
Original Submissions
Current Issue: Volume 15 |  PDF
PDF
Load-sharing Construct Allowing for Immediate Weightbearing and Mobilization in a 18 year old with Bilateral Calcaneus Fractures: A Case Report
John Y. Kwon, M.D., Mostafa M. Abousayed, M.D., Eric C. Fu, M.D., and Gleeson Rebello, M.B.B.S.
Department of Orthopaedic Surgery, Massachusetts General Hospital, Harvard Medical School, Boston, MA 02114
PDF
Background
Patient AR is a healthy 18-year-old male who sustained bilateral closed calcaneus fractures after an axial loading injury while skiing. The patient presented to the emergency department of Massachusetts General Hospital complaining of bilateral foot pain and swelling.
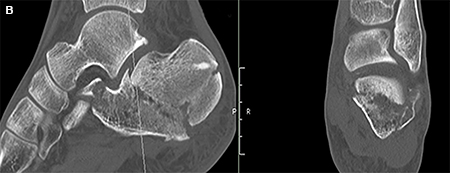
Physical examination revealed bilateral foot tenderness and edema in an otherwise alert and oriented patient. His skin was intact and his lower extremity compartments were soft and compressible with intact neurovascular examinations. Plain x-rays of both feet were obtained and revealed bilateral calcaneus fractures (Figures 1A, 1B). CT scan of the right foot revealed a Sanders type I calcaneus fracture with minimal involvement of the posterior facet and normal Bohler’s angle. CT scan of the left foot revealed a tongue type fracture with flattening of Bohler’s angle and increased relative displacement. (Figures 2A, 2B).
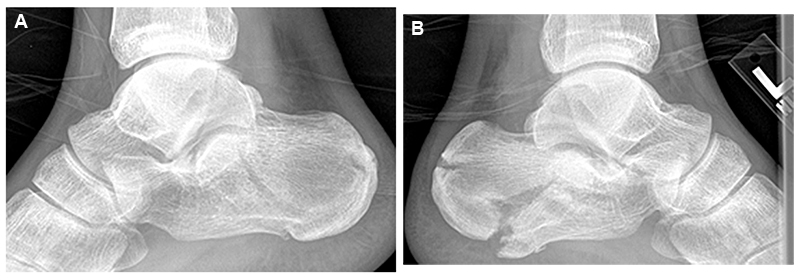
(A) Right Sanders I calcaneus fracture (B) Left tongue type calcaneus fracture demonstrating displacement and flattening of Bohler’s angle
All Rights Reserved. Permission For Use Required.
-View Large-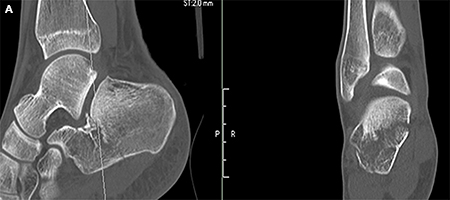
{kind=link}
{kind=link}
{kind=link}
CT Scans (A) Right calcaneus (B) Left Calcaneus
After proper consultation, a decision was made to treat both sides surgically via percutaneous approaches to accelerate the rehabilitation course of the patient and allow early weight-bearing.
Surgical Intervention
The patient was taken 1 week post-injury to the operating theatre. Under general anesthesia with bilateral popliteal blocks, the patient was first placed in the right lateral decubitus position.
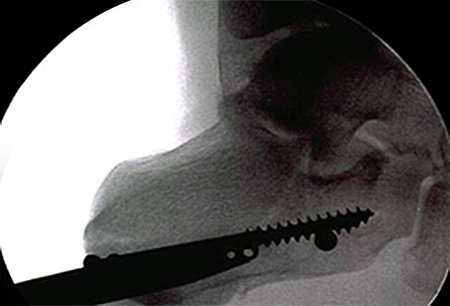
Intraoperative image demonstrating rafting screws placed using “perfect circle” technique of the drill sleeve for proper screw positioning
All Rights Reserved. Permission For Use Required.
-View Large-{kind=link}

Preoperative CT scan showing malreduced syndesmosis
All Rights Reserved. Permission For Use Required.
At the two-week post-operative visit (3 weeks post-injury) his surgical incisions were found to be well healed. The patient transitioned to a short air cast boot on the left side and instructed to continue non-weight-bearing and began self-directed range-of-motion exercises. On the right-side, he was placed in a Darco heel wedge shoe and allowed to fully weight-bear. This specific type of shoe off-loads pressure on the heel by approximately 25% and transfers weight bearing loads to the mid and forefoot (Figure 4).
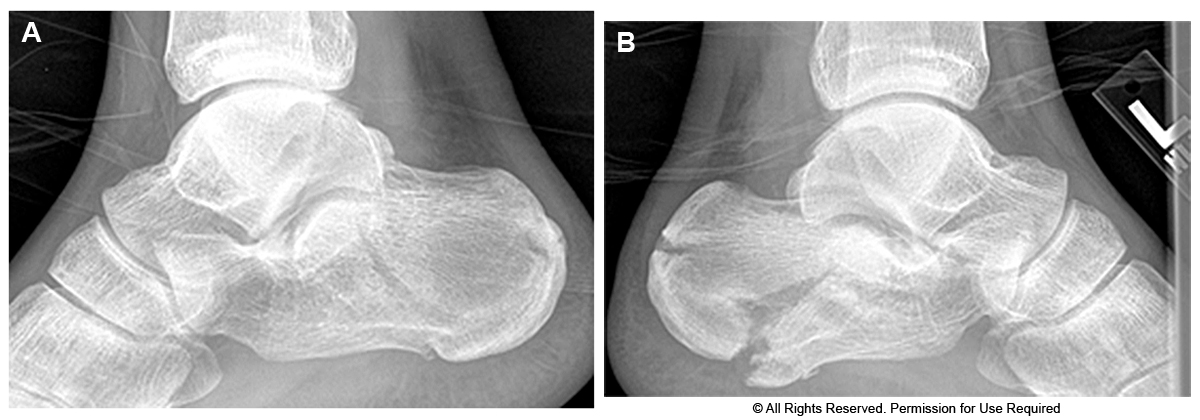
At the patient’s five-week post-operative visit, plain x-rays of both sides showed maintained reduction and position of the screws. Patient activity was progressed to touch-down-weight-bearing in his boot on the left. On the right-side he was transferred to a regular post-operative shoe with continued full-weight-bearing. He was fully weight-bearing bilaterally in a regular shoe without assistive devices at 2 months postoperatively and went on to successful healing. (Figures 5A, 5B, 5C, 5D).
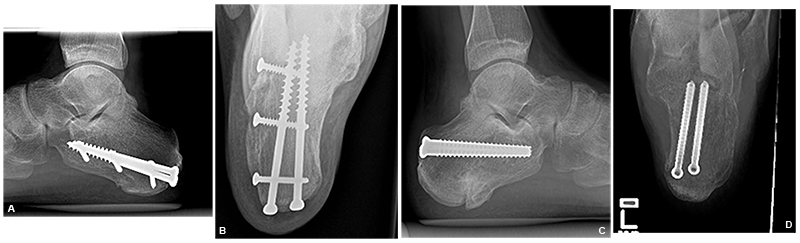
(A) Right calcaneus lateral view (B) Right calcaneus Harris heel view (C) Left calcaneus lateral view (D) Left calcaneus Harris heel view
All Rights Reserved. Permission For Use Required.
-View Large-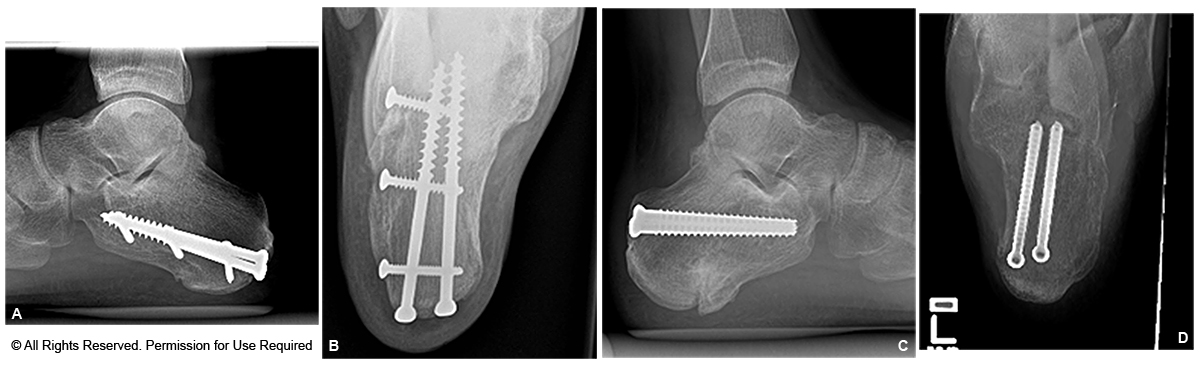{kind=link}
Outcome scores were obtained at approximately 3 months postoperatively. His American Orthopaedic Foot and Ankle Society (AOFAS) hindfoot score was 94/100. His Short-Form (SF)-36 physical function score was 70 and norm-based physical function score 44.6 (compared to average physical function score for males 18-24 years old being 54.26).
Discussion
We present the case of an 18-year-old male who sustained bilateral calcaneus fractures treated with a percutaneously placed load-sharing construct to stabilize a non-displaced calcaneus fracture. The clinical benefit of this intervention was to allow for immediate weight-bearing and early mobilization in the setting of bilateral injuries.
Most authors have recommended nonoperative management of Sanders type I fractures given the minimal displacement and relative preservation of the posterior facet of the calcaneus.1, 2, 3 Crosby and Fitzgibbons evaluated the outcomes of non-operative treatment of calcaneus fractures and concluded that all patients with non- or minimally-displaced type I fracture had better results in comparison to displaced type II and III fractures.4 Given the relatively high rate of wound healing complications using traditional operative exposures, Sanders type I fractures have been historically treated nonoperatively. Successful conservative treatment of calcaneal fractures traditionally consists of non-weight bearing in a cast or boot for a period of 2 - 3 months. The main drawback with prolonged immobilization and nonweightbearing is increased collagen breakdown, disuse osteopenia, muscle atrophy, joint stiffness and general deconditioning. Fiorre, et al. found a positive correlation between the amount of bone resorption and the length of immobilization and suggested that uncoupling between bone formation and resorption with consequent disuse atrophy develops during this period.5
In the presented case study, the major clinical benefit of operative intervention was an earlier transition to full weight-bearing for an otherwise healthy young patient with bilateral calcaneus fractures. Faster return to weight-bearing theoretically decreases muscle atrophy and joint stiffness, and allows for earlier return to activities of daily living and work. Percutaneous reduction and fixation mitigates the major surgical risk of post-operative wound breakdown and infection.
Examining the internal architecture of the calcaneus, five distinct trabecular patterns can be identified. The primary compressive group is directed in a dorso-plantar direction from the posterior facet and fans towards the posterior inferior tuber. The secondary compressive group is centered at the Angle of Gissane and directed towards the anterior inferior calcaneus and calcaneal-cuboid articulation. The primary tensile group is directed antero-posteriorly towards the posterior surface while the secondary group lies more anteriorly. The fifth trabecular pattern extends from the tuberosity towards the insertion site of the tendo-achilles.6, 7, 8 They are arranged in a unique fashion with a small triangular area relatively void of dense trabeculae lying at the mid portion of the calcaneus which represents the weakest part of the calcaneus. This neutral triangle, which is devoid of dense trabecular bone and directly plantar to the inferior anatomic apex of the talus, is the site of the primary fracture line in calcaneus fractures. Mahato, et al.9 demonstrated that 70 % of the body weight forces are distributed across the superior articular surface of the calcaneus with the remaining 30% through the sustentaculum.9 This fact, along with the understanding of the calcaneal trabecular patterns and cancellous bone density, helps explains the formation of the primary fracture line.
Understanding the load distribution on the calcaneus and pathomechanics of fracture line development and displacement, we aimed to devise a load sharing construct to stabilize this patient’s non-displaced right calcaneus fracture to allow for immediate weightbearing in the setting of bilateral injuries. Two large solid 6.5 mm screws, with increased resistance to bending forces compared to cannulated screws, were placed traversing the calcaneus as internal struts to reinforce the stability of the calcaneal long axis. The calcaneus, similar to the metatarsals and unlike other load-sharing bones, is loaded perpendicular to its long axis. Therefore to prevent cantilever bending of the cancellous screws, three 3.5 mm bicortical screws were placed in a lateral to medial direction functioning as struts to support the overlying axial screws from failing, thus creating a supported beam construct.
No previous study has compared operative to conservative treatment for non-displaced calcaneal fractures nor specifically examined the morbidity of prolonged non-weight-bearing and immobilization in this setting. This case report illustrates the utility of a load-sharing construct to allow early weight bearing and faster return to pre-injury level of activities. Due to his bilateral calcaneus fractures, this patient would have traditionally undergone 2-3 months of non-weight-bearing and reliance on a wheelchair during this time. Our load-sharing construct for the right calcaneus fracture allowed for full weightbearing in an offloading shoe at 3 weeks post-injury which accelerated his recovery and allowed for crutch mobilization. Furthermore this allowed for rapid mobilization with outcome scores obtained at 3 months postoperatively demonstrating excellent AOFAS hindfoot scores and SF-36 physical function scores approaching norms for his demographic peer group.
References
