
Original Submissions
Current Issue: Volume 15 |  PDF
PDF
Measuring Bohler’s Angle with Oblique Lateral Radiographs: Implications for Management of Calcaneal Fractures
R. James Touissaint, M.D., Leah Gitajn, M.D., and John Kwon, M.D.
Department of Orthopaedic Surgery, Massachusetts General Hospital, Harvard Medical School, Boston, MA 02114
PDF
Background: In the setting of calcaneus fractures, attempts at perfect lateral hindfoot images usually result in oblique x-rays. The purpose of this study is two-fold: (1) to assess whether orthopaedic surgeons can accurately measure Bohler’s angles on oblique lateral radiographs; and (2) to determine how Bohler’s angle (BA) is influenced by the obliquity of lateral radiographs.
Methods: Observed Bohler’s Angle Measurement- A cadaver specimen was imaged using a C-arm to obtain a perfect lateral and oblique laterals up to 25 degrees in the anterior, posterior, cephalad and caudad directions. Orthopaedic attendings and residents were asked to measure the observed BA’s. True Bohler’s Angle Measurement - Metallic markers were placed in the anatomic landmarks needed to calculate the BA. The same series of oblique images were obtained. The true BA was then measured on each image.
Results: Observed Bohler’s Angle - The observed BA’s were significantly different from the control value for all images except for the posterior oblique image at 20 degrees. True Bohler’s Angle - The greatest difference from the perfect lateral BA was found in the cephalad-oblique radiographs, whereas the BA remained relatively constant with posteriorly directed oblique radiographs.
Conclusions: Orthopaedic surgeons’ ability to accurately measure BA significantly decreases with increasing obliquity of lateral radiographs. The true BA varies most with increasing obliquity in the cephalad direction, but less so with posteriorly directed radiographs. Understanding these subtle changes should enable surgeons to more carefully interpret data obtained from oblique lateral radiographs when deciding upon treatment based on Bohler’s angles.
Keywords: bohler’s angle, calcaneus fracture, radiographs
Level of Evidence: Level V
Background
The calcaneus is the most commonly fractured tarsal bone, and it accounts for 1% to 2 % of all fractures. The majority of calcaneus fractures are caused by a fall from height or a motor vehicle accident, and typically result in depression of the posterior facet.6 First described in 1931, the “tuber-joint angle” or Bohler’s angle (BA) is used to determine the amount of posterior facet displacement and loss of calcaneal inclination. The Bohler’s angle is obtained on a lateral foot radiograph. It is the angle formed by the intersection of a line joining the highest point of the anterior calcaneal process and the highest point of the posterior process, with a line drawn projecting from the superior posterior calcaneal tuberosity.2 It is widely accepted that in the uninjured adult population, a normal Bohler’s angle is between 25 and 40 degrees.2, 1 However, numerous papers suggest that there is variation among populations, with a range of values between 14 degrees in Malawians and up to 50 degrees in Ugandan subjects.15, 8, 14, 7, 13
Bohler’s angle has been shown to have prognostic value in determining morbidity and outcomes following calcaneus fractures.4 This radiographic parameter is often used to guide treatment, and the need for obtaining further imaging such as computed tomography (CT) scans. Unfortunately, lateral radiographs obtained in the trauma setting are often oblique due to difficulties in positioning the traumatized extremity, or due to limited positioning secondary to splint materials. These detail of these radiographs may influence the accuracy of the measured Bohler’s angle, as skewed views can lead to more bony overlap that blurs the proper anatomic landmarks. Inaccurate assessment of Bohler’s angles may lead to under- or overtreatment of patients with intra-articular calcaneus fractures.
The purpose of this study is two-fold: (1) to assess whether orthopaedic surgeons can accurately measure Bohler’s angles on oblique lateral radiographs; and (2) to determine how Bohler’s angle, as measured using consistent anatomic landmarks, is influenced by the obliquity of the lateral radiograph. We hypothesize that orthopaedic surgeons will inaccurately measure Bohler’s angle on oblique lateral x-rays. We also hypothesize that the true Bohler’s angle will vary based on the magnitude of the obliquity of the lateral image.
Materials and Methods
Observed Bohler’s Angles
A fresh-frozen cadaver specimen was imaged using a large C-arm with laser positioner (General Electric, Fairfield, CT) to obtain multiple fluoroscopic images. First, a perfect lateral image of the hindfoot was obtained. A perfect lateral requires that the medial and lateral articular surfaces of the talar dome be superimposed, that the tibiotalar joint remains open with a symmetrical joint space, and that the distal fibula continues to be superimposed by the posterior half of the distal tibia.12 Next, a series of oblique images was taken with the beam directed anteriorly, posteriorly, cephalad and caudad. These images were taken in 5-degree increments from 0 to 25 degrees in each direction, with the C-arm’s laser positioner utilized to maintain a constant reference point (Figures 1, 2). Forty-one orthopaedic surgeons, consisting of five foot and ankle and trauma specialists and 36 orthopaedic residents (Post-Graduate Years 1 through 5), were then asked to measure Bohler’s angles on all images. All participants received written instruction on how to measure Bohler’s angle as originally described by Bohler in 1931.2 All images were presented in random order via a random order generator spreadsheet function (Excel, Microsoft Corp, Redmond, WA). All study participants used the angle-measuring tool found within the Picture Archiving and Communication System (PACS).
True Bohler’s Angles
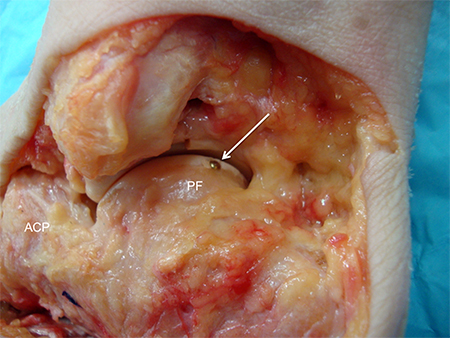
Dissected cadaver specimen with visible metallic marker placed in the superior most portion of the posterior calcaneal facet. ACP = anterior calcaneal process. PF = posterior facet. Arrow is pointing at metallic marker.
All Rights Reserved. Permission For Use Required.
-View Large-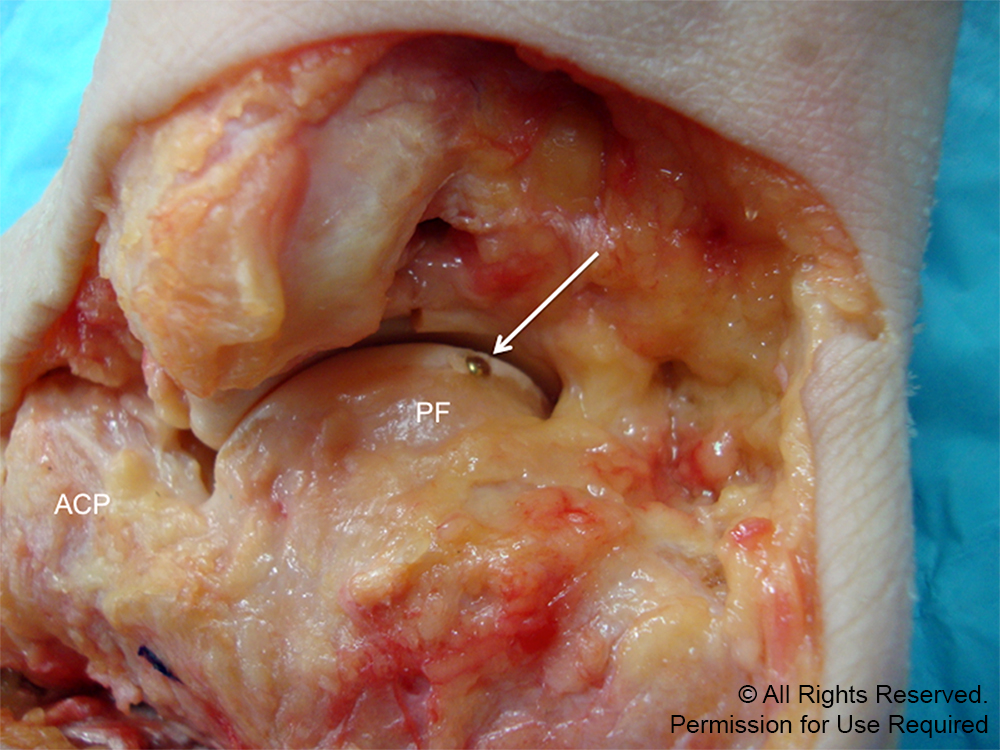{kind=link}
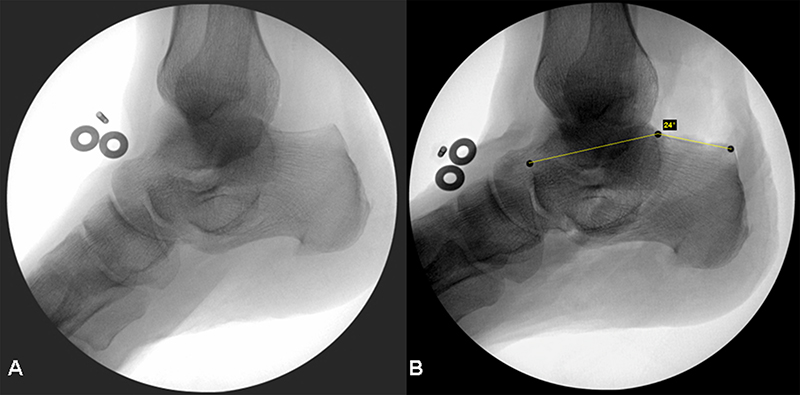
Representative oblique lateral images of the hindfoot with x-ray beam directed 25-degrees cephalad. (A) Without metallic markers. (B) With metallic markers.
All Rights Reserved. Permission For Use Required.
-View Large-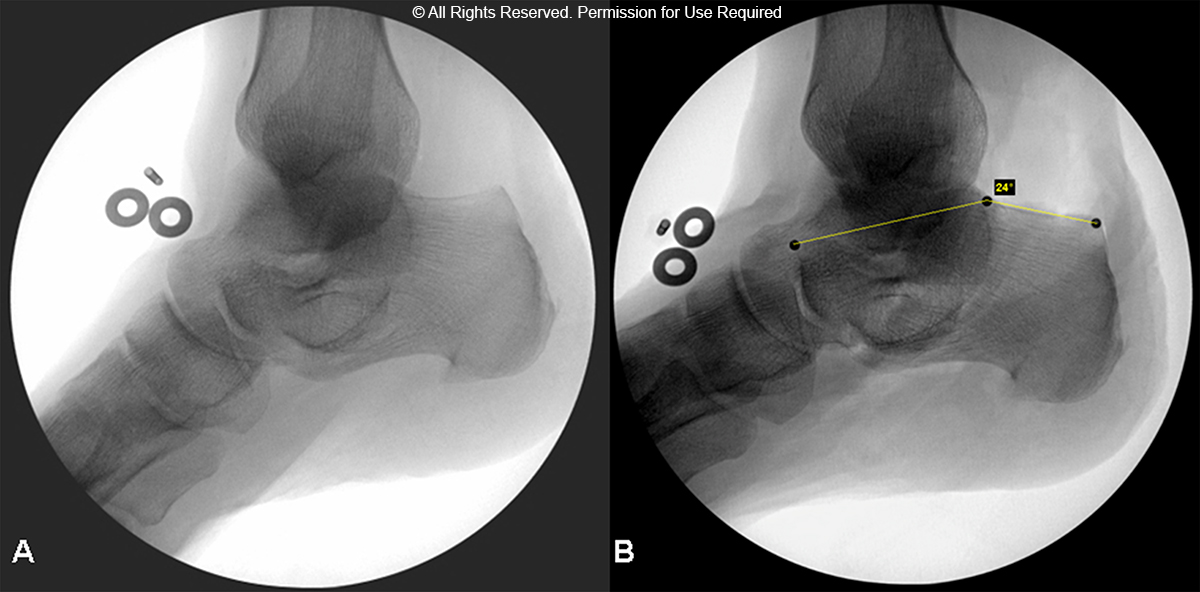{kind=link}
An independent statistician entered all data into a statistical database (SPSS v.19.0, © SPSS Inc., Chicago, IL) for analysis. Descriptive statistics were computed to provide an overall summary of the study sample. For all analyses, a p-value < 0.05 was considered significant.
Results
Observed Bohler’s Angles
For all study participants, the observed Bohler’s angles were significantly different from the control value for all images except for the oblique image in which the x-ray beam was directed 20 degrees posteriorly (p = 0.43). Anteriorly and caudally directed oblique images resulted in observed Bohler’s angles that were lower than control values. Posterior and cephalad oblique images resulted in observed Bohler’s angles that were greater than control values (Table 1), (Figures 3, 4).
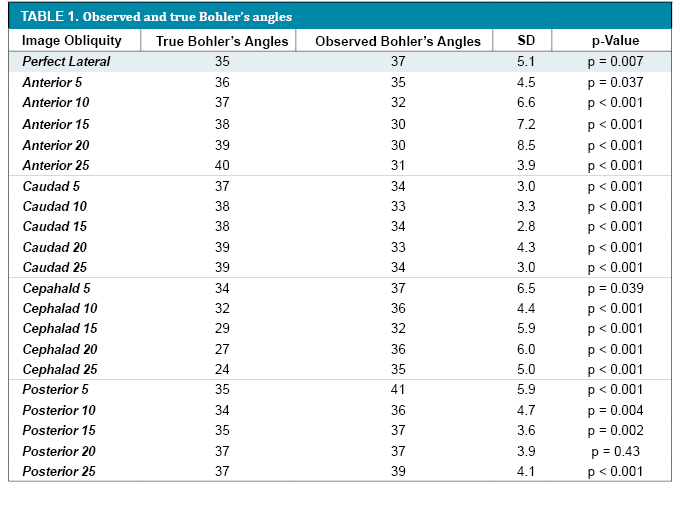
p-Values < 0.05 are statistically significant. Image obliquity, true Bohler’s angle and observed Bohler’s angle values are listed in degrees. True Bohler’s angles represent the mean of the three authors’ measurements. The interobserver correlation was excellent, ICC = 0.985 (p < 0.001). Observed Bohler’s angles are listed as the mean value of all observers. SD = standard deviation.
-View Large-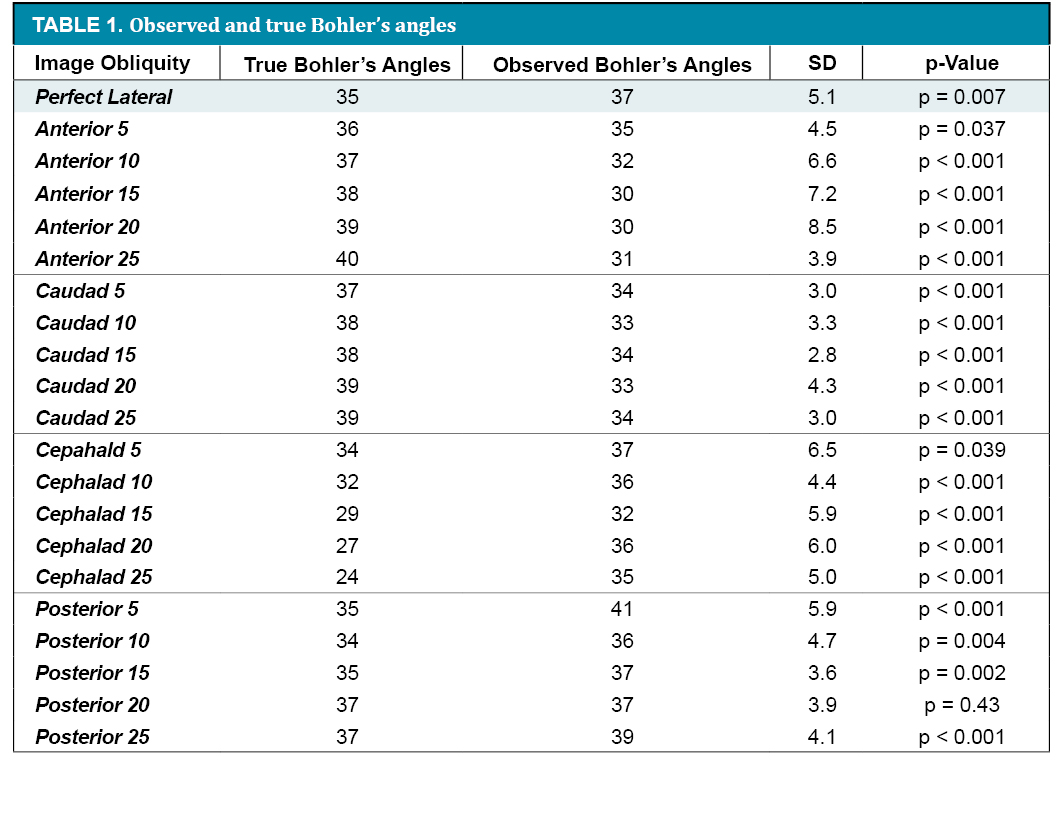{kind=link}
True Bohler’s Angles
The true Bohler’s angle measured on the perfect lateral image was determined to be 35 degrees. The true Bohler’s angle was found to increase with increasing obliquity as the x-ray beam was directed anteriorly and caudally, whereas the angle remained relatively constant when directed posteriorly. The true Bohler’s angle decreased as the x-ray beam was directed cephalad. With increasing obliquity, the difference between the true Bohler’s angle on the perfect lateral and oblique laterals was found to be smallest in the posterior direction (Figures 3, 4).
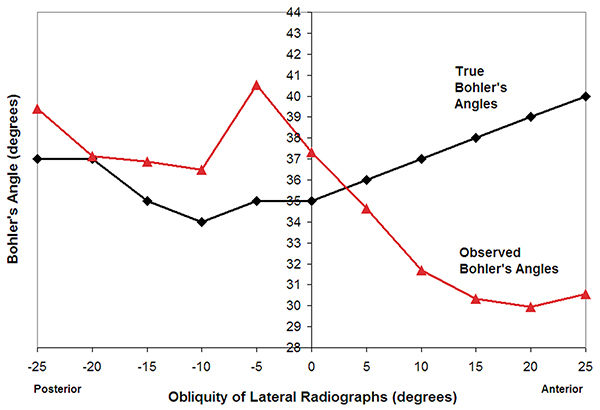
Observed and true Bohler’s angles with changes in the obliquity of lateral radiographs in the anterior (positive values on x-axis) and posterior (negative values on x-axis) directions.
All Rights Reserved. Permission For Use Required.
-View Large-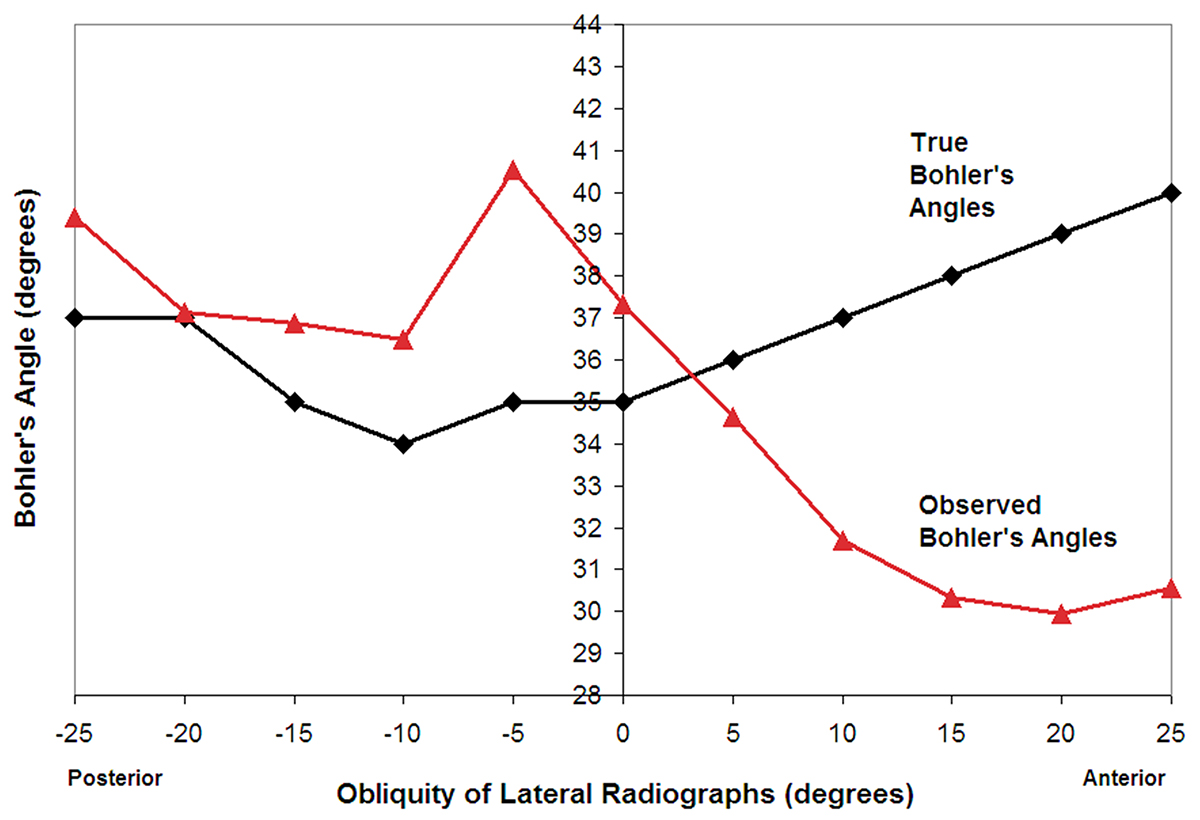{kind=link}
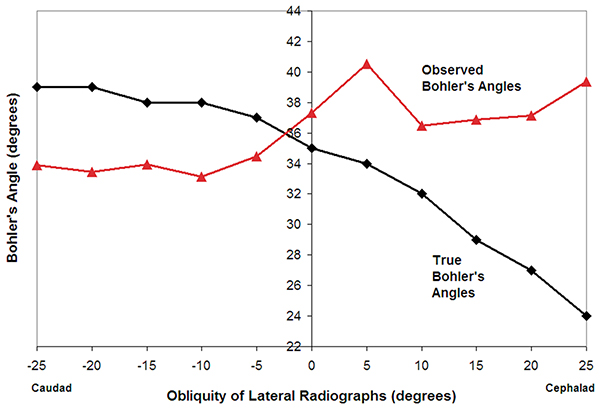
Observed and true Bohler’s angles with changes in the obliquity of lateral radiographs in the cephalad (positive values on x-axis) and caudad (negative values on x-axis) directions.
All Rights Reserved. Permission For Use Required.
-View Large-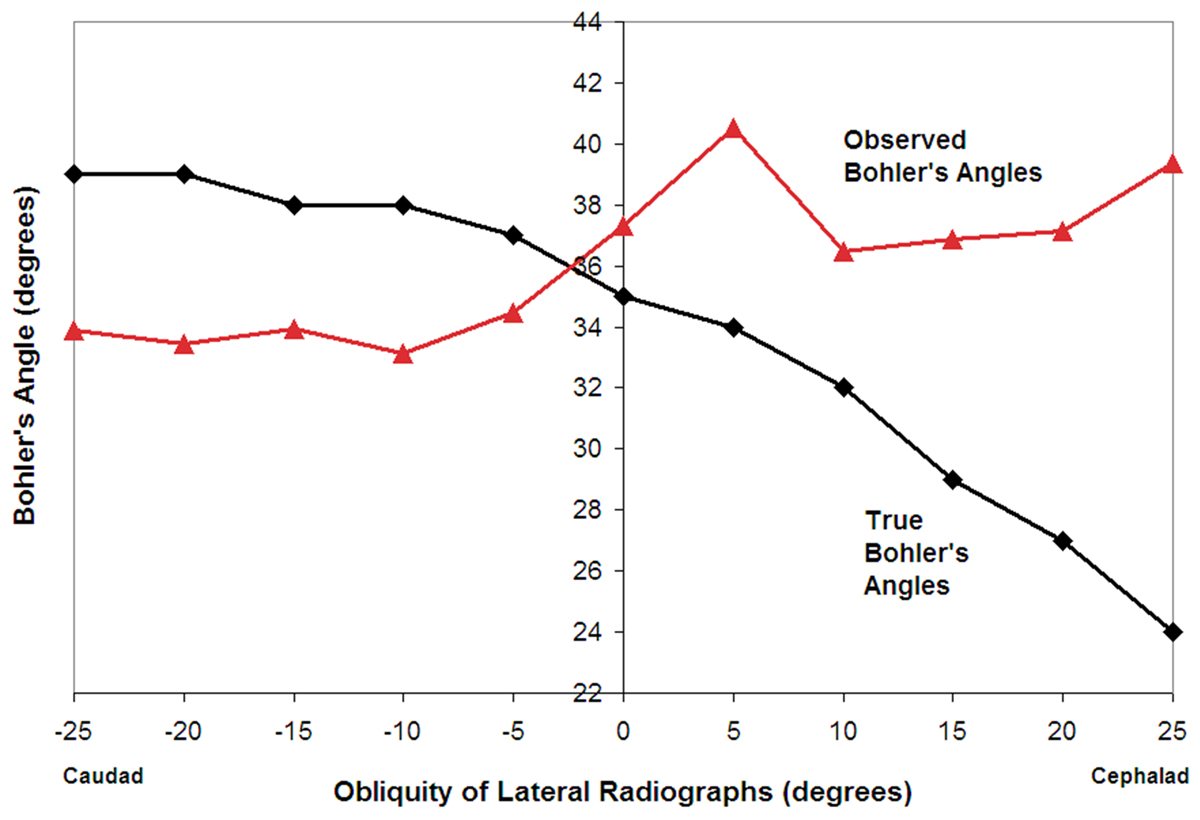{kind=link}
There was no significant difference between the true Bohler’s angle values for the three authors. The agreement between the authors was excellent with an ICC of 0.985 (p < 0.001) for the mean of the true Bohler’s angles.
Discussion
Observed Bohler’s Angles
The study findings highlight the difficulty of accurately measuring Bohler’s angle on oblique images. The results also highlighted that the true Bohler’s angle varied based on the obliquity of the lateral fluoroscopic image. These findings are notable given that in the trauma setting, oblique lateral radiographs are often the norm due to difficulties in proper positioning of the traumatized extremity or limitations from splint materials. Numerous papers direct clinicians to the importance of Bohler’s angle as a prognostic indicator for patient outcomes.4, 3, 10 The randomized controlled study performed by Buckley et al. in 2002 suggests that anatomic or near anatomic reduction has a positive effect on patient outcomes.4 Buckley and Meek in 1992 demonstrated that malreduced intra-articular fractures fared no better than those treated nonoperatively.3 An accurate assessment of Bohler’s angle and displacement of the posterior facet will avoid the over- or under-treatment of calcaneus fractures.
Observed Bohler’s Angles
As demonstrated in Table 1, there was a statistically significant difference for nearly all oblique images obtained, including the perfect lateral image. Willmott et al. showed that Bohler’s angle has good interobserver reliability and can be easily measured on a plain lateral radiograph.15 Clint et al. also demonstrated excellent interobserver agreement in assessing Bohler’s angle in children.5 The work done by Willmott et al. and Clint et al., suggests that high quality lateral radiographs are needed to confidently estimate Bohler’s angle, and accurately detect posterior facet displacement.
Our findings further illustrate that suboptimal imaging in the form of oblique hindfoot lateral x-rays will result in inaccurate calculation of Bohler’s angle. The inability of the study participants to accurately measure Bohler’s angle was a result of several factors. Oblique radiographs change the relationship between the three anatomic landmarks used to measure Bohler’s angle, the anterior calcaneal process, the superior most portion of the posterior facet and the posterior superior tuberosity. A “flattening” of the posterior facet appears to occur with x-rays directed cephalad, whereas this relationship is reversed in the caudal and anteriorly directed x-rays. Oblique radiographs result in the three anatomic landmarks not easily visualized “en face” as would be expected in the perfect lateral x-ray. Instead, a double shadow of the landmarks is seen rendering it difficult for clinicians to estimate Bohler’s angle.
True Bohler’s Angles
As previously noted, the true Bohler’s angle was found to vary based on the obliquity of the lateral fluoroscopic image, which is in direct contrast to the results of Malissard et al. In their study, Malissard et al demonstrated that Bohler’s angle was constant despite an obliquity of up to 15 degrees in all planes.11 Our findings suggest that Bohler’s angle does indeed vary with a difference of up to 6 degrees when the x-ray beam is directed 15 degrees cephalad. This difference is increased to 11 degrees when the x-ray beam is directed 25 degrees cephalad. However even considering this information, the data still show that Bohler’s angle does not vary significantly with posteriorly directed oblique radiographs – only a two-degree change with 25-degree oblique laterals. This would imply that although posteriorly directed oblique images may be acceptable, clinicians should avoid oblique radiographs in the cephalad direction.
The results of our study should be interpreted in the following context: There were only 41 participants (five attending orthopaedic physicians and 36 orthopaedic residents in all levels of training) involved. A broader sample size of participants may change the direction of the results.
Conclusion
The study findings reveal that orthopaedic surgeons’ ability to accurately measure Bohler’s angle significantly decreases with increasing obliquity of lateral radiographs. In addition, the true Bohler’s angle varies most with increasing obliquity in the cephalad direction, but less so with posteriorly directed x-rays. Although perfect hindfoot laterals are ideal, posteriorly directed oblique images may be acceptable. Oblique lateral radiographs in the cephalad direction should be avoided. Surgeons should be aware of variations in true Bohler’s angle, as well as difficulties with accurately measuring this angle with oblique lateral x-rays when evaluating patients with intra-articular calcaneus fractures. Understanding these subtle changes should enable surgeons to more carefully interpret data obtained from oblique lateral radiographs, both when deciding upon the need for CT and/or when determining operative versus nonoperative treatment based solely on Bohler’s angles.
References
