
Original Submissions
Current Issue: Volume 15 |  PDF
PDF
Approach to Management of the Patient with the Multiligament-Injured Knee
Kaitlin M. Carroll B.S., Gregory Cvetanovich M.D., Benton E. Heyworth M.D., Sam Van de Velde M.D., Thomas J. Gill IV M.D.
Sports Medicine Service, Department of Orthopaedic Surgery, Massachusetts General Hospital, Harvard Medical School, Boston, MA 02114
PDF
Background: Multiligament knee injuries are typically the result of severe trauma, and can result in loss of limb or limb function. At the present time, there is controversy regarding initial treatment and optimal surgical management.
Questions/Purposes: The objectives of this study were (1) tTo offer an algorithm for management of the patient with a multiligamentous injury to the knee .(2) to describe the clinical and functional outcomes of a consecutive series of patients with multiligament knee injuries managed with this approach by a single surgeon (3) to present a novel surgical technique for the treatment of multiligamentous knee injuries.
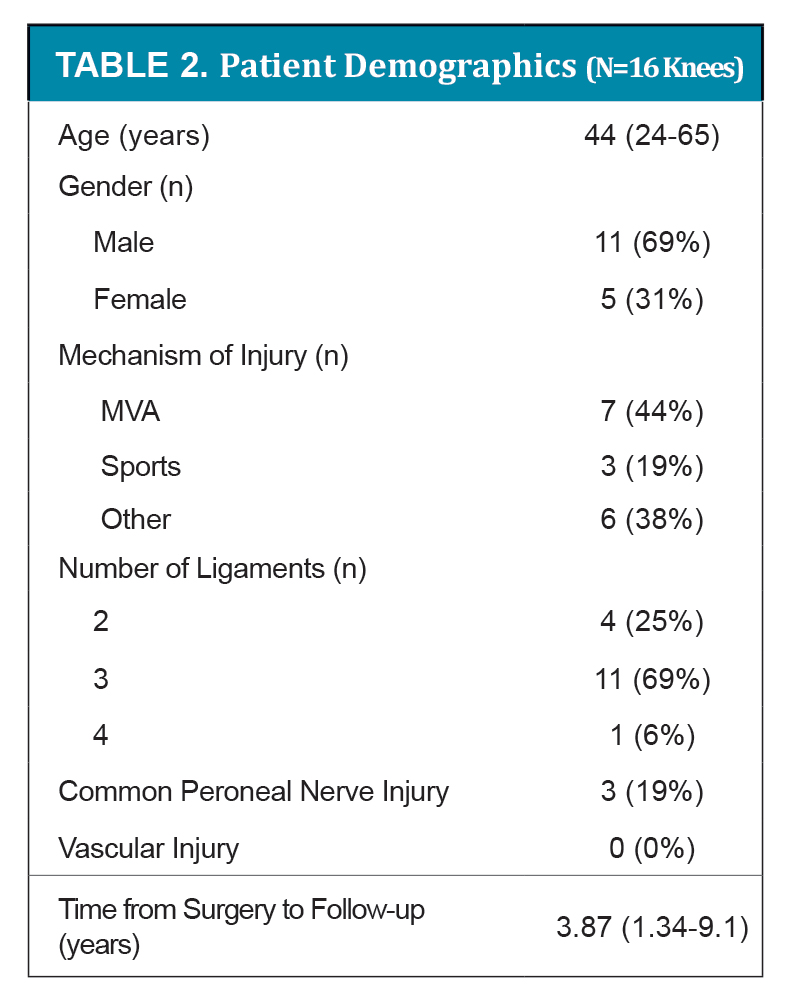
Patients & Methods: We present data on sixteen consecutive knees in 16 patients, 11 male and 5 female, mean age 44 (range 24-65) years with a diagnosis of a multiligament knee injury (defined as a disruption of two or more ligaments that include the PCL). All patients underwent standard preoperative evaluation and were treated according to our algorithm for surgical reconstruction of multiligament-injured knees. Mean follow-up since surgery was 3.87 (range 2-9) years. Outcome measures were determination of range of motion, testing with KT-2000 arthrometer, and Tegner and Lysholm scores.
Results: Common mechanisms of injury were MVA in 7 patients (44%) and sports in 3 patients (19%). Of the four major knee ligaments, 4 patients (25%) had two injured ligaments, 11 patients (69%) had three injured ligaments, and 1 patient (6%) had four injured ligaments. There was an associated common peroneal nerve injury in 3 patients (19%) and there were no patients with associated vascular injuries. Six patients (38%) underwent staged reconstruction, with the remainder of patients undergoing single-stage reconstruction. Following surgery, mean range of motion (ROM) in flexion was 111 (range 95-138) degrees, and mean ROM in extension was -2 (range -12-0) degrees. Mean Tegner score before injury was 6 (range 0-9) and mean Tegner activity level after reconstruction was 4 (range 1-7). Mean post-operative Lysholm score was 78 (range 30-118). Mean KT-2000 anterior manual maximum difference was 2.5 (0.3-6.7) millimeters and mean posterior difference was 2.2 (0.0-3.3) millimeters. Following surgery, one patient (6%) had symptomatic recurrent instability that required a revision.
Conclusions:Our current algorithm used to treat this series of multiligament knee injuries demonstrated satisfactory clinical and functional outcomes, with few complications. An algorithmic approach to treatment as presented by the authors can minimize adverse sequellae associated with surgical treatment of multiligament knee injuries.
Keywords: medial collateral ligament (MCL), medial knee injury, knee ligament injury, multiligament injury
Level of Evidence: Level IV, case series.
Background
Although they account for less than 0.02% of all orthopaedic injuries, multiligament knee injuries may lead to neurovascular compromise that can threaten the affected limb.8,15 Multiligament knee injuries are defined as disruption of at least 2 of the 4 major knee ligaments, and typically occur as a result of acute, traumatic knee dislocation.1,5,21 In addition to ligament damage, the energy required for traumatic knee dislocation frequently causes other associated injuries such as fracture and neurovascular damage.5,8,21 Even if neurovascular compromise is avoided, the morbidity resulting from multiligament knee injuries is substantial and includes pain, instability, and stiffness of the affected joint.5
The optimal treatment of multiligament knee injuries is a complex problem. This is currently an area of controversy in the field due to a paucity of high-level evidence to guide management. Historically, treatment involved closed reduction and casting or cast-bracing immobilization.9 With recent advances in operative technique, multiligament knee injuries are now typically managed surgically.8,9 Cohort studies to date have suggested that surgical treatment yields superior outcomes compared to nonoperative management, as measured by International Knee Documentation Committee (IKDC) scores and higher rates of return to work and sports.2,14,16,23 In addition, cohort studies have suggested that for most injury patterns, early surgery (<3 weeks from the injury to the operation) yields improved outcomes compared to delayed surgery, as measured by Lysholm scores and IKDC scores.4,6,10,20,22 Finally, studies addressing repair versus reconstruction of damaged structures indicate that reconstruction of the posterolateral corner (PLC) is associated with lower revision rates than repair of the PLC, and that reconstruction of the cruciate ligaments yielded superior functional and clinical outcome compared to repair of these structures.7,11,18
To our knowledge, there have been no randomized-controlled trials addressing the impact of different management options on outcomes of patients with multiligament knee injuries. Multiligament knee injuries do not lend themselves well to randomized controlled trials for various reasons, including the heterogeneity of multiligament knee injuries (both pattern of ligament injury and associated ipsilateral and contralateral leg injuries), the high rates of associated trauma, and the relatively low incidence of these injuries. In light of these challenges of studying the multiligament-injured knee, it is imperative that authors continue to report well-designed case series and descriptions of algorithmic approaches to management of these injuries.
Through this case series, we intend to (1) describe our approach to the patient with a knee dislocation, and 2) to report on the outcomes of these patients following our reconstruction algorithm of multiligament-injured knees.
Patients & Methods
Patients
Between 2003 and 2008, 16 consecutive patients with 16 multiligament-injured knees (defined as disruption of 2 or more ligaments that include the PCL) and no other major trauma underwent surgical reconstruction performed by the senior author. With appropriate Institutional Review Board approval, the prospectively collected data were retrospectively reviewed, and all patients were invited for follow-up examination to assess clinical and functional outcome. The follow-up examinations were performed by a single clinician. Outcome measures collected were the Lysholm score, Tegner activity scale, KT-2000 arthrometric testing (MedMetric, San Diego, CA), and clinical examination of range of motion (ROM). Multiligament knee injuries were classified according to the classification system of Schenck.17
Clinical Assessment
All patients underwent standard preoperative evaluation, including neurovascular evaluation, determination of instability pattern, soft tissue assessment, and diagnostic imaging with MRI.
Physical Examination
Anterior cruciate ligament injuries were diagnosed with a positive Lachman test, anterior drawer test, and pivot shift test. PCL injuries were diagnosed with a positive posterior drawer test at 90 degrees and positive posterior sag. Grade III injuries were indicated for surgery. MCL injuries that required surgical repair were grade III injuries with no end point to valgus stress. PLC injuries that required surgical repair or reconstruction were unstable to varus stress and had a positive dial test at 30 and 90 degrees of knee flexion.
Vascular Assessment
Vascular assessment was performed on all patients. Formal arteriography was reserved for patients with diminished or abnormal palpable pulses, ankle-brachial index less than 0.8, or a knee dislocation resulting from high energy trauma.
Neurologic Assessment
Baseline EMG studies were obtained at approximately 2 weeks after injury if a patient was diagnosed with a peroneal nerve injury. If a neurotmesis was present, acute nerve exploration and cable grafting was indicated. If an incomplete injury was diagnosed, repeat EMG studies were obtained 6 months to check on the recovery status.
Imaging
All patients were assessed with plain radiographs to rule out fracture and confirm reduction of the joint. MRI scans were performed on all patients to not only to confirm the ligamentous injuries diagnosed by physical examination, but to identify their exact site of injury. In particular, collateral ligaments were examined to see if the tear was mid substance vs. an avulsion injury, and to identify any associated intra-articular damage.
Surgical Technique
Surgery was typically deferred until range of motion was restored to at least 120 degrees, and for at least 3 weeks to give the joint capsule time to heal in order to avoid fluid extravasations from arthroscopy.
The patient is placed in the supine position with a leg post with a well padded thigh tourniquet placed as proximally as possible. No intra-operative fluoroscopy is used. To begin, a diagnostic arthroscopy is performed using standard inferolateral and inferomedial portals. Any associated articular cartilage or meniscal injuries are addressed.
PCL Reconstruction
PCL reconstruction is indicated for all multiligament injured patients with grade III PCL injuries. Reconstruction is performed using a 10 mm Achilles tendon allograft. The PCL remnants are debrided and an accessory posteromedial portal is established. A 70° arthroscope is used during debridement of the posterior aspect of the proximal tibia under direct visualization. A PCL tibial guide (Arthrex, Naples, Fl) is inserted at a 70° angle and a 10 mm tibial tunnel is drilled under direct visualization. The PCL femoral guide (Arthrex, Naples, Fl) is then placed approximately 6 mm posterior to the articular surface in the 11:30 position for left knees (12:30 position for right knees), a short longitudinal incision made over the anteromedial aspect of the distal femur, and an 10 mm femoral tunnel is drilled outside-in. The Achilles tendon allograft is passed in antegrade fashion. A 25 mm interference screw is used to secure the femoral tunnel. Screw diameter is determined based on graft-tunnel fit. Cycling of the knee should reveal less than 1 mm of graft motion in all cases. The tibial tunnel is left unsecured.
ACL Reconstruction
The tibial guide is inserted through the inferomedial portal using a 55 degree angle. The entrance point on the tibia should be at least 2cm above the PCL tibial tunnel, and approximately half way between the tibial tubercle and the tibial attachment of the MCL. The tip of the guide is placed in the central aspect of the ACL tibial footprint, at the level of the anterior horn of the lateral meniscus. A 10mm tunnel is then drilled for the patellar tendon allograft. A reverse chamfer drill is used to smooth the posterior aspect of the tibial tunnel at the entrance into the joint. A 6mm femoral guide is then placed through the tibial tunnel, and aimed at 2 or 10 o’clock position on the intercondylar wall. The femoral tunnel is then reamed with a 10mm drill through the tibial tunnel with the knee flexed to 90°. The graft is passed in retrograde fashion. A femoral interference screw is used to secure the femoral attachment of the graft. The tibial attachment is left unsecured.
MCL Repair/Posteromedial Corner Reconstruction
The MCL is examined under anesthesia pre-operatively. MCL repair is performed in the acute setting when the ligament is avulsed from either its femoral or tibial attachment site. Typically, suture anchors are used to re-attach the attachment site. For acute mid substance tears a ligament repair with capsular imbrication is performed.
For more chronic injuries with a mid-substance tear and residual valgus instability after cruciate fixation, a MCL reconstruction is performed with posteromedial corner reconstruction.
The isometric attachments of the femoral and tibial attachment sites are determined by inserting a Kirchener wire into the medial femoral epicondyle and at a point in the medial tibia 6-8 cm distal to the medial joint line. It should be remembered that the MCL has an attachment site slightly posterior to the mid-coronal plane of the tibia. A heavy suture is then looped around the wires and the knee put through a range of motion from 0-90 degrees. If there is undue (>2-3mm) excursion of the suture with flexion and extension, the attachment sites should be relocated and repeat testing performed.
Once the attachment sites have been determined, we prefer a split Achilles tendon allograft for surgical reconstruction. The calcaneal bone block is prepared to fit loosely through a 10mm spacer. It is inserted into a 10mm x 30mm drill hole in the medial femoral epicondyle, and secured with a composite interference screw. One limb of the Achilles tendon is tubularized, and “docked” into a drill hole made in the tibia of 7mm, which is secured with both an interference screw and by tying the sutures over the lateral aspect of the tibia. The knee should be placed in 30 degrees of flexion when reconstructing the MCL.The function of the posterior oblique ligament can then be re-approximated by suturing the posterior limb of the graft into the posteromedial capsule. This posteromedial aspect of the reconstruction contributes substantially to the resultant valgus and posteromedial rotational stability.
LCL Repair/Posterolateral Corner Reconstruction
For acute injuries, LCL repair is performed when the distal attachment site is avulsed from the proximal fibula, often with the distal tendon of the biceps femoris. Three drill holes are placed through the proximal fibula, and the tendons of the LCL and biceps femoris are whipstitched. The sutures are passed through the bone tunnels in the proximal fibula, and tied distally. The tear in the posterolateral capsule is repaired. However, even in the acute setting, residual varus instability can persist. In these cases, a PCL reconstruction/augmentation is performed.
Multiple different types of posterolateral reconstructions have been described, and there are certainly many approaches that can be used successfully. In the subacute setting, we perform a fibular-based reconstruction. A soft tissue allograft such as a posterior tibial tendon or semitendinosis is whipstiched. A 6mm drill hole is made from posterior to anterior in the fibular head leaving at least a 1 cm proximal bone bridge proximally. The lateral femoral attachment site is identified, a kirchener wire placed, and a heavy suture passed around the wire and through the fibular head in a triangular shape. The knee is put through a range of motion from 0-90 degrees to insure that there is not undue (>2-3mm) excursion of the suture. The soft tissue graft is passed through the fibular head, and “docked” into an 8mm x 40mm femoral tunnel. The knee is flexed to 30 degrees, with a slight valgus and internal rotation force. The graft is secured in the bone tunnel with a composite 8mm x 30mm interference screw. The suture ends are passed through the femur, and tied over the medial femoral cortex to re-enforce the stability of the graft.
In the more chronic setting with severe posterolateral rotation stability (as evidenced by a dial test of 30 degrees or more), a formal popliteus reconstruction using a popliteal “bypass” graft is performed. We prefer to use a split Achilles tendon graft, where the bone block is fixed in the femoral tunnel with an average graft length of 20 cm. The anterior limb of the graft is then passed from posterior to anterior through the fibular head, secured with an interference screw, and sewed back upon itself as it exits anteriorly. The posterior limb is passed from posterior to anterior through the proximal aspect of the lateral tibial metaphysis, exiting at the level of Gerdy’s tubercle and fixed with an interference screw in order to recreate stability from the popliteus tendon. Once the collateral ligaments are secured, the knee is flexed to 90 degrees with an anterior drawer applied. A 9 x 30 mm Milagro ( Depuy Mitek, Raynham, MA) interference screw is inserted until it reaches the posterior tibial cortex, typically 60-65mm posteriorly in the tunnel to fix the PCL in the tibial tunnel. This technique will shorten the effective length of the graft and increase its stiffness, .3 , thereby improving the posterior stability of the joint.3 Fixation is augmented with a 9 x 30 mm interference screw more anteriorly.
Next, the knee is brought into full extension. The ACL tibial tunnel is secured with the graft under full tension in extension with an interference screw.
Rehabilitation
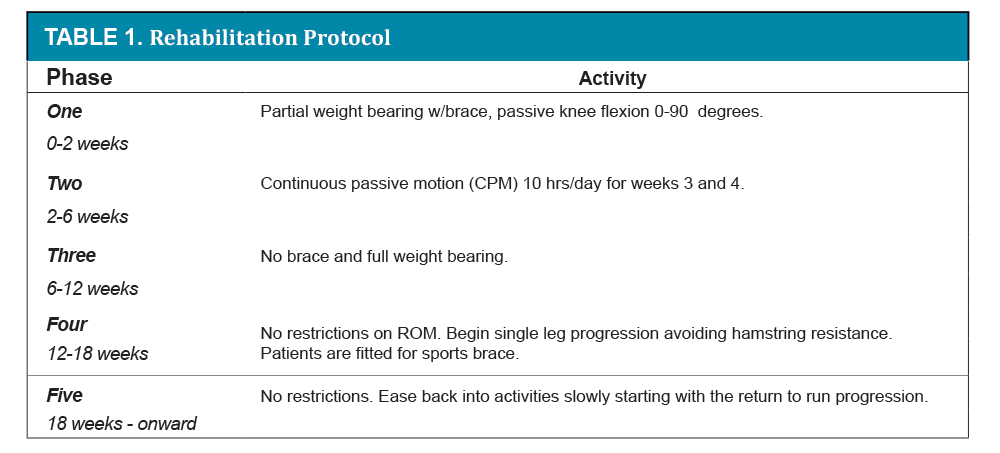
All patients underwent our standard postoperative rehabilitation for these injuries (Table 1). Our standard postoperative rehabilitation protocol consists of five phases to protect the reconstructed ligament and ease patients back to activity with an early emphasis on range of motion. Phase one is from 0-2 weeks, and involves partial weight bearing with a hinged brace locked at zero degrees with passive knee flexion 0-90 degrees. Phase two is from 2-6 weeks with partial weight bearing and continued use of the brace for ambulating 0-90 degrees. At this phase in the rehabilitation protocol, patients use a continuous passive motion (CPM) machine for 10 hours a day for weeks three and four to gain their full range of motion. Phase three is 6 to 12 weeks with no brace and full weight bearing. At this point patients should have full range of motion. From 0-12 weeks patients should focus on closed-chain strengthening and proprioception exercises. Phase four is 12-18 weeks post-operatively with no restrictions on ROM. Patients should continue closed chain strengthening and start single leg progression avoiding hamstring resistance. At this point, patients are fitted for a sports brace. Phase 5 is from 18 weeks onward with no restrictions and patients should ease back into their activities slowly starting with the return to run progression. Patients can return to most strenuous job-related activities in 4-6 months, light sports in 6 months, and heavy sports in 8 months. Following surgical dislocation of a dislocated knee, return to running is permitted at 4 months with a custom fit brace, with return to contact sports at 8 months. It typically takes at least one full year for a patient to optimize their outcome following reconstruction with regard to muscle strength, joint motion, speed and agility.
Data Analysis
Data are presented with mean values and ranges for the relevant variables. The paired Wilcoxon test was used to compare the preoperative and postoperative scores and to compare the clinical scores between the involved and noninvolved knee. Spearman correlations were used to evaluate the influence of the clinical results on functional outcome scores. P values were considered significant when P<0.05.
Results
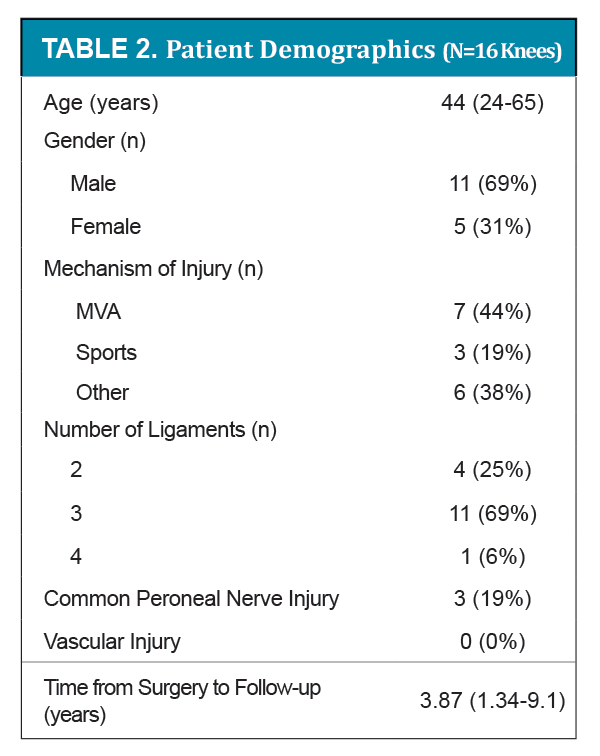
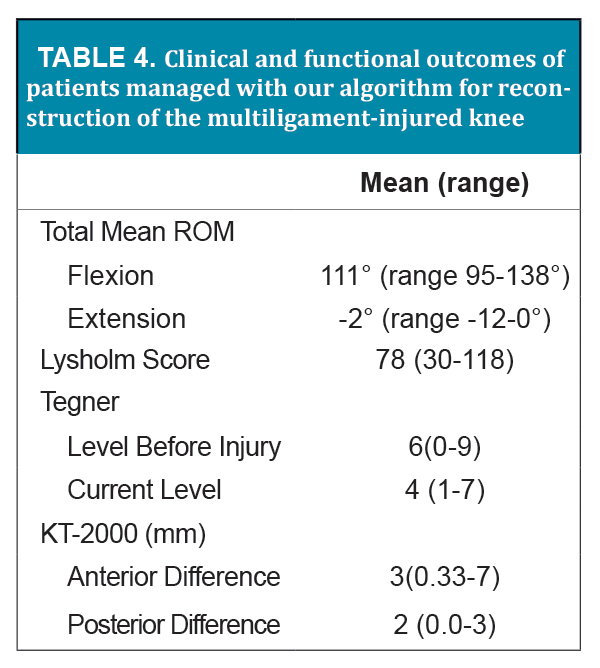
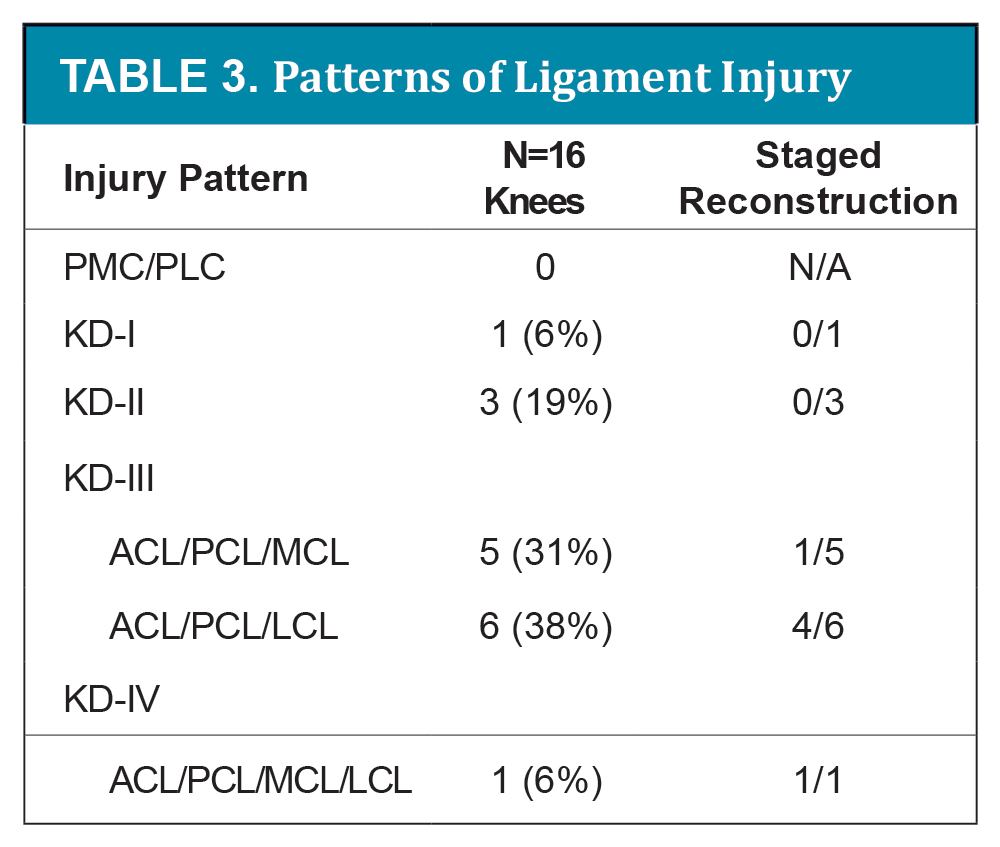
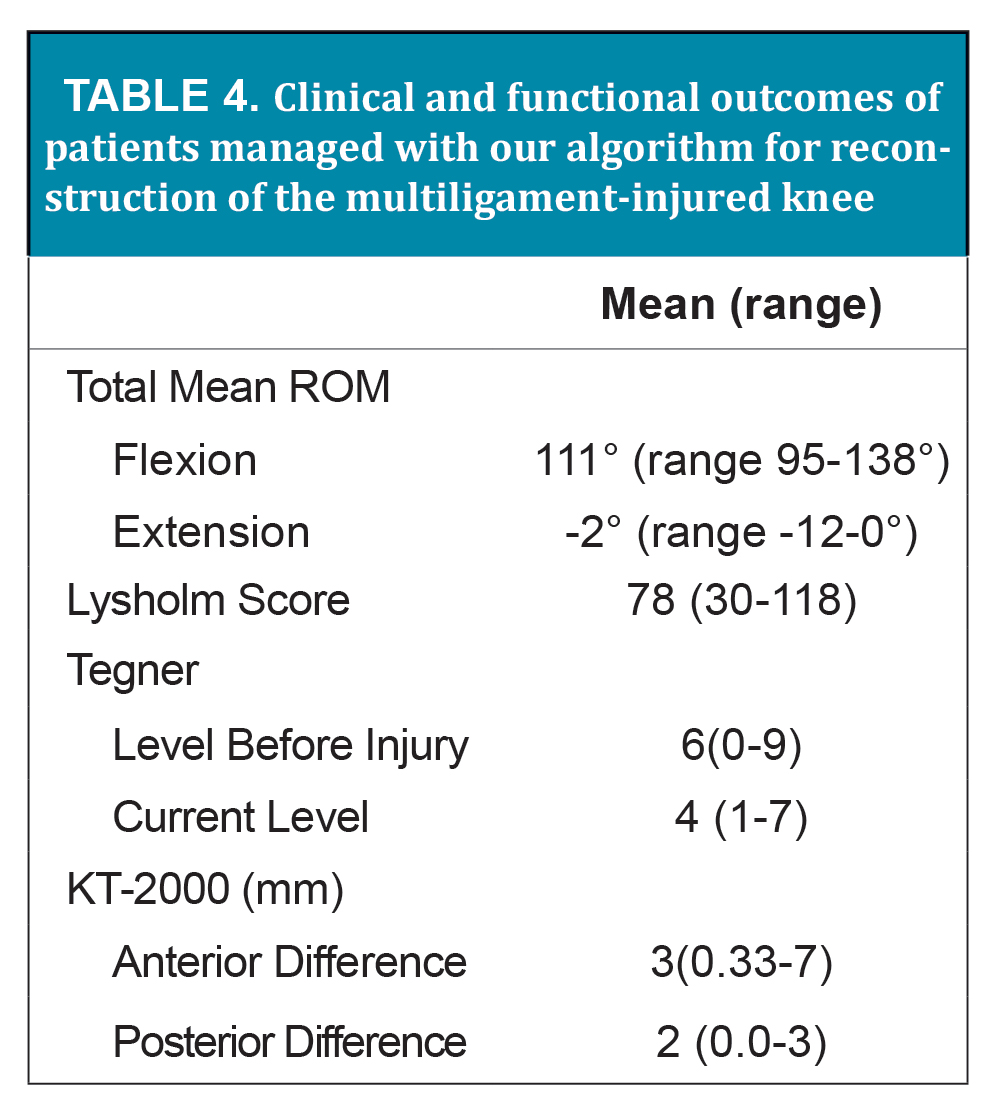
Table 3 classifies the injury pattern according to the Schneck classification of multiligament-injured knees and indicates the usage of staged reconstruction for each injury pattern for our series of cases.17 One injury (6%) was KD-1, 3 injuries (19%) were KD-II, 5 injuries (31%) were KD-III involving the MCL/PMC, 6 injuries (38%) were KD-III involving the LCL/PLC, and 1 injury (6%) was KD-IV. Six patients (38%) underwent staged reconstruction, 1 patient with ACL/PCL/MCL injuries, 4 patients with ACL/PCL/LCL injuries, and 1 patient with ACL/PCL/LCL/MCL injuries. All other patients underwent single-stage reconstruction. On average, patients underwent follow-up for clinical and functional outcome 3.9 years after surgery (range 1.3 to 9.1 years). Table 4 describes the clinical and functional outcomes of patients managed with our algorithm for reconstruction of the multiligament-injured knee. Mean range of motion (ROM) in flexion was 111 degrees (range 95-138 degrees). Mean ROM in extension was -2 degrees (range -12-0 degrees). Mean Lysholm score was 77.7 (range 30-118). Mean Tegner level before injury was 6 (range 0-9), and mean current level at the time of follow-up was 4 (range 1-7).
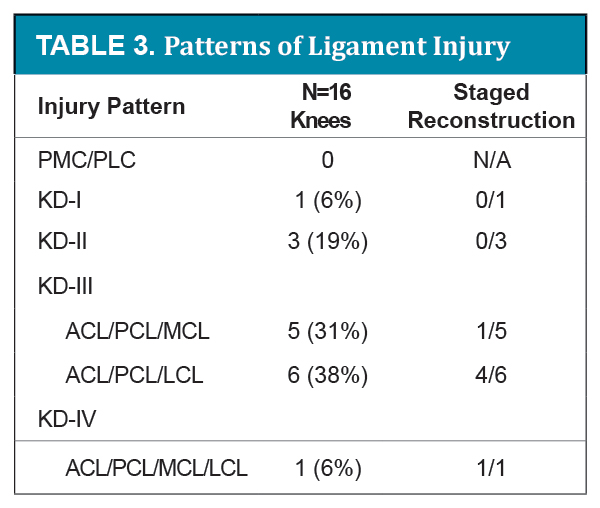 KD = knee dislocations, MCL = medial collateral ligament (including posteromedial corner), LCL = lateral collateral ligament (including posterolateral corner), ACL = anterior cruciate ligament, PCL = posterior cruciate ligament.
KD = knee dislocations, MCL = medial collateral ligament (including posteromedial corner), LCL = lateral collateral ligament (including posterolateral corner), ACL = anterior cruciate ligament, PCL = posterior cruciate ligament.Classification methology described by: Schenck RJ. Classification of knee dislocations. Oper Tech Sports Med. 2003;11:193-198
-View Large-
{kind=link}
{kind=link}
{kind=link}
{kind=link}
A ligamentous knee examination using a KT-2000 arthrometer revealed a mean anterior difference of 3 (range 0.3-7) millimeters and a mean posterior difference of 2.0mm (range 0.0-3.3).
Complications included the need for a revision due to recurrent instability. This occurred in 1 (6%) patient . No arthrofibrosis, intra-articular infection, deep venous thrombosis, or superficial wound infections were noted.
Discussion
In this study, no patient sustained a vascular injury. However, when a patient presents with a multiligament injured knee, there are several key issues to keep in mind. First, anytime there are 3 or more ligaments involved, the patient should be assumed to have sustained a knee dislocation. As such, it is imperative to rule out an associated vascular injury to the popliteal vessels. In particular, an intimal tear in the popliteal artery must be ruled out. Consultation from the institutional vascular surgery service should be routinely performed, and the use of a diagnostic algorithm and various modalities are often institution-specific. The senior author frequently requests an angiogram, especially in the setting of high energy, posteriorly directed trauma. Magnetic resonance angiography (MRA) shows promise as an alternative means of investigating the vascular status.19 Ankle-brachial indices can also be helpful, especially in the subacute setting (> 24 hours after injury), and should be performed in conjunction with serial vascular examinations, including Doppler, by the primary orthopaedic surgery team. If less than 0.9, they have been shown to have a positive predictive value of 100%.12 Meticulous documentation and communication are critical in this phase to avoid limb-threatening sequellae of these injuries.
In addition to ruling out a vascular injury, careful assessment of the peroneal and tibial nerves should be performed, especially in the setting of posterolateral corner injuries. Nerve injury has been reported in approximately 25% of knee dislocations,13 and such injuries are typically the result of traction injuries. In this study, 3/16 patients (19%) sustained common peroneal nerve injury and no patients injured the tibial nerve. The peroneal nerve is injured far more commonly than the tibial nerve, and one-third of all injuries will recover spontaneously.13
If neurovascular injury has been ruled out, most patients will benefit from surgical ligamentous reconstruction, especially if they wish to return to athletics or physically demanding professions. The primary considerations relating to surgical management are (1) timing of surgical intervention, (2) repair vs. reconstruction of torn cruciate and/or collateral ligaments, (3) type of graft to be used if reconstruction is chosen, (4) non-operative versus operative treatment of MCL injuries, (5) rehabilitation philosophy, and (6) application of specific return to play/work criteria.
Although there are different ways to approach knee dislocations, the results of this study demonstrate a high percentage of excellent outcomes using the following treatment philosophy.
Acute vs. Delayed Surgery
With regard to timing of surgical intervention, we reserve acute surgery for open dislocations, vascular injury, or uncontrolled instability. As none of these indications for acute surgery occurred in this study population, no patients in our study underwent acute surgery. For patients with vascular injuries, we prefer to repair any collateral ligament injuries when possible at the time of the vascular repair, and delay addressing the cruciate ligaments until the revascularization has been in place for at least 8 weeks. This is especially the case for lateral sided injuries, where the LCL and biceps femoris typically avulse from the fibular head and retract proximally. If gross stability remains a concern after revascularization, an external fixator can be placed. Return to surgery should then be delayed until the fixator is removed at 4-6 weeks and range of motion restored to at least 120 degrees, with use of a hinged-knee brace to maintain stability in this period.
In the absence of vascular injury or open dislocations, we will consider surgery in the sub-acute period if there is an avulsion of the LCL and biceps femoris complex from the fibular head. In this situation, we have found that direct repair of the LCL and biceps femoris complex is best performed within the first six weeks, and preferably the first 3-4 weeks. The popliteus is sometimes avulsed from the femur as well, and can be repaired at the same time. In this study, /6 patients with ACL/PCL/LCL injury underwent early repair of the lateral side, followed by staged cruciate reconstruction. The other two patients with ACL/PCL/LCL injury had a single-stage repair due to the need to get back to their sport in the shortest period of time possible.
For most medial-sided dislocations, there is little necessity for acute intervention. In the author’s experience, medial-sided dislocations have a higher risk of stiffness after surgery. We typically wait 6-8 weeks with early range of motion exercises in a hinged brace in order to restore motion and to facilitate non-operative MCL healing, especially in the case of mid-substance collateral ligament injury. If the MCL is completely avulsed from the femur, or there is significant retraction of the tibial attachments of the superficial MCL with grade III valgus laxity, then we will often perform surgical reconstruction of the ACL and PCL at 4-6 weeks once motion has been restored and the capsule healed, and perform a direct repair of the MCL at the same time. Waiting much longer makes this repair more difficult, as the MCL attachments can become encased in scar. For our case series, 4/5 patients with ACL/PCL/MCL injury were treated with a single-stage surgical intervention involving reconstruction of the ACL and PCL between 6-8 weeks after injury. 1/5 patients was treated more acutely, with surgery 10 days after injury, involving MCL repair and PCL reconstruction, followed by staged ACL reconstruction. This was due to the presence of a tibial avulsion of the MCL, which typically has persistent valgus laxity following non-operative treatment.
Similarly, there is little need for an acute repair in “simple” (i.e. no neurovascular injury) lateral-sided dislocations if the LCL is torn mid-substance. In this situation, primary repair is not possible. Posterolateral corner reconstruction must be performed, and we believe that this is best performed on a sub acute basis (4-6 weeks), once range of motion has been restored and associated trauma addressed.
Repair vs. Reconstruction of Ligaments
The question of repair versus reconstruction of ligaments is best addressed by separating the categories into cruciate injuries vs. collateral ligament injuries, as well as by the location of the tears (i.e. mid-substance vs. avulsion). In general, we believe that there is no role for direct ACL repair and little role for PCL repair unless there is a bony avulsion from its posterior tibial attachment site. In our series, all cruciate ligaments underwent allograft reconstruction. We prefer allograft because it minimizes iatrogenic trauma to an already traumatized knee. ACL repair has been shown to have very poor results. In the senior author’s experience, PCL repair also has an unacceptably high failure rate, with more residual laxity than a well-done reconstruction.
With regard to the collateral ligaments, MRI is a very important aspect of the pre-operative surgical planning process. Mid-substance tears of the LCL and popliteus should be reconstructed. Fibular avulsions of the LCL/biceps femoris complex should be repaired. However, it is not uncommon for some residual post-operative varus laxity following direct repair. In order to minimize this persistent laxity, direct repair of the posterolateral joint capsule and popliteus (if possible) should be performed concomitantly. In our series, 3/6 patients with LCL/PLC injury underwent repair of these structures, whereas the other 3/6 patients underwent PLC/LCL reconstruction. Using our approach, the repair alone was performed in 3 patients because there was good posterolateral stability following the initial repair of the LCL and posterolateral capsule. Reconstruction was performed in 3 patients in whom persistent laxity persisted despite repair.
In our opinion, there is seldom an indication for primary reconstruction of the MCL in the acute or subacute setting. In our series, 2/5 patients with MCL injury underwent repair. MCL avulsions were directly repaired using suture anchors. Mid-substance tears are treated initially in a hinged-knee brace with early motion, which resulted in 3 MCL injuries able to be treated non-operatively prior to surgical reconstruction of the cruciate ligaments. Capsular imbrication can be considered if there is too much residual valgus laxity following reconstruction and fixation of the cruciate ligaments. If a knee dislocation is being reconstructed after a more chronic presentation (e.g. greater than 6 months), ACL/PCL and concomitant MCL reconstructed may be necessary. There were no such cases in our series.
Rehabilitation
It is commonly stated that the biggest problem with surgical treatment of a knee dislocation is stiffness, rather than instability. While true in some cases, the etiology of the multiligament injury, its initial treatment, timing of the surgery, whether the medial or lateral ligaments are involved, surgical technique, and post-operative rehabilitation play a more decisive role in whether this adage holds true. Knee dislocations that result from high-velocity trauma or a crush injury are more likely to result in stiffness due to the associated soft tissue trauma, especially if definitive surgical interventions of the ligaments are performed on an acute basis. Patients who are not treated with pre-operative rehabilitation to restore motion pre-operatively are also more likely to result in stiffness, just as occurs when an isolated ACL reconstruction is performed before motion is restored.
Medial dislocations tend to be stiffer. As a result, we prefer to begin early range of motion post-operatively. Because the lateral ligamentous complex is primarily extra-articular, stiffness is much less of an issue, while persistent laxity is more of a risk. Therefore, we tend to keep ACL/PCL/PLC procedures immobilized for 2-3 weeks while partial weight bearing to encourage PCL and PLC stability, and then unlock the brace for motion while ambulating. Continuous passive motion machines are very helpful to restore motion, minimize swelling, and decrease pain in some cases. Using this approach, there were no cases of arthrofibrosis in this series.
Conclusion
The current series presented here demonstrates favorable outcomes with use of the treatment algorithm presented. While addressing all of the associated injuries at the same surgical procedure is possible, especially for ACL/PCL/MCL injuries or in patients for whom return to play/work is a major concern, there should be little hesitation on the part of the surgeon to plan for a staged procedure if 1) there is an ACL/PCL/PCL injury pattern, 2) the patient is at high risk for stiffness, 3) there is a concern about the length of tourniquet time, or 4) a re-vascularization is needed. The post-operative rehabilitation for an ACL reconstruction is very different from that of a PCL reconstruction. The ACL is best when moved early, the PCL often benefits from initial immobilization. The ACL protocol emphasizes hamstring strength and function, while the PCL rehabilitation emphasizes the quadriceps. Therefore, especially for younger athletes, we do not hesitate to perform a primary PCL/PLC reconstruction, followed by 8 weeks of rehabilitation to restore motion and gain muscle control, followed by ACL reconstruction at the second stage. Any adhesions formed from the initial trauma and PCL reconstruction can also be resected at this second stage, thereby minimizing the risk of arthrofibrosis and patellofemoral pain.
The strength of this study is that a single surgeon performed all the cases with a standardized approach and standardized rehabilitation protocol. This study is limited by a retrospective review of prospectively collected data on a small series of cases.
While individualization of management decisions based on each patient’s clinical presentation, as well as their baseline and future goals for function is warranted, adoption of an algorithmic approach can minimize the wide range of adverse sequellae associated with multiligament knee injuries. We advocate its use to give patients the best chance for knee stability and optimization of lower extremity function and return to sport and work.
Ethical Board Review Statement
All human studies have been approved by the appropriate ethics committee and therefore have been performed in accordance with the ethical standards in the 1964 Declaration of Helsinki. All persons gave their informed consent before their inclusion in the study. All studies were carried out in accordance with relevant regulations of the US Health Insurance Portability and Accountability Act (HIPAA).
References
