
Research
28th Annual Meeting of The Orthopaedic Trauma Association
September 6-8, 2012, Chicago, IL
Alignment in Nonperatively Treated Distal Radius Fractures: Are Our Current Predictors Predictive?
Joey Lamartina, M.D., Charlton Stucken, M.D., Andrew Jawa, M.D., Paul Tornetta III, M.D.
Boston University Medical Center, Boston, MA, USA
Background/Purpose
Multiple methods have been described to predict loss of reduction in distal radius fractures treated nonoperatively. We sought to independently validate the McQueen equation and LaFontaine’s criteria in a large series of distal radius fractures treated nonoperatively. Additionally, we wished to evaluate postreduction volar cortical alignment (volar hook) and a specific definition for dorsal comminution on the final reduction of these patients. We hypothesized that restoring the volar cortical integrity would aid in maintenance of the volar tilt by a standard three-point molded cast.
Methods
We prospectively screened 546 consecutive distal radius fractures using the McQueen equation and LaFontaine’s criteria for instability. We excluded patients with <10° of dorsal tilt upon presentation, leaving 275 fractures of which 168 were treated nonoperatively and form the basis of this study. Patients were managed with short arm casts and seen every other week in the clinic by an attending orthopaedic trauma surgeon. Patients were recasted if there was thought to be a shift in the fracture position or if the cast became loose. We measured the following parameters on the initial reduction and final radiographs: dorsal tilt, radial height, radial inclination, ulnar variance, and the presence of carpal malalignment. We defined dorsal comminution as having a loss of the dorsal cortex of ≥5mm on the postreduction lateral radiograph. We defined “volar hook” as having collinear alignment of the cortical edges of the fracture at the volar surface. We performed univariate analysis to determine how predictive the McQueen percentage and the number of Lafontaine’s criteria present were on each radiographic parameter. Additional univariate analyses were done on the radiographic components of each score, volar hook, sex, and age. Based on the univariate analysis of the various predictors, a multivariate analysis was done including age, dorsal comminution (DC), volar hook (VH), and intra-articular fracture (IAF) against all radiographic outcome parameters and any change in those parameters during healing.
Results
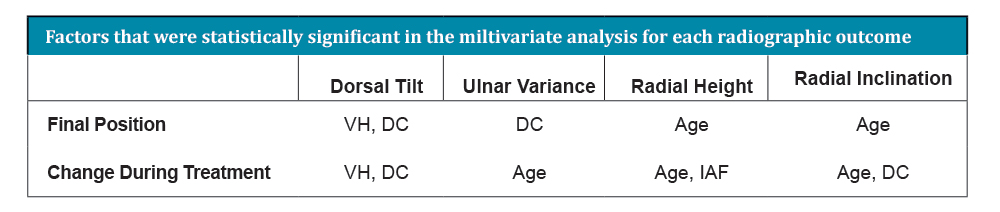
In the univariate analysis, the McQueen percentage and the total number of LaFontaine’s criteria present predicted the change in radial height and inclination. The change in dorsal tilt was predicted by VH and DC. The change in ulnar variance was predicted by DC and IAF. The change in radial height was predicted by IAF and age and the change in radial inclination was predicted only by age. Final dorsal tilt was predicted by VH, DC, and sex. Carpal malalignment at healing was predicted by VH and age. The table details the results of the multivariate analysis.
Discussion
We attempted to validate the McQueen percentage and Lafontaine’s criteria on the final radiographic position and the change in position over time in 168 consecutive patients with displaced distal radius fractures treated nonoperatively. Additionally, using a multivariate technique, we found that VH and DC were strong predictors of final dorsal tilt and the change in angulation during healing. Age was the most important factor in predicting ulnar variance, radial height, and inclination as well as the change in these parameters during treatment. Most important, VH (P = 0.001) and age (P = 0.03) were both predictive of carpal malalignment.
Conclusion
We were able to validate the McQueen equation and LaFontaine’s criteria on radial height and inclination. However, neither method was predictive of final dorsal tilt or carpal malalignment. Hooking the volar cortex (restoring the volar cortical integrity) was the strongest predictor of final volar tilt, the change in volar tilt, and carpal malalignment at union. These data suggest that restoration of volar cortical alignment is an important predictor of success in nonoperative treatment of distal radius fractures.

- In This Issue
- Senior Thesis Day
- Abstracts
- Research Reviews
- Citations