|
|
|
| Click here to visit our web site |
|
INTRODUCTION While numerous studies have described injuries of the cruciate ligaments and menisci in soccer players, little information is available on articular cartilage injuries in these highdemand athletes. (4) This lack of data is surprising since the prevalence of acute and chronic articular cartilage lesions in the cruciate-deficient knee is well documented. 5,6 The lack of available data on cartilage lesions in soccer players is not completely understood, but may be related to the limited treatment options available for these injuries in the past. Levy and coworkers have recently confirmed the increasing frequency of isolated chondral injuries in collegiate, professional and worldclass soccer players. They concluded that the observed increase resulted from both the growing popularity of the sport and the increased awareness of chondral injuries due to emerging new techniques for cartilage repair. (4) In full-thickness injuries to the articular cartilage, disruption of the articular surface occurs without concomitant violation the subchondral bone, which precludes access to the subchondral vasculature. Since no bleeding occurs, the avascular cartilage can only promote repair via a transient increase in mitotic and metabolic activity in the surviving chondrocytes bordering the defect. Due to this limited response, the newly synthesized matrix is nearly always insufficient to fill the defect and restore the articular surface. Laboratory studies have shown that because of the qualitative and quantitative deficiencies in the spontaneous repair tissue, the newly formed matrix deteriorates quickly with loading of the joint surface. (7) Clinically, this leads to progression of the lesions, with pain, swelling, catching of the joint, and a dramatic reduction of the patient’s quality of life and ability to participate in athletic activities. (8) Repair of articular cartilage has been difficult due to the pathophysiology and molecular biology of cartilage tissue, and traditional treatment methods have not produced reliable and lasting results. (9,10) The treatment of articular cartilage lesions in the knee has recently gained considerable interest due to the development of new techniques. The successful repair of articular cartilage lesions of the human knee by autologous chondrocyte transplantation was first reported by Brittberg in 1994. (11) Recent follow-up data demonstrates excellent results with the use of this technique up to eleven years. (12,13) However, an evaluation of autologous chondrocyte transplantation in high-demand athletes, such as soccer players, has not yet been performed. METHODS
Soccer players with acute or chronic articular cartilage lesions were treated with autologous chondrocyte transplantation at Brigham and Women’s Hospital, Boston, MA, Santa Monica Orthopedic Sports Medicine Foundation, Los Angeles, CA and Gothenburg Medical Center, Gothenburg, Sweden. The athletes were examined and completed functional outcome questionnaires preoperatively and at defined postoperative intervals. Data analysis included gender, associated injuries, skill level, previous injuries or trauma, and clinical symptoms. Intraoperative data was collected from operative notes and available intraoperative video recordings and photographs to determine anatomic location, defect size and grade. Articular cartilage lesions were graded using the most widely accepted depth classification system described by Outerbridge (Figure 1). (14)
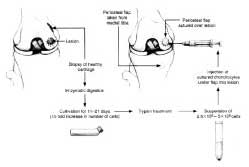
Autologous chondrocytes were harvested from a nonweightbearing area of the knee joint. The cells were then cultured and multiplied in vitro followed by reimplantation after 3-4 weeks. At implantation, the cultured chondrocytes were placed under a periosteal flap covering the articular cartilage defect and sealed with a thin fibrin layer (Figure 2). Local growth factors stimulate the chondrocytes to produce an extracellular cartilage matrix that closely resembles hyaline cartilage. Results of a recent multicenter study demonstrated good to excellent results in up to 92% after 2-11 years following autologous chondrocyte transplantation. 12,13 Rehabilitation was performed according to previously described protocols. (15) Functional outcome was evaluated by use of scientifically established knee rating systems including the Modified Cincinnati Knee Score, Western Ontario McMaster Index WOMAC), and Knee Society Score. Data analysis was performed by standard statistical methods using established commercially available software (SSPS Inc. , Chicago, IL, USA). Differences were considered significant at a probability level of 95% (P<0.05). RESULTS
plateau, trochlear, and patellar lesions also noted. Single lesions predominated (Figure 3). Additional procedures included high tibial osteotomy, ACLreconstruction, meniscal repair, and tibial tubercle osteotomy. Seventy percent of all players rated their results as good or excellent by overall clinical evaluation. The rate of good or excellent results was higher in players with single cartilage lesions or defects located on the medial femoral condyle. Modified Cincinnati scores, Western Ontario MacMaster (WOMAC) Scores, and Knee Society Scores all improved significantly. No association was found between the functional outcome and gender, age, defect location, defect size, defect number, or presence of anterior cruciate ligament deficiency. Failure of the repair occurred in under 15 percent of patients. Graft delamination was noted in one patient. DISCUSSION The soccer population was chosen to test the effect of autologous chondrocyte transplantation since the increased risk for development of knee osteoarthritis in this high-demand athletic population is well documented, particularly at the elite level. (20-23) A recent consensus conference on osteoarthritis at the National Institute of Health (NIH) demonstrated a relative risk of 4.4-5. 3 for knee osteoarthritis in soccer players. (24) This fivefold increased risk for gonarthrosis likely results from the high joint stresses associated with repetitive joint impact and torsional loading from rapid deceleration motions, frequent pivoting, and player contact. Besides chronic cartilage degeneration, acute injuries to the articular cartilage of the knee can have a profound impact on the player’s career, representing the most common cause of permanent disability. (25) Thus, management of chondral lesions in the knee in this high-demand population may play a crucial role in limiting or preventing severe long-term sequelae. (26) Acute or chronic injuries of the anterior cruciate ligament were reported in approximately half of our patients. This is consistent with the previously described high incidence of soccer-related anterior cruciate ligament (ACL) injuries. Anterior cruciate ligament injuries are associated with articular cartilage lesions in 40-70% and these lesions are frequently located on the femoral condyle. (5) Accordingly, the articular cartilage lesions in soccer players in our study presented primarily as isolated lesions of the medial or lateral femoral condyle. In contrast to previous studies,(12) no significant differences were observed between players with isolated or multiple lesions, but this may be related to the relatively low number of athletes with multiple articular cartilage defects in our study population. The percentage of good to excellent results in soccer players falls within the previously reported range of 65-92% good to excellent results for autologous chondrocyte transplantation in the general patient population. (12,13) As observed in previous studies of this technique, isolated lesions of the femoral condyle in soccer players were associated with better outcomes. SUMMARY Kai Mithoefer, MD is a Resident, Harvard Combined Orthopaedic Residency Program. Eric Giza, MD is a Resident, Harvard Combined Orthopaedic Residency Program. Tom Gill, MD is an Attending Physician, Massachusetts General Hospital and an Assistant Professor of Orthopaedic Surgery, Harvard Medical School. Bert R. Bert R. Mandelbaum, MD is an Orthopaedics Surgeon, Santa Monica Orthopaedic and Sports Medicine Group, Santa Monica, California. Tom Minas, MD is Director, Cartilage Repair Center, Brigham and Women’s Hospital and an Associate Professor, Harvard Medical School. Lars Peterson, MD is an Attending Physician, Department of Orthopaedic Surgery Gothenburg Medical Center, Gothenburg, Sweden. Address correspondence to: |
|||||||||
|
Print Manuscript • View References • Download PDF version • Close window |