCPs. Make a three-point mold such that the most distal mold puts pressure against the distal fracture fragment to hold it in place, the second mold on the opposite side of the arm and slightly more proximal up the arm providing counter-pressure, and the third mold being the most proximal (just proximal to the second mold) and on the same side as the first mold, providing counter-pressure to the second mold (Figure 2B)
- Obtain post-reduction films
- Does not typically require orthopedic admission, follow up in 1 week in orthopedic clinic
Pelvic Ring Fractures
Presentation
Bimodal (in young patients, almost always from high energy trauma - struck by car, rolled over by vehicle; in older population, can result from ground-level fall onto side)
Exam
- Pain with with lateral compression of pelvis
- Blood in the rectal or vaginal vault (open pelvic fracture), bruising over lower abdomen, blood in urine (often with concomitant bladder or urethral injury)
Management
- Assess hemodynamic stability and follow appropriate trauma algorithm9,10
- Obtain AP pelvis XR in the trauma bay
- If hemodynamically unstable, resuscitate 1:1:1 ratio of packed red blood cells, fresh frozen plasma and platelets, and apply pelvic binder centered over greater trochanters
- May require urgent stabilization in the operating room
- If hemodynamically stable, obtain CT pelvis in addition to AP radiograph
- May require orthopedic intervention (non-urgently) after trauma workup depending on the specific type of pelvic ring fracture
Acetabular Fractures
Presentation
Bimodal (high energy trauma in younger patients such as MVCs and low energy mechanisms in older patients such as fall from standing); outcomes typically worse in the elderly11
Exam
- Pain with axial loading of the femur and with log roll
- Assess distal neurovascular status
Management
- Obtain Judet views (obturator oblique and iliac oblique to assess column or wall involvement)
- If the hip is unstable, if there is incongruity of the femoral head within the acetabulum, or if there are incarcerated fragments within the weight-bearing portion of the joint, place femoral traction pin
- After femoral traction, CT pelvis is typically required
Hip Dislocation
Presentation
Bimodal (in young population, usually after axial loading mechanism to hip directed through a flexed hip - sitting in car/car crash; in elderly, often due to flexion and internal rotation of the hip, commonly in the setting of a prosthetic hip replacement)
Exam
- Leg typically shortened and internally rotated
- Assess for distal motor/sensory function (rule out sciatic nerve palsy)
Management
- In a native hip (i.e. no joint replacement), atraumatic reduction is done emergently to restore blood supply to the femoral head
- Assess for concomitant femoral neck fracture, particularly in the case of high energy mechanism
- Prepare patient for conscious sedation
- In a prosthetic hip, determine if the hip has a constrained liner or is a dual-mobility hip - these often cannot be close reduced and must be addressed with open reduction
Proximal Femur Fractures
Presentation
Usually after ground-level fall in older population or with high energy trauma in younger population
Exam
Deformity and swelling of proximal thigh, may have significant muscle spasm and shortening of leg
Management
- Four basic types - femoral head and femoral neck fractures are intracapsular while intertrochanteric and subtrochanteric fractures are extracapsular
- Displaced femoral neck fractures in the young patient are taken to the operating room for closed versus open reduction and internal fixation as soon as feasible13
- Obtain AP and cross table lateral views, traction views if needed - typically in fracture patterns where it is difficult to distinguish the level of the fracture or the fracture pattern
- Will most likely require operative fixation
Femoral Shaft Fractures
Presentation
Usually after high energy trauma in both younger and older populations, with exception of atypical femoral shaft fracture in older patients on bisphosphonate therapy
Exam
- Swelling, deformity, and muscle spasms of the thigh
- Assess thigh and distal neurovascular status
Management
- AP and lateral views of full-length femur, hip, knee
- If displaced and significantly shortened, may require tibial traction pin placement
- In the case of high energy mechanism, obtain CT hip to ensure no concomitant femoral neck fracture
- Roughly 9% of femoral shaft fractures will have a femoral neck fracture which is often vertically oriented and nondisplaced or minimally displaced14
Distal Femur Fractures
Presentation
Bimodal (after high energy trauma in younger population or after ground level fall or axial load onto knee in older population)
Exam
- Knee pain and swelling, deformity
- Evaluate skin integrity and vascular status
- Potential injury to the popliteal artery should be assessed with ABIs (if ABI <0.9, obtain CTA)
Management
- Obtain AP, lateral, and traction view. Obtain CT imaging if suspicion for a Hoffa’s fragment (fracture in the coronal plane of the distal femur) or if traction view is insufficient to elucidate fracture pattern
- Often complex, intraarticular, and comminuted fractures regardless of etiology15
- Place into knee immobilizer. Severely comminuted injuries should be placed in long leg splint
Patellar Fractures
Presentation
Most often occurs in younger male population through direct impact mechanism
Exam
- Palpable patella defect with hemarthrosis
- Straight leg raise test to assess the integrity of the extensor mechanism
Management
- Obtain AP, lateral, and sunrise views of the knee
- Obtain US if XRs show no fracture but patient is unable to extend at knee - may indicate a quad tendon or patellar tendon rupture
- Bipartite patellas may be mistaken for fracture (generally superolateral) - check for lipohemarthrosis on cross-table lateral X-rays which indicate an acute fracture
- In a patient with a nondisplaced fracture and intact extensor mechanism, this may be treated non-operatively. Place into knee immobilizer and follow up in orthopedic trauma clinic in 1 week
- Surgery is necessary for fractures disrupting the extensor mechanism and those with >2 to 3 mm step-off and >1 to 4 mm of displacement16
Proximal Tibia Fractures
Presentation
After laterally-directed or axial force onto knee
Exam
- Knee swollen, unstable to varus or valgus stresses
- Assess leg compartments (pain with passive movement of ankle or toes, paresthesias in foot) and distal neurovascular status
Management
- Tibial plateau and proximal third tibial shaft fractures
- Obtain AP, lateral, oblique views, CT scan if there is involvement of the tibial plateau
- Lipohemarthrosis indicates occult fracture – obtain a CT scan
- Minimally displaced tibial plateau fractures can typically be managed non-operatively with good functional outcomes17
- Prepare long leg splint if tibial shaft fracture - use 10-12 layers of 6 inch plaster for posterior slab (extends from posterior proximal thigh down to just past the tips of the toes) and 10-12 layers for the stirrup - should wrap around heel on sides of ankle up to mid-thigh both medially and laterally
- If tibial plateau fracture, place into knee immobilizer if unicondylar fracture; long leg splint if comminuted (complete articular fracture)
- Serial compartment checks
Tibial Shaft Fractures
Presentation
After high energy injury in young people (fall from height, laterally directed force), or after twisting injury in elderly
Exam
- Visible deformity of tibia, evaluate skin for open injury
- Assess leg compartments and distal neurovascular status
Management
- Obtain full length AP, lateral views, of the tibia, ipsilateral knee and ankle
- Obtain CT if there is intra-articular fracture extension or suspicion of joint involvement
- Prepare long leg splint - see proximal tibia fractures
- Management of open tibial shaft fractures with urgent debridement and external fixation vs. primary intramedullary nailing is an ongoing discussion in the literature18
- Serial compartment checks
Tibial Plafond/Pilon Fractures
Presentation
High energy axial load to the ankle in younger patients
Exam
Assess soft tissue integrity, stability and alignment of the ankle, and distal neurovascular status
Management
- Obtain ankle AP, lateral, mortise views as well as full length tib/fib and foot films
- May need CT to better assess intra-articular involvement, however this often is not done until after placement of an external fixator, which elucidates comminuted fracture patterns through traction and ligamentotaxis
- Prepare short leg splint – see ankle fractures
- Depending on degree of comminution and soft tissue compromise, consider early application of external fixator19
Ankle Fractures
Presentation
Usually after twisting mechanism in both young and old populations
Exam
- May have extensive skin bruising or swelling, obvious deformity of ankle
- Evaluate skin for open injury
Management
- Obtain ankle AP, lateral, mortise views
- If there is a fibula fracture at or below the level of the syndesmosis, and there is a congruent ankle mortise (joint space appears symmetric all around the talus), place into a long aircast boot for a trial of weight bearing as tolerated - follow up in ortho trauma clinic in 1 week for repeat XRs of the ankle. These injuries do well with non-operative management20
- If apparent isolated medial malleolus fracture, obtain full length tib/fib films as this may be a Maisonneuve fracture (fracture of the proximal fibula with syndesmotic injury)
- Most ankle fracture/dislocations can be closed reduced with the Quigley Maneuver (with the exception of ankle fractures with a vertical medial malleolar fracture).
- Obtain 10cc of 1% lidocaine without epinephrine for hematoma block medial to the tibialis anterior tendon
- Place in short leg splint: use 10-12 layers of 6 inch plaster for posterior slab (extends from posterior proximal leg down to just past the tips of the toes) and 10-12 layers for the stirrup - should wrap around heel on sides of ankle up to mid-leg both medially and laterally (Figure 3A). Ensure adequate plaster foot plate that extends past and protects the toes (Figure 3B).
- Flex the knee and apply a posterolateral to anteromedial directed force to the hindfoot with the distal hand by cupping the lateral aspect of the foot and heel while applying counterpressure with the proximal hand just superior to the medial malleolus (Figure 3C).
- If relatively simple ankle fracture pattern and the reduction is sufficient (i.e. congruency of the joint is restored well), the patient can be non-weight bearing and can follow up in orthopedic trauma clinic in 1 week for discussion of fixation
- Patients with ankle fractures with swollen skin and absent wrinkle sign will often be discharged and will return to clinic for scheduled fixation as their skin will not be amenable to fixation within 1-2 days

Foot Fractures
Presentation
Often after fall from height (calcaneus) or direct impact (car rolled over foot, kicked hard object)
Exam
- Swelling and focal pain over fracture site in foot
- May have threatened or tented skin in calcaneus fractures
- If fall from height, may have lumbar spine pain indicating concomitant spine injury - obtain spine imaging
Management
- Most metatarsal fractures can be placed into hard-soled shoes and allowed to weight bear as tolerated with the exception of first metatarsal fractures, which should be made non-weight bearing in a hard-soled shoe with plan to follow up for fixation in orthopedic clinic
- 5th metatarsal base fractures - classified into Pseudo Jones fractures and Jones fractures
- Jones fractures have a fracture line exiting into the space between the 4th and 5th metatarsals. Pseudo Jones fractures have a fracture line exiting into the articulation between the cuboid and the 5th metatarsal base
- Jones fractures - non-weight bearing in an aircast boot or hard soled shoe
- Special consideration of operative management for high-level athletes21
- Pseudo Jones fractures - weight bearing as tolerated in an aircast boot or hard soled shoe
- Both can follow up in orthopedic trauma or foot and ankle clinic in 1-2 weeks
- Talus fractures typically require orthopedic consultation and operative fixation - if displaced or dislocated will require reduction, often with sedation
- Talar process fractures can be subtle on plain films and often require CT22
- Calcaneus fractures are particularly morbid. Assess for soft tissue integrity and skin blanching and place into plantarflexion if significant posterior skin tenting – this may require urgent surgical management
- Prepare for bulky Jones splint - short leg splint with 10x padding and webril, particularly padded around the heel
Management of Compartment Syndrome
Presentation
Often occurs in the setting of trauma/fractures but can also result from burns, tight casts or wraps, bleeding, IV extravasation, reperfusion injury
Exam
Significant pain especially with passive stretch, tense or woody compartments, paresthesias. Anesthesia and paralysis are late findings.
Management
- Primarily clinical diagnosis but can be supplemented with direct compartment measurements
- High suspicion and frequent serial checks very important
- Elevation to 20-30 mm Hg below the diastolic pressure (Δp) is typically an indication for surgery23
- Emergent fasciotomies to release all affected compartments and to prevent further tissue ischemia
Management of Open Fractures
Presentation
Often occurs with higher-energy injuries in areas of the body with relatively less soft tissue coverage or with more extreme angulation of fracture fragments
Exam
Assess for gross contamination, devitalized tissue, lacerations or wounds that do not stop bleeding (more superficial lacerations typically achieve hemostasis more rapidly)
Management
- All open fractures require urgent irrigation and debridement in the operating room
- Surgical debridement 6-8 hours after time of injury is preferred
- Grossly contaminated wounds should be irrigated in ED with low pressure normal saline24 and debrided of contaminants and dead tissue
- Early antibiotic administration is key to reducing infection - Ancef 2 grams every 8 hours for 24-48 hours, add Ceftriaxone when wound is more than 10cm or if the fracture is segmental. However, full extent of wound and classification of grade of open injury by Gustillo-Anderson classification cannot be determined until OR debridement, so if uncertain, add Ceftriaxone empirically
- Standard antibiotic regimens, doses, and durations remain under investigation25
- Penicillin for farm injuries
- Update tetanus prophylaxis
Representative Radiographs:  PDF
PDF





{kind=link}
{kind=link}
{kind=link}