INTRODUCTION
Isolated arthritis of one compartment of the
knee poses a difficult clinical challenge. Unicompartmental knee arthroplasty
(UKA) has been advocated as a potential treatment for this condition.
Although early reports of UKA were unfavorable(1,2),
several authors have recently reported excellent clinical results at long
term follow-up, by using more stringent selection criteria, improved surgical
technique, and more precise instrumentation. (3-5)
HISTORY
The first unicompartmental arthroplasties were
implanted in the early 1950’s. The original procedures involved a
hemiarthroplasty resurfacing of the tibia. (6,7)
The major source of failure in these implants was articular cartilage
loss on the femoral side. Marmor, based on experience with these tibial
plateau prostheses, addressed the femoral side with a metal component
and thus inserted the first cemented unicompartmental knee replacement
in the United States. (8)
The all polyethylene Marmor tibial component was modeled on the tibial
plateau prostheses. In 1978, Goodfellow and O’Connor designed the
Oxford implant, a meniscal bearing prosthesis, with a spherical femoral
component, a flat metallic tibial component, and a fully congruent polyethylene
liner to allow rotation and translation of the liner between the femur
and tibia. (9,10) During the
early years of their development, many of these prostheses were used on
both the medial and lateral side of the same knee. (8,11-13)
These bicompartmental, modular arthroplasties proved to be more technically
difficult and less reliable than standard total knee arthroplasty and
fell out of favor by the early 1980’s. Recently, there has been a
resurgence of interest in UKA in the United States, based on good long-term
results and the potential advantages of this operation over alternatives
such as high tibial osteotomy and total knee arthroplasty.
INDICATIONS
Kozinn and Scott put forth the most widely
accepted indications for UKA in 1989. (14)
Their criteria included age greater than 60 years, weight less than 180
lbs. , low activity level, and minimal pain at rest. They advocated a
minimal arc of motion of 90°, with no greater than a 5° flexion
contracture, and correctable angular deformity of not greater than 10°
varus or 15° valgus. The anterior cruciate ligament is felt by many
authors to play a critical role in the success of UKA. This is particularly
true in certain designs such as the Oxford meniscal bearing implant, as
soft tissue laxity can lead to displacement of the central polyethylene
bearing. Patient weight is also an important factor in success of UKA.
Heck et al. analyzed risk factors for failure after UKA. (15)
In a series of 294 knees, the average weight of patients requiring revision
was 90. 4 kg (199.3 lbs. ) compared to 67 kg (147.7 lbs. ) in non-revised
cases. Many authors continue to perform UKA in spite of the presence of
patellofemoral chondromalacia. (3,14,16)
However, in our experience, patients who have complaints of predominantly
anterior knee pain at rest, anterior pain with squatting and stair climbing,
or who have a positive patellar apprehension test may be better treated
with tricompartmental knee arthroplasty. Patients with chondrocalcinosis
or inflammatory disease such as rheumatoid arthritis are best treated
with total knee arthroplasty due to the risk of progression and ongoing
synovitis.
UNICOMPARTMENTAL KNEE ARTHROPLASTY COMPARED
TO HIGH TIBIAL OSTEOTOMY
High tibial osteotomy (HTO) has traditionally
been indicated in young, active patients with unicompartmental arthritis
of the medial compartment. In comparison to UKA, results after HTO have
been inferior. Several studies have shown statistically better long-term
outcomes after unicompartmental arthroplasty compared with high tibial
osteotomy in similar patient populations. A direct comparison of HTO to
UKA was performed in Bristol, UK(17,18)
and reported by Broughton et al. at 5-10 years and by Weale and Newman
at 12-17 years. They compared a group of 49 knees with UKA (average age
at latest follow-up = 80) to a group of 42 knees treated with HTO (average
age at latest follow-up = 74). Preoperative characteristics were similar
between the groups. At 12 to 17 year follow-up, pain was absent or mild
in 80% of the UKA group and only 43% of the HTO group. The HTO patients
had a higher reoperation rate than the UKA group (35% vs. 12%). There
was a higher complication rate in the HTO group with more wound problems,
neurovascular complications, and higher rate of deep vein thrombosis (DVT).
(18)
MINIMALLY INVASIVE SURGERY
 |
 |
|
| Three
inch long skin incision is made starting from the superior pole of
the patella and extending distally to the tibial tubercle (1 cm medial
to the medial pole of the patella). |
A medial arthrotomy is made in line with skin incision. |
|
 |
 |
|
| Femoral
sizing guide attached and the chamfer cuts performed along with drilling
of the lug holes for the femoral component. |
The
external tibial alignment guide-taking approximately 2mm of bone from
medial tibial plateau. |
|
 |
 |
|
| The
transverse tibial cut is performed with a reciprocating saw. |
Final implants E F |
|
| Minimally
Invasive Unicompartmental Knee Arthroplasty |
|
The term minimally invasive surgery has been
used to describe operations with small skin incisions and less muscle
dissection. Repicci and Eberle showed that it was possible to resurface
one compartment of the knee using a three inch incision extending from
the proximal medial tip of the patella to a point 1 inch below the tibial
articular surface. (19) A
one-inch proximal transverse capsular incision was also made, extending
from the medial edge of the patella in combination with a 1. 5 inch incision
of the medial capsule from the tibial plateau . Using this technique, 80% of their
patients were able to have an outpatient procedure. These authors advocated
preoperative arthroscopic examination to evaluate for involvement of other
compartments. Using this technique, the estimated average cost of UKA
was $7000 compared with $16,000 for UKA with a standard knee incision
and arthrotomy with patellar eversion. (19)
Price et al. prospectively compared the technique of UKA through a short
medial incision without patellar dislocation to UKA through a standard
open incision with patellar eversion, and to TKA through a standard incision.
(20) Recovery in the minimally
invasive group was twice as rapid as the open UKA group and three times
as rapid as the TKA group. Robertsson et al. performed a cost analysis
of UKA to TKA by comparing matched patients from the Swedish Knee Registry.
(21) They determined that
for UKA, mean hospital stay was shorter with lower cost, and the cost
of the UKA implants was approximately one-half of the cost of TKA implants.
FUTURE DIRECTIONS
 |
|
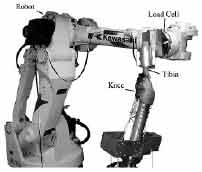
Robotic Testing System: Six degree-of-freedom (DOF) universal load
cell (JR3 Model 160M50S, JR3 Inc. , Woodland, CA) attached to the
end effector of a 6DOF robot arm (Kawasaki UZ150, Kawasaki Heavy Industry,
Japan). The system has a load capacity of 1470 N. Courtesy Dr. Guoan
Li |
Few studies in the literature have investigated
the biomechanical behavior of unicompartmental knee replacement. Range
of motion, walking, and stair climbing have been studied in clinical reports
of UKA, but the kinetics and kinematics of UKA have not been well quantified
in vitro. The effect of implant alignment and orientation likely plays
an important role in cartilage contact pressures and motion in the uninvolved
compartments. Additionally, although the importance of an intact ACL in
knee joint function after UKA has been reported in clinical studies, this
has not been studied directly in the laboratory. Such quantitative data
would be a significant help to surgeons in improving indications, materials,
designs and ultimately the clinical results of UKA. In future studies
carried out by this lab, a robotic testing system will be used to quantify
the effect of UKA on knee kinematics and contact forces in various compartments
of the knee .
The data from these studies may help to optimize the biomechanics of UKA
and provide guidance for future high flexion UKA designs.
SUMMARY
Unicompartmental knee arthroplasty is an effective
and reliable surgical treatment for localized knee arthrosis. Using strict
patient selection criteria, this procedure has demonstrated excellent
long-term results, comparable to those of total knee arthroplasty. (3,5)
In the current health-care market, unicompartmental knee arthroplasty
may have multiple advantages over total knee arthroplasty based on lower
implant cost(21), shorter
hospital stay(20), more rapid
recovery(20,22), decreased
transfusion requirement(19,23),
and improved patient satisfaction(24).
is an Arthroplasty Fellow, Massachusetts General Hospital.
is
a graduate student at MIT.
is Chief, Arthroplasty Service, Massachusetts General Hospital.
is Chief, Department of Orthopaedic Surgery, Massachusetts General Hospital
and Edith M. Ashley, Professor of Orthopaedic Surgery, Harvard Medical
School.
Address correspondence to:
Andrew Freiberg, MD
Department of Orthopaedic Surgery
Massachusetts General Hospital
Wang ACC, Suite 537
15 Parkman Street Boston,
MA 02114
|
