|
|
|
| Click here to visit our web site |
|
INTRODUCTION
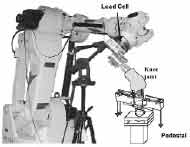
The testing system (Figure 1) consists of a robotic manipulator and a six-degree of freedom load cell. The robotic manipulator (Kawasaki UZ150, Kawasaki Heavy Industry, Japan) is a position-controlling device with a high degree of repeatability for position and orientation. The robotic manipulator can learn the complex motion of a specimen both under unloaded conditions and in response to external loads, and can reproduce these motions in subsequent tests after the specimen has been surgically modified. For example, using the setup shown in Figure 1, the robotic manipulator can define a “passive path” of the knee under zero loading by incrementally determining a flexion path that minimizes forces and moments in the remaining five degrees of freedom. Using the principle of superposition, changes in the kinematic behavior of the knee after surgical modification or in response to simulated muscle loading can then be compared to the original passive path. In this manner, the effects these modifications or loading conditions have on the kinematics and contact forces in the knee can be determined. To date, the robotic testing system has been implemented in testing protocols of the forearm and knee. We would like to present an overview of current research projects in the Bioengineering Research Laboratory using this robotic testing technology. ROLE OF THE INTEROSSEOUS LIGAMENT IN FOREARM
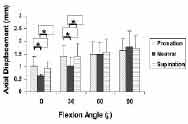
LOAD TRANSMISSION In order to design a suitable reconstruction, it is important to understand the biomechanical role of the IOL in the intact forearm. Previous studies have used load cells implanted directly in the radius and ulna to quantify the force transferred across the IOL under compressive loads applied to the forearm. (3,7,10) However, implantation of the load cell requires soft-tissue dissection and disruption of the integrity of the radius and ulna, potentially changing the structural properties of the forearm. These studies have not investigated to what extent disruption of the bony architecture affects the experimental determination of IOL force. Furthermore, most of these studies have only examined the function of the IOL at one elbow flexion angle. (3,7) By using the robotic testing apparatus, we have been able to noninvasively test a series of human cadaveric forearms at varying elbow flexion and forearm rotation positions, to determine in situ forces in the IOL in response to a 100N compressive load along the long axis of the radius. Testing was performed with the bones and soft tissues of the forearm intact, and transsection of the IOL was performed via an incision along the subcutaneous border of the ulna, with minimal disruption of soft tissues and closure of the wound in layers prior to testing. Our experiments demonstrated that displacement of the radius in response to axial compressive load varied with elbow flexion and forearm rotation (Figure 2). With the forearm in neutral, axial loading resulted in maximal displacement at 90° of elbow flexion. Similar patterns of increasing displacement with increasing elbow flexion were observed with the forearm in supination and pronation.
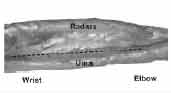
In neutral forearm rotation, in situ IOL force was minimal at full extension and increased to a maximum of 19 N at 90° of elbow flexion. In contrast, loading of the forearms in pronation and supination resulted in maximal IOL force at 30° of elbow flexion; minimal force was again noted at full extension for both forearm supination and pronation. Over all flexion angles, the highest force was observed when the forearm was supinated; the average forces transferred from the radius to the ulna were 36%, 21%, and 15% of the applied forearm load in supination, pronation, and neutral, respectively. These findings indicate that the IOL plays a significant biomechanical role in the transmission of force from the radius to the ulna in the forearm. The amount of force that the IOL transfers depends on whether the forearm is in pronation, supination, or neutral, and also varies with flexion of the elbow. At all flexion angles, the force that the IOL transfers from the radius to the ulna was greater in supination than in pronation or neutral rotation. These findings are similar to those reported by others. Morrey et al. reported that, under simulated muscle loads, force transferred via the radiocapitellar joint was greater in pronation than in supination, implying that more force was carried in the IOL in supination. (7) Using load cells directly implanted in the radius and ulna, Birkbeck et al. reported that the IOL transferred 17%, 6%, and 6% of applied axial load when the forearm was supinated, neutral, and pronated, respectively. (1) Advantages to our experimental technique include the measurement of forces and displacements with no disruption of the bones and minimal disruption of the soft tissues surrounding the forearm. Previous studies have reported force in portions of the IOL (e.g. the central band). (5,6,12) Our experiment quantified the force in the entire IOL. Schneiderman et al. (10) observed that anatomically, the IOL has a number of thickened bands throughout its length (Figure 3), and suggested that strain in different portions of the IOL is not uniform and varies with different positions of the forearm. Published studies have differed in reported values for IOL central band dimensions,(3,12) which implies that either there is significant variation in the morphology of the central band, or that proper identification of this structure is difficult. Therefore, measurement of force transferred by the IOL across its entire length may be a more accurate measure of its contribution to forearm biomechanics.
Clinically, most radial head fractures occur with the forearm pronated. We found that, with the elbow in full extension, the IOL carried only 8% of the applied axial load in pronation, compared with 31% in supination. Under axial loading, less force in the IOL with the forearm in pronation implies greater force transmitted across the radiocapitellar joint. Therefore, in a fall on an outstretched hand with the forearm pronated and elbow extended, the IOL does not function as effectively to bear axial load, resulting in greater load transmission through the radial head and increasing the likelihood of radial head fracture. Similarly, our results suggest that the forearm should be immobilized in supination after isolated radial head fracture, to minimize forces transmitted across the radial head. Finally, the significant role of the IOL in axial force transmission in the forearm suggests that repair or reconstruction of the IOL may be indicated in Essex-Lopresti lesions in order to improve clinical outcomes. In summary, a minimally invasive technique was utilized to quantify the forces transferred by the IOL from 0° to 90° of flexion with the forearm in pronation, neutral, and supination. Our results demonstrate that the IOL plays an important biomechanical role in bearing axial load in the forearm. The IOL transfers load from the radius to ulna across the full range of forearm flexion with maximum load transferred in supination at all flexion angles. These findings may help explain the pathogenesis of radial head fractures, and have implications on the treatment of forearm injuries. Further work will focus on the incorporation of simulated muscle loads across the forearm and their effect on load bearing in the IOL. ACKNOWLEDGEMENTS
Conrad Wang, MD is a Resident, Harvard Combined Orthopaedic Residency Program. Guoan Li, PhD is an Assistant Professor, Orthopaedic Surgery/Bioengineering Harvard Medical School. Harry E. Rubash, MD is Chief, Department of Orthopaedic Surgery, Massachusetts General Hospital and Edith M. Ashley, Professor of Orthopaedic Surgery, Harvard Medical School. Address correspondence to: |
|
Print Manuscript • View References • Download PDF version • Close window |